Leg Leiomyoma in Male Patients: A Report of Two Cases
Abdullah Zaher, Louise-Marie Mboua Tetka, Aïcha Ben Lakhdar, Noureddine Sekkach

TL;DR
Two male patients had rare leg leiomyomas, benign tumors typically found in the uterus, diagnosed only after surgery since imaging failed to identify them.
Contribution
The paper reports two rare cases of leg leiomyoma in male patients, highlighting diagnostic challenges and the importance of histologic analysis.
Findings
Leiomyoma and angioleiomyoma were confirmed in two male patients via histology after radiologists failed to diagnose the masses.
Surgical excision was the effective treatment for both cases, providing immediate symptom relief.
Leg leiomyoma is uncommon in men, and clinicians should consider it when evaluating soft tissue lumps despite diagnostic difficulties.
Abstract
Leiomyomas, benign smooth muscle tumors, are most frequently found in the uterus. Leg leiomyoma has been reported in a small number of studies, making it an uncommon finding. We present two male patients who came to the clinic with bothersome masses in their calf and knee, respectively. The radiologists could not diagnose these masses during the preoperative workup. According to pathology reports, the masses that were surgically removed were leiomyoma in one patient and angioleiomyoma in the other. Clinicians should consider leiomyoma when looking at soft tissue