Two Japanese Cases of Breast Cancer That Developed Pembrolizumab-Induced Adrenal Insufficiency and Literature Review
Yuka Ozawa, Takaaki Tokito, Mariko Kikuchi, Hiroshi Katoh, Takafumi Sangai

TL;DR
This paper reports two cases of adrenal insufficiency caused by pembrolizumab in breast cancer patients and highlights the importance of early detection using CTCAE grading.
Contribution
The study adds to the understanding of pembrolizumab-induced adrenal insufficiency through real-world case reports and emphasizes early detection methods.
Findings
Two Japanese breast cancer patients developed adrenal insufficiency during pembrolizumab treatment.
Symptoms improved after hydrocortisone treatment, confirming the diagnosis of pembrolizumab-induced adrenal insufficiency.
CTCAE grading showed clear changes in adverse event severity, aiding early detection of adrenal insufficiency.
Abstract
We report two cases of adrenal insufficiency (AI) occurring during neoadjuvant treatment with pembrolizumab for breast cancer. In the first case, a 53-year-old female presented with a chief complaint of poor oral intake and fatigue. In the second case, a 46-year-old female presented with a chief complaint of fever, poor oral intake, and general fatigue and was admitted with a diagnosis of pneumonia. Her symptoms did not improve during treatment for pneumonia. After that, two patients were diagnosed with pembrolizumab-induced adrenal insufficiency and were treated with hydrocortisone with improvement in their symptoms. AI due to pembrolizumab use is a relatively rare adverse event, but if it is detected late, it can be potentially life-threatening. In both cases, there were clear changes in the common terminology criteria for adverse events (CTCAE) grade at the time of diagnosis of AI.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
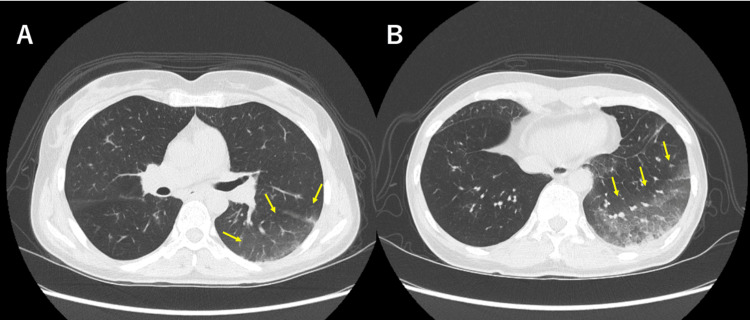 Figure 1
Figure 1| Laboratory Test | Result at the first visit | Result when diagnosed with AI | Reference Range |
| White Blood Cell | 5.4 *103/µL | 4.5 *103/µL | 3.3-8.6 *103/µL |
| Neutrophil | 52.9% | 45.3% | 50-70 % |
| Eosinophil | 3.0% | 0.9% | 2.0-5.0 % |
| Red Blood Cell | 4.3 *106/µL | 3.3 *106/µL | 3.86-4.92 *106/µL |
| Hemoglobin | 12.9 g/dL | 10.8 g/dL | 11.6-14.8 g/dL |
| Platelet | 34.6 *104/µL | 42.1 *104/µL | 15.8-34.8 *104/µL |
| Protein | 7.2 g/dL | 6.5 g/dL | 6.6-8.1 g/dL |
| AST | 16 U/L | 22 U/L | 13-30 U/L |
| ALT | 14 U/L | 13 U/L | 7-23 U/L |
| Creatinin | 0.91 mg/dL | 0.73 mg/dL | 0.46-0.79 mg/dL |
| Sodium | 144 mmol/L | 140 mmol/L | 138-145 mmol/L |
| Potassium | 3.8 mmol/L | 3.6 mmol/L | 3.6-4.8 mmol/L |
| CRP | 0.06 mg/dL | 0.13 mg/dL | <0.14 mg/dL |
| Glucose | 84 mg/dL | 113 mg/dL | 73-109 mg/dL |
| TSH | 0.7 µIU/mL | 14.1 µIU/mL | 0.5-5.0 µIU/mL |
| FT3 | 2.78 pg/mL | 2.54 pg/mL | 2.3-4.0 pg/mL |
| FT4 | 1.35 ng/dL | 0.88 ng/dL | 0.9-1.7 ng/dL |
| ACTH | 31.8 pg/mL | <2.0 pg/mL | 7.2-63.3 pg/mL |
| Cortisol | 17.8 µg/dL | 0.32 µg/dL | 7.07-19.6 µg/dL |
| Laboratory Test | Result at the first visit | Result at the time of hospitalization | Reference Range |
| White Blood Cell | 5.4 *103/µL | 13.7 *103/µL | 3.3-8.6 *103/µL |
| Neutrophil | 46% | 44% | 50-70 % |
| Eosinophil | 18% | 48% | 2.0-5.0 % |
| Red Blood Cell | 4.31 *106/µL | 4.45 *106/µL | 3.86-4.92 *106/µL |
| Hemoglobin | 11.7 g/dL | 13.5 g/dL | 11.6-14.8 g/dL |
