Acute Occlusion of a Persistent Sciatic Artery in a Patient with COVID-19 Infection
Daisuke Futagami, Taira Kobayashi, Hironobu Morimoto, Junya Kitaura, Shogo Mukai, Shinya Takahashi

TL;DR
A rare case of a blocked sciatic artery in a man with COVID-19 was successfully treated with surgery.
Contribution
This case report highlights a rare vascular complication of COVID-19 and its successful surgical management.
Findings
Acute occlusion of a persistent sciatic artery was diagnosed in a patient with COVID-19.
Conservative treatment failed, leading to toe necrosis.
Distal artery bypass successfully treated the condition.
Abstract
Persistent sciatic artery (PSA) is an exceptionally rare vascular condition that occurs in approximately 0.025%–0.04% of the general population. We describe the case of a 51-year-old man who presented with acute left lower limb pain and high fever. He was diagnosed with COVID-19 and isolated, and conservative treatment was performed for toe pain, resulting in left toe necrosis. Computed tomography revealed PSA occlusion in the left lower extremity. We diagnosed the patient with acute occlusion of the PSA due to COVID-19. The complicated disease was successfully treated using distal artery bypass.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1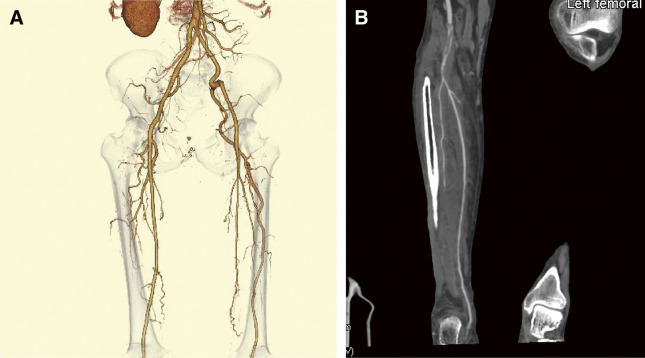 Figure 2
Figure 2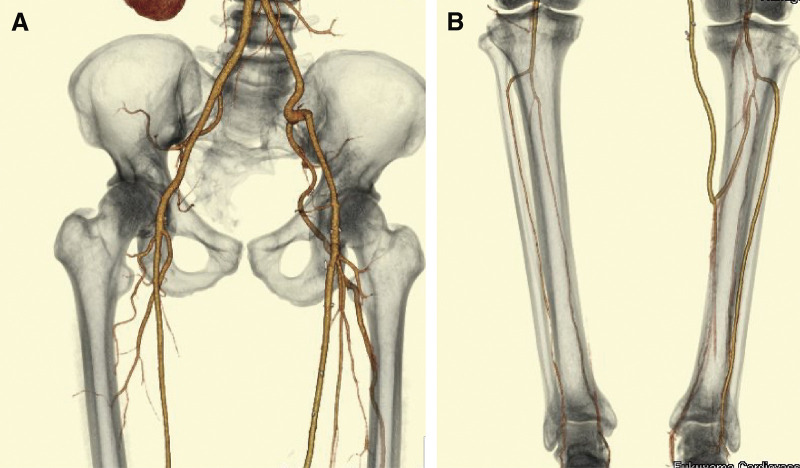 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Optic Conditions · Vasculitis and related conditions · Cerebral Venous Sinus Thrombosis
Introduction
The coronavirus disease 2019 (COVID-19) pandemic continues to spread worldwide. The major risk factors for morbidity and mortality in patients with COVID-19 are advanced age and comorbidities. In critically ill COVID-19 patients, prothrombotic coagulation disorders and thromboembolisms are common complications that contribute to increased morbidity and mortality. Patients with persistent sciatic artery (PSA) are more likely to experience symptomatic local thrombosis and distal embolization. Here, we report a case of acute thrombotic PSA without aneurysm formation following COVID-19.