lumps, even though it's rare for men to have this condition in those areas. Clinical and radiographic confirmation of the diagnosis is challenging. However, a histologic analysis can support the diagnosis. The preferred course of treatment that provides instant symptom alleviation is surgical excision.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
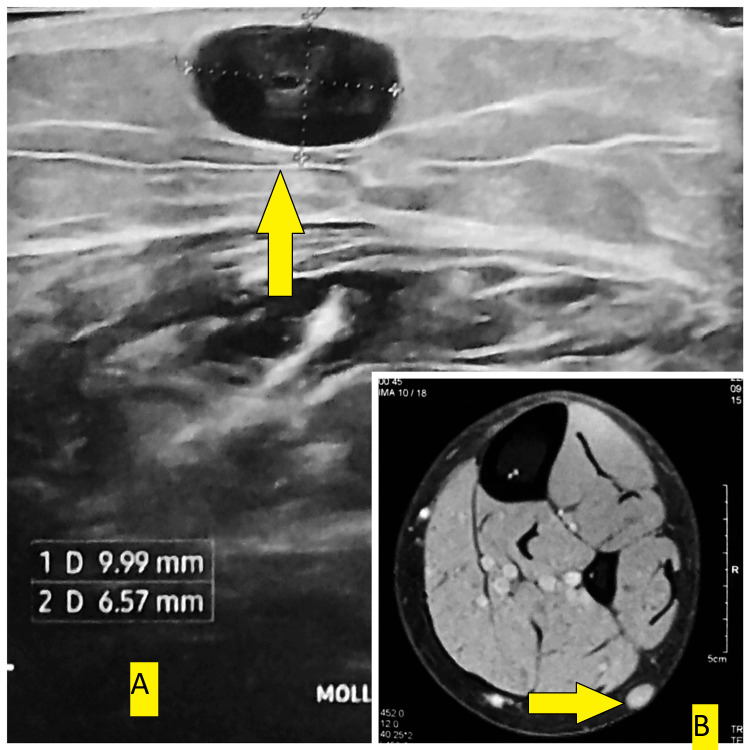 Figure 1
Figure 1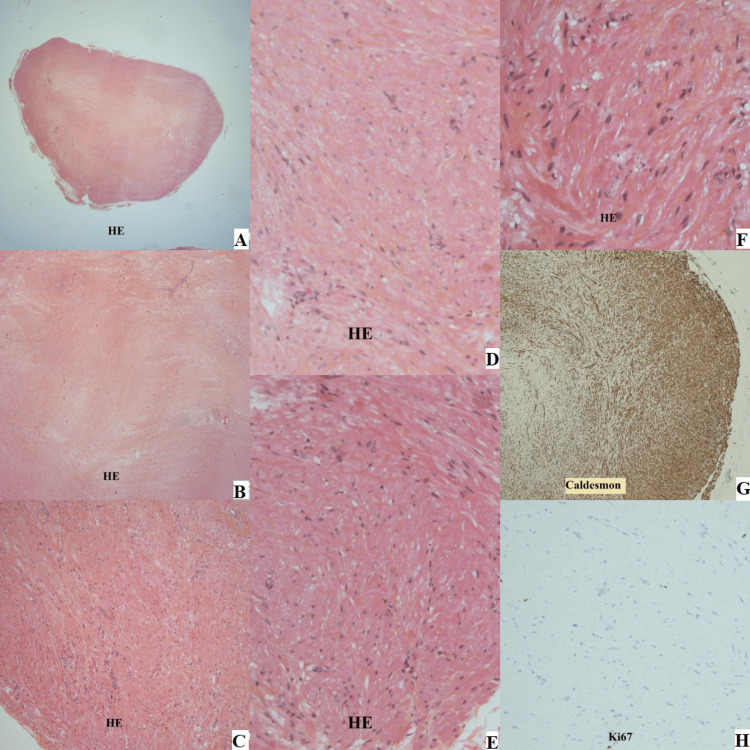 Figure 2
Figure 2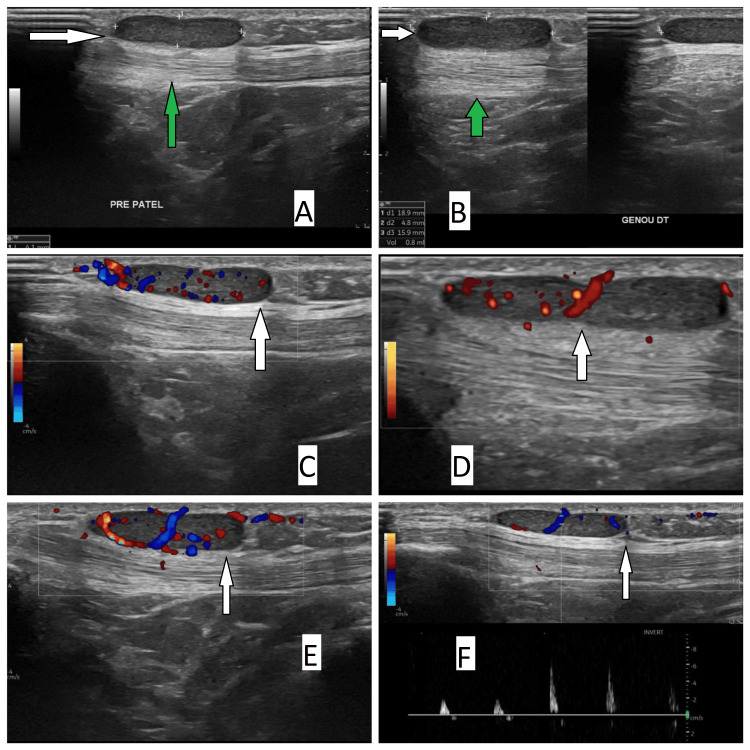 Figure 3
Figure 3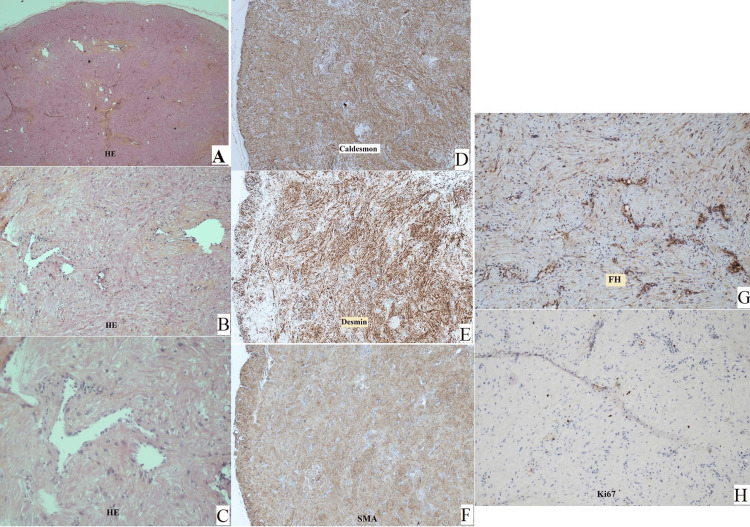 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSoft tissue tumors and treatment · Uterine Myomas and Treatments · Soft tissue tumor case studies
Introduction
Benign smooth muscle tumors, known as leiomyomas, are mostly found in the uterus, impacting about 80% of women [1]. However, they may develop in other areas with smooth muscle, like the gastrointestinal tract [2]. The incidence of leiomyomas at the extremity level is higher in the lower extremities than in the upper extremities, although there is little evidence of these cases in the literature [3]. Based on the tissue of origin, leiomyomas can be further classified into three subtypes: genital leiomyomas, piloleiomyomas, and angioleiomyomas. The most prevalent subtypes of leiomyoma, angioleiomyomas and piloleiomyomas, can develop over the extremities [4].