| Platelet | 32.6 *104/µL | 22.9 *104/µL | 15.8-34.8 *104/µL |
| Protein | 6.6 g/dL | 6.1 g/dL | 6.6-8.1 g/dL |
| AST | 32 U/L | 26 U/L | 13-30 U/L |
| ALT | 27 U/L | 19 U/L | 7-23 U/L |
| Creatinin | 0.73 mg/dL | 0.47 mg/dL | 0.46-0.79 mg/dL |
| Sodium | 140 mmol/L | 126 mmol/L | 138-145 mmol/L |
| Potassium | 4.2 mmol/L | 3.8 mmol/L | 3.6-4.8 mmol/L |
| CRP | <0.03 mg/dL | 2.44 mg/dL | <0.14 mg/dL |
| Glucose | 137 mg/dL | 113 mg/dL | 73-109 mg/dL |
| TSH | 2.09 µIU/mL | 3.88 µIU/mL | 0.5-5.0 µIU/mL |
| FT3 | 2.64 pg/mL | 4.07 pg/mL | 2.3-4.0 pg/mL |
| FT4 | 1.3 ng/dL | 1.77 ng/dL | 0.9-1.7 ng/dL |
| ACTH | 41.8 pg/mL | <2.0 pg/mL(*) | 7.2-63.3 pg/mL |
| Cortisol | 8.51 µg/dL | <0.2 µg/dL(*) | 7.07-19.6 µg/dL |
| Case No. | Age | Sex | Site of primary tumor | Stage IV Y/N | Drug types | Symptoms that led to the diagnosis | Reference |
| 1 | 52 | M | Lung | Y | CBDCA+PEM+Pembrolizmab | Fatigue | * |
| 2 | 54 | M | Lung | N | Pembrolizumab | Fatigue | [ |
| 3 | 77 | M | Colon | Y | Pembrolizumab | Fatigue, poor appetite, and dry mouth | [ |
| 4 | 87 | F | Colon | Y | Pembrolizumab | Poor appetite, shortness of breath, and depression | [ |
| 5 | 75 | M | Skin | Y | Pembrolizumab | Fatigue and poor appetite | [ |
| 6 | 70 | M | Lung | Y | Pembrolizumab | Fatigue and fever | [ |
| 7 | 59 | M | Lung | Y | Pembrolizumab | Fatigue (Grade 2) | [ |
| 8 | 72 | M | Lung | N | Pembrolizumab | Fatigue, poor appetite and diarrhea | [ |
| 9 | 74 | M | Renal pelvis | N | Pembrolizumab | Fatigue and poor appetite | [ |
| 10 | 78 | M | Renal pelvis | N | Pembrolizumab | Fatigue | [ |
| 11 | 70 | M | Ureter | Y | Pembrolizumab | Fatigue and poor appetite | [ |
| 12 | 79 | M | Lung | Y | Pembrolizumab | Consciousness disturbance | [ |
| 13 | 53 | F | Breast | N | Pembrolizumab+CBDCA+PTX→Pembrolizumab+EC | Fatigue and poor appetite (Grade 2) | Our case 1 |
| 14 | 46 | F | Breast | N | Pembrolizumab+CBDCA+PTX→Pembrolizumab+EC | Fatigue and poor appetite (Grade 2) | Our case 2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Colorectal Cancer Treatments and Studies · Adrenal Hormones and Disorders
Introduction
Recurrence and metastasis of triple-negative breast cancer (TNBC) are associated with poor prognosis, making the initial treatment aimed at controlling potential microscopic metastases through local and systemic therapies extremely important. The KEYNOTE-522 trial demonstrated that the addition of pembrolizumab significantly improved pathological complete response rates and event-free survival [1], leading to the use of pembrolizumab, an anti-PD-1 (Programmed cell Death-1) antibody, as neoadjuvant and adjuvant immunotherapy for high-risk early TNBC. Currently, pembrolizumab is used for many malignancies, such as lung cancer, urothelial carcinoma, and malignant melanoma, in addition to breast cancer. On the other hand, immune-related adverse events (irAEs) associated with pembrolizumab have been reported, and endocrine disorders, such as adrenal insufficiency (AI), which can be fatal, are one of the irAEs that should be monitored closely [2]. In the two cases we encountered, one presented with typical symptoms, allowing for early diagnosis and treatment intervention, while the other exhibited various symptoms, making diagnosis difficult. With this case report, we aim to contribute to the growing body of evidence and raise awareness among clinicians.