Case Report
A 51-year-old man presented with sudden severe left toe pain and high-grade fever (temperature >39°C). COVID-19 was confirmed by PCR testing. Oxygen therapy was not required, and the chest X-ray showed no abnormalities. The patient was isolated for seven days. He had no significant medical history and was an active smoker. Conservative treatment for the toe pain led to necrosis of the left 5th toe. A minor amputation was performed by a previous physician. However, wound healing was not achieved. The laboratory findings were as follows: activated partial thromboplastin time (aPTT) 29.0 seconds, prothrombin time-international normalized ratio (PT-INR) 0.94, D-dimer 1.6 µg/mL, hemoglobin A1C (HbA1c) 5.3%, and blood glucose level 94 mg/dL.
Magnetic resonance angiography (MRA) was performed to diagnose vascular malformation and obstruction of the left popliteal artery, and he was admitted to our hospital. Electrocardiography (ECG) was a normal sinus rhythm. Computed tomography (CT) revealed no mobile plaques in the aortoiliac lesion.
Physical examination revealed necrosis of the first, second, and third toes, with no detectable pulses in the left popliteal, dorsalis pedis, or posterior tibial arteries (PTAs; Fig. 1). Heparin sodium was administered intravenously and maintained at 10000 units daily, and the ankle-brachial index (ABI) was 0.74 on the left. After 14 days, conservative treatment did not lead to improvement in the necrosis.
Fig. 1 Preoperative findings in the patient with partial necrosis of the first, second, and third toes and amputation of the fifth toe.
CT revealed left PSA, while the superficial femoral artery (SFA) was absent, and the popliteal artery (P2 segment) appeared occluded, likely due to acute thrombosis (Figs. 2A and 2B). The distal popliteal artery (P3 segment) was stenosed with atherosclerosis, whereas the PTA demonstrated significant stenosis (Figs. 2A and 2B).
Fig. 2 CT revealed occlusion of the PSA in his left lower extremity. (A) The left PSA originates from the internal iliac artery, passes through the greater sciatic foramen alongside the sciatic nerve, and runs laterally to the insertion of the adductor magnus muscle before continuing as the popliteal artery. The SFA is completely absent. (B) The left PSA was occluded with acute thrombosis in the popliteal artery P2 segment and stenosed with atherosclerosis in the P3 segment. SFA: superficial femoral artery; CT: computed tomography; PSA: persistent sciatic artery
Revascularization was performed under general anesthesia. The left inguinal region was incised to expose the origin of the SFA. A second incision was made in the mid-calf region on the left side, revealing the PTA. We performed an SFA-to-PTA bypass using a single-segment great saphenous vein graft in a non-reversed fashion. After distal anastomosis, complete angiography revealed no stenosis at the proximal or distal anastomotic sites.
The operation time was 255 min, and intraoperative bleeding was 30 mL. No peri-operative events were observed.
Aspirin (100 mg/day) was started a week before the operation, and edoxaban (30 mg/day) was administered postoperatively.
The ABI improved from 0.74 to 0.89 postoperatively, and pain in the left toe was diminished. CT demonstrated a patent SFA-to-PTA bypass (Fig. 3).
Fig. 3 Postoperative CT demonstrated that the SFA to PTA bypass is patent (A, B). SFA: superficial femoral artery; CT: computed tomography; PTA: posterior tibial artery
He was discharged on day 13 postoperative with ambulatory status.
After discharge, the necrosis of the left first, second, and third toes also improved, and no further minor amputations were needed during the follow-up period.
Discussion
The PSA is an exceptionally rare vascular anomaly, occurring in only 0.025%–0.04% of the general population.^1)^ The PSA originates from the internal iliac artery, exits the pelvis through the greater sciatic foramen alongside the sciatic nerve, travels laterally past the insertion of the adductor magnus muscle, and then continues as the popliteal artery. There are 4 types of PSA (Supplementary Table 1).