Angioleiomyoma (also called vascular leiomyoma) arises from the muscular layer of the vessel wall. The most typical manifestation is a solid, painful swelling beneath the skin. Approximately 5% of all soft tissue tumors are angioleiomyomas [5]. Its subcutaneous location at the knee joint is rare, as is its location in the lower limbs [6]. It is more prevalent in women in third and sixth decades of their lives. Pregnancy, hormonal changes, infection, and traumatic venous congestion can be among the causes of vascular leiomyoma [7]. Since leiomyoma is an extremely uncommon diagnosis, a list of differential diagnoses can be made when a patient arrives at the clinic with any lower limb mass without mentioning leiomyoma as a potential diagnosis [3]. The diagnosis of leiomyomas is mostly based on histological characteristics because of their rarity and nonspecific clinical nature. This case report details the uncommon finding in two male patients who had two distinct leiomyoma subtypes removed from their legs.
Case presentation
Case 1
The first patient was a healthy 31-year-old male who had a left calf mass that had been there for more than five years. According to the patient, the lump was smaller at first but has since slightly increased in size. He claimed that the contact irritates him, especially since he began participating in martial arts sports. He denied having related neurovascular symptoms when questioned. A green pea-sized, non-tender mid-calf mobile lump was palpable on the lateral side during physical examination. No distal neurovascular signs were present.
On his initial visit, the patient brought an echography report that described a 10x5.6 mm subcutaneous lump on the lateral side, mid-height of the left leg, with central vascularization. According to the radiologist, the diagnosis was most consistent with adenopathy. An MRI was required to confirm the presence of a small non-specific subcutaneous nodule on the posterior calf measuring 9x6.6x1 mm, which is compatible with a cystic formation (Figure 1).
Preoperative scans of the first patientPreoperative echography (A) and MRI (B) images, with arrows marking the mass of interest.
The patient was scheduled for surgical excision of this mass. During surgery, the mass was found just beneath the skin, easily excised, and sent for pathological analysis. With no indications of malignancy, the pathology report validated the histological diagnosis of leiomyoma (Figure 2).
Histopathological study images (patient one)Histological slides of the excised tumor prepared with different stains (A, B, C, D, E, F prepared with hematoxylin-eosin (HE); G prepared with caldesmon stain and H was ki67 marker stained ).
Following surgery, the patient was seen at the clinic one month following the mass's removal. The patient's scar has healed. He was questioned and found to have no family history of uterine fibroids or malignancy, renal cell carcinoma, or other cancers. At the end of the visit, oral consent to publish the case was done.
Case 2
The second patient was a 48-year-old healthy man who presented with a mass in his right knee, which started appearing two years ago. The mass was localized to the anterior part of the knee just below the kneecap. It bothered him and was sometimes painful, yet it did not change in size with time. The lump was felt directly in front of the patellar tendon during the physical examination. It was spherical and about 1 cm in diameter.
An echography was requested that revealed a well-defined, 4x17 mm pre-patellar subcutaneous mass that was vascularized on Doppler (Figure 3). The radiologist's differential diagnosis included vascular malformation or peripheral nerve tumor.
Preoperative scans of the second patient Preoperative echography (A, B) and echo-Doppler (C, D, E, F) images (white arrow: the mass, green arrow: the patellar tendon).
Surgical excision was programmed. The mass was easily excised and sent to pathological analysis. The pathology report confirmed the histological diagnosis of angioleiomyoma with no indications of malignancy (Figure 4).
Histopathological study images (patient two) Histological slides of the excised tumor prepared with different stains (A, B, and C prepared with hematoxylin-eosin (HE) stain, D caldesmon stain, E desmin stain, F smooth muscle actin (SMA) stain, G fumarate hydratase (FH) stain, and H ki67 marker stain.
Following surgery, the patient was seen at the clinic one month after the mass was removed. The patient's scar has healed. He was questioned again about his personal history of medical problems. He denied having any medical problems or any family history of malignancy. Before leaving the clinic, oral consent was obtained to publish the case.
Discussion
Leiomyomas are benign tumors made of smooth muscle, mostly found in the uterus and digestive system. Cutaneous leiomyomas can be divided into three types: angioleiomyomas, piloleiomyomas, and genital leiomyomas. Angioleiomyomas and piloleiomyomas are the most common types of cutaneous leiomyomas, and they can show up on the arms and legs [4]. However, some studies showed variable distribution of these tumors with lower limbs affected in 9.3-43.4% of the cases [8].
These tumors, when located in the limbs, exhibit the same nonspecific symptoms as more common masses like lipomas and epidermoid cysts. The symptoms can vary depending on the location, size, and type of each mass. Additionally, paraclinical findings, such as ultrasound and MRI results, are often similar across these different types of masses. Clinical suspicion and diagnosis of such findings are difficult due to their rarity and lack of a diagnostic method to confirm the diagnosis other than histopathological examination [4].