Case presentation
Case 1
In the first case, a 53-year-old female with no significant past medical history noticed a lump in her right breast. She was diagnosed with right breast cancer (Invasive ductal carcinoma, Triple negative type, cT2N0M0 cStageIIA) and started neoadjuvant chemotherapy and immunotherapy. After the first cycle of pembrolizumab, carboplatin, and paclitaxel, the laboratory data showed hyperthyroidism and then hypothyroidism at the time of the third cycle. She was administered Levothyroxine. She also started complaining of nausea and mild shortness of breath, but both were considered Grade 1. Following her second cycle of pembrolizumab, epirubicin, and cyclophosphamide, she experienced worsening appetite loss and general fatigue (Grade 2). She was suspected of secondary AI and underwent a laboratory test (Table 1).
As demonstrated in Table 1, the patient's adrenocorticotropic hormone (ACTH) and cortisol levels were significantly below the normal reference range, a key indicator of adrenal insufficiency. This finding, coupled with clinical symptoms, confirmed the diagnosis of pembrolizumab-induced AI. She was administered a physiological maintenance of hydrocortisone 15mg; her symptoms significantly improved the next day. After that, computerized tomography (CT) and magnetic resonance imaging (MRI) scans showed a clinical complete response (cCR), so pembrolizumab was not resumed. Instead, she underwent a right total mastectomy and sentinel lymph node biopsy. Postoperative pathology revealed no residue of malignancy. Currently, she is receiving pembrolizumab again while taking hydrocortisone.
Case 2
In the second case, a 46-year-old female with no significant past medical history was referred for further evaluation following a screening ultrasound. She was diagnosed with left breast cancer (Invasive ductal carcinoma, Triple negative type, cT2N0M0, cStage IIA) and started neoadjuvant chemotherapy and immunotherapy. After the introduction of pembrolizumab, carboplatin, and paclitaxel, she started complaining of nausea and fatigue, which were equivalent to Grade 1. After the first cycle of pembrolizumab, epirubicin, and cyclophosphamide, her symptoms worsened (Grade 2), and she developed a fever, so she was hospitalized (Table 2).
At the time of hospitalization, she had a productive cough and required low-dose oxygen. A chest CT scan revealed a ground-glass opacity in the dorsal segment of the left upper lobe (Figure 1A) and an infiltrative shadow in the dorsal segment of the left lower lobe (Figure 1B).
Chest CT scan
She was suspected of bronchopneumonia based on these findings. No clear distant metastasis was observed. She was diagnosed with aspiration pneumonia and received antibiotic treatment. On day three of hospitalization, she continued to experience poor appetite and general fatigue. In addition to the poor response to antibiotic therapy and persistent findings of hyponatremia and eosinophilia on blood tests raised, she was suspected of secondary AI and underwent additional laboratory tests (Table 2). As demonstrated in Table 2, the patient's ACTH and cortisol levels were significantly below the normal reference range. This finding and clinical symptoms confirmed the diagnosis of pembrolizumab-induced AI. A pituitary MRI did not reveal any abnormality or lesion. She was administered a stress-dose glucocorticoid replacement for three days. She gradually tapered glucocorticoid and transitioned to a physiological maintenance dose of hydrocortisone 15mg, immediately improving her appetite and energy level. She was discharged on day eleven of admission. After that, CT and MRI scans showed a cCR, so pembrolizumab was not resumed. Instead, she underwent a left total mastectomy and sentinel lymph node biopsy. Postoperative pathology revealed an invasive residual disease (ypT1aN0).
Discussion
Currently, pembrolizumab is a therapeutic agent that binds to PD-1, which is involved in regulating autoimmune responses. This binding releases the brakes on the immune system by blocking inhibitory signals, reactivating T cells to increase their attack on tumors [3]. However, because it is a drug related to the body's autoimmune response, immune checkpoint inhibitors (ICIs) such as pembrolizumab can disrupt the normal regulation of the immune system, leading to the development of autoimmune diseases. These immune-related side effects are referred to as irAEs [4]. In fact, molecules involved in antigen presentation on T cells are expressed throughout the body so that irAEs can occur systemically. However, reports of these events are relatively more common in the skin, gastrointestinal tract, and endocrine system. There are several reports regarding the mechanisms of onset for some organs, such as the skin [5], thyroid [6], and pituitary gland [7-8]. However, there are no reports confirming the mechanisms of onset for adrenal cortical insufficiency.
Adrenal insufficiency as an irAE is observed in approximately 2.6% of patients receiving ICI treatment, making it a relatively rare adverse event [1]. Clinical symptoms of AI include fever, fatigue, and gastrointestinal symptoms. However, cases that reach grade 3 or higher are rare, occurring in approximately 1.0% of patients [1]. A search on the Japanese medical database Ichushi Web using the keywords "Pembrolizumab" and "adrenal cortical insufficiency" yielded 20 relevant articles. All of the articles were related to lung cancer, urological malignancies, gastrointestinal cancers, and malignant melanoma, and no case reports related to breast cancer were found. Out of the 20 articles, 12 case reports described the symptoms that led to the discovery of adrenal cortical insufficiency [9-16,18,19]. The most commonly reported symptoms were fatigue (75%) and poor appetite (50%). One of these reports indicated that the severity of the symptoms was equivalent to Grade 2 (Table 3).
Additionally, cases with hyponatremia and eosinophilia were notable in the blood biochemical findings. Specifically, hyponatremia was observed in 10 out of 14 cases (71%; Grade 1/2/3/4, 3/0/6/1 cases, respectively). In fact, there are several studies suggesting that eosinophilia and hyponatremia are likely to be biomarkers indicative of AI [17].
In the two cases discussed, the CTCAE grade reached Grade 2 at the time of diagnosis of AI. There was a clear change in the grading of the symptoms following treatment. In the second case, pneumonia complicates the condition, which masks the typical symptoms of AI, leading to a delay in treatment intervention. If AI had been suspected at the stage when there was a change in the Grade and adrenal function tests had been added to the blood test, it is possible that treatment intervention could have been initiated at an earlier stage. Moreover, the blood tests at the time of hospitalization already showed eosinophilia and hyponatremia, and the biochemical findings suggested the possibility of AI.
In patients undergoing chemotherapy, side effects such as poor appetite and fatigue are commonly observed, which makes it possible to overlook AI caused by irAEs in clinical practice. As a trigger for suspecting AI, it is essential to carefully monitor changes in the severity of symptoms, reference the CTCAE grade, and conduct a more thorough patient interview to ensure timely recognition and appropriate management. Additionally, biochemical findings such as blood cell counts and electrolyte abnormalities can also help identify AI. Therefore, it is important to check these alongside the adverse symptoms to aid in early detection.
Conclusions
We presented two cases of pembrolizumab-induced adrenal insufficiency. AI can often be masked by the side effects of chemotherapy, making it important to monitor changes in CTCAE grade and biochemical findings closely. It is particularly crucial to suspect AI in cases of grade 2 or higher fatigue, poor oral intake, or hyponatremia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Event-free survival with pembrolizumab in early triple-negative breast cancer N Engl J Med Schmid P Cortes J Dent R 55656738620223513927410.1056/NEJ Moa 2112651 · doi ↗ · pubmed ↗
- 2Incidence of endocrine dysfunction following the use of different immune checkpoint inhibitor regimens: A systematic review and meta-analysis JAMA Oncol Barroso-Sousa R Barry WT Garrido-Castro AC Hodi FS Min L Krop IE Tolaney SM 173182420182897365610.1001/jamaoncol.2017.3064 PMC 5838579 · doi ↗ · pubmed ↗
- 3PD-1/PD-L 1 pathway: Current researches in cancer Am J Cancer Res Han Y Liu D Li L 727742102020 https://pubmed.ncbi.nlm.nih.gov/32266087/32266087 PMC 7136921 · pubmed ↗
- 4Managing immune checkpoint-blocking antibody side effects Am Soc Clin Oncol Educ Book Postow MA 768335201510.14694/Ed Book_AM.2015.35.7625993145 · doi ↗ · pubmed ↗
- 5Melan-A-specific cytotoxic T cells are associated with tumor regression and autoimmunity following treatment with anti-CTLA-4Clin Cancer Res Klein O Ebert LM Nicholaou T 250725131520091931847710.1158/1078-0432.CCR-08-2424 · doi ↗ · pubmed ↗
- 6Antibody-mediated thyroid dysfunction during T-cell checkpoint blockade in patients with non-small-cell lung cancer Ann Oncol Osorio JC Ni A Chaft JE 5835892820172799896710.1093/annonc/mdw 640PMC 5834017 · doi ↗ · pubmed ↗
- 7Pituitary expression of CTLA-4 mediates hypophysitis secondary to administration of CTLA-4 blocking antibody Sci Transl Med Iwama S De Remigis A Callahan MK Slovin SF Wolchok JD Caturegli P 2306201410.1126/scitranslmed.300800224695685 · doi ↗ · pubmed ↗
- 8Hypophysitis secondary to cytotoxic T-lymphocyte-associated protein 4 blockade: Insights into pathogenesis from an autopsy series Am J Pathol Caturegli P Di Dalmazi G Lombardi M 3225323518620162775004610.1016/j.ajpath.2016.08.020PMC 5225294 · doi ↗ · pubmed ↗