Angioleiomyomas, also called angiomyomas or vascular leiomyomas, arise from the tunica media of veins. They make up 5% of all benign tumors in soft tissues. Factors like minor injuries, blood flow problems, and hormonal changes, especially estrogen, may affect their development. They are the type of cutaneous leiomyoma that most often appears in the extremities, with 60% presenting in the lower extremity below the thigh [9]. Typically, they show up as a small lump (usually less than 20 mm), and more than half of cases present with pain or tenderness. Most cases (around two-thirds) occur in people aged 40 to 60, and they are more common in women (2:1 ratio) [10].
In our second case, we reported a male patient in his fourth decade of life who manifested with a painful mass that was located just below the patella. Upon reviewing the literature, we found a similar case of a female patient of the same age presenting with a 0.5 cm nodule just below her kneecap that was eventually excised and turned out to be an angioleiomyoma [11].
Unlike angioleiomyomas, piloleiomyomas, also called pilar leiomyomas, come from the arrector pili muscle of the hair follicle. They often appear as firm, rounded nodules. Unlike angioleiomyomas, piloleiomyomas are usually not as painful. They typically develop in adolescents and younger adults, affecting both men and women equally [12]. In our first case, our patient was a young male presenting with a non-painful mass in his calf that was removed surgically and found to be a leiomyoma on microscopic analysis.
While reviewing the literature, there exists a syndrome of hereditary leiomyomatosis and renal cell cancer, also known as Reed’s syndrome. It is a rare autosomal dominant disorder caused by a mutation in the fumarate hydratase, a tumor suppressor gene, leading to an accumulation of fumarate. This syndrome is associated with benign smooth muscle tumors and an increased risk of renal cell carcinoma. In females, it is characterized by the presence of superficial leiomyomas besides uterine leiomyomas [13]. Thus, in the case of the presence of cutaneous leiomyomas, a clinician should be aware of this condition. The definitive diagnosis is made by genetic testing confirming the gene mutation [14]. However, there are certain diagnostic criteria that raise clinical suspicion for this syndrome. Major criteria include the finding of multiple skin lesions proven to be leiomyomas in at least one specimen, whereas the minor criteria consist of the discovery of a solitary cutaneous leiomyoma and family history of hereditary leiomyomatosis and renal cell carcinoma, early-onset renal papillary tumor, and multiple early-onset symptomatic uterine fibroids.
In our cases, none of the two patients was classified as having Reed's syndrome, as each had only one nodule, which was diagnosed as a cutaneous leiomyoma. In addition to this finding, which is considered a minor criterion, none of the other criteria applied to our patients. With respect to the treatment of these tumors, surgical excision leads to the absolute resolution of the symptoms, as shown in our cases.
Conclusions
In summary, even though leiomyomas are not commonly found in the legs, they should still be considered in the list of the differential diagnosis of masses of lower extremities. Confirmation of the diagnosis is only achieved by having a microscopic analysis of such tumors. This means that removing the tumor through surgery helps not only in treating a patient’s symptoms but also in aiding in the diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Serum dioxin concentrations and risk of uterine leiomyoma in the Seveso Women's Health Study Am J Epidemiol Eskenazi B Warner M Samuels S 798716620071744302310.1093/aje/kwm 048 · doi ↗ · pubmed ↗
- 2From the radiologic pathology archives: esophageal neoplasms: radiologic-pathologic correlation Radiographics Lewis RB Mehrotra AK Rodriguez P Levine MS 108311083320132384297310.1148/rg.334135027 · doi ↗ · pubmed ↗
- 3Unusual presentation of leiomyoma in the hindfoot Case Rep Orthop Zaher A Yasser J Badaro D Sekkach N 1217277202420243851661310.1155/2024/1217277 PMC 10957246 · doi ↗ · pubmed ↗
- 4Leiomyoma of the foot: a case report Cureus Buddemeyer K Mc Kissack HM Farnell C 010201810.7759/cureus.3419 PMC 628487130542633 · doi ↗ · pubmed ↗
- 5Angioleiomyoma. A clinicopathologic reappraisal of 562 cases Cancer Hachisuga T Hashimoto H Enjoji M 126130541984672273710.1002/1097-0142(19840701)54:1<126::aid-cncr 2820540125>3.0.co;2-f · doi ↗ · pubmed ↗
- 6Angioleiomyoma of the knee: an uncommon cause of leg pain. A systematic review of the literature Interdisciplinary Neurosurgery Montemurro N Ortenzi V Naccarato GA Perrini P 100877122020
- 7Clinical and histological features of vascular leiomyoma of the foot: case report and literature review Foot Ankle Surg Santucci A Albini M Ventura A De Palma L 26727462000
- 8Cutaneous leiomyoma of the leg: a case report and literature review Sierra Leone J Med Omoke NI Aniume OI Nwigwe CG Utah FU 444612024 https://sljm.org/journal/index.php/sljm/article/view/83