This case had type 2b, a complete PSA with an incompletely developed femoral artery in which the SFA was absent entirely.^2)^
Thrombotic complications are common in patients with COVID-19 and tend to increase mortality and morbidity.^3–5)^ A study found that the pooled incidence of arterial thrombosis (AT) in critically ill COVID-19 patients admitted to intensive care units was 4.4%. The anatomical distribution of arterial thrombotic events was diverse, occurring in limb arteries (39%), cerebral arteries (24%), great vessels (aorta, common iliac artery, common carotid artery, and brachiocephalic trunk; 19%), coronary arteries (9%), and the superior mesenteric artery (8%). The mortality rate among these patients was approximately 20%.^6)^
The mechanisms of AT in COVID-19 patients remain unclear. Emerging evidence suggests that COVID-19 is associated with endotheliitis, characterized by extensive endothelial cell damage and infiltration by inflammatory cells.^7,8)^ This endothelial damage may result from direct viral infection, facilitated by the overexpression of angiotensin-converting enzyme 2 (ACE2), the receptor through which SARS-CoV-2 gains entry into endothelial cells.
Furthermore, COVID-19 is linked to a hypercoagulable state, characterized by elevated levels of D-dimer, prothrombin, and fibrinogen, along with shortened clot formation time and increased maximum clot firmness. This hyperviscosity is believed to stem from systemic extrapulmonary inflammation and cytokine storms, which activate the coagulation cascade. These factors—endotheliitis, hypercoagulability, and prolonged immobilization in severe COVID-19 patients—provide a plausible explanation for the development of AT.^7,9)^ The present patient was infected with COVID-19, and COVID-19 infection might have contributed to acute thrombosis in his PSA level.
Aneurysmal degeneration is seen in 41%–60% of patients with PSA, and many of these patients present with symptoms due to thrombosis, embolization, or local compression. The patient in the present case did not have an aneurysm of the PSA but developed thrombosis of the left PSA.
To the best of our knowledge, previous reports have not shown that COVID-19 causes acute thrombosis in patients with PSA.
In this patient, the PSA was not aneurysmal, but arterial sclerosis progressed, and the patient was susceptible to external forces owing to its anatomical location, which could have been a possible cause of acute occlusion during COVID-19 infection. In cases of PSA, careful observation is necessary even in the absence of aneurysms, particularly during the COVID-19 infection.
Treatment varies based on the symptoms, type of PSA, and presence or absence of an aneurysm.^2,10,11)^ In a review of 101 cases of popliteal artery aneurysm presenting with acute limb ischemia, Mann et al. noted that 46.1% (n = 47) of the patients underwent open surgical repair, 20.8% (n = 21) were treated with an endovascular approach, another 20.8% (n = 21) received a hybrid treatment, and 10.8% (n = 11) were managed non-surgically due to either mild symptoms or patient refusal of the procedure.^2)^
The report indicated that 84.3% (n = 86) of cases demonstrated good recovery over a mean follow-up period of 21 months, with 3 instances of graft or stent occlusion recorded.^2)^
This case involved type 2b PSA without SFA, and endovascular treatment was anatomically difficult to perform. In addition, the patient had severe toe necrosis; thus, we chose open bypass rather than endovascular treatment because of the increased blood supply.
Conclusion
PSA is an extremely rare vascular phenomenon, and we encountered a patient who presented with acute thrombosis of the non-aneurysmal PSA due to COVID-19. The complicated disease was successfully treated using SFA-to-PTA bypass.
Declarations
Informed consent
Written informed consent was obtained from the patient for the publication of the case details.
Ethics approval
This study was approved by the Ethics Committee of Fukuyama Cardiovascular Hospital (No. 114).
Data availability statement
The data that support the findings of this study are available from the corresponding author, D.F., upon reasonable request.
Acknowledgments
We would like to thank Editage (www.editage.jp) for English language editing.
Disclosure statement
The authors declare no conflicts of interest associated with this manuscript.
Author contributions
Study conception: DF and TK
Data collection: DF
Manuscript preparation: DF
Critical review and revision: all authors
Final approval of the article: all authors
Accountability for all aspects of the work: all authors.
Supplementary Information
Supplementary Table 1. Type of persistent sciatic artery
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meghpara MK, Alaoudi M, Mutyala M. Persistent sciatic artery in a patient with unilateral acute lower extremity ischemia. J Vasc Surg Cases Innov Tech 2020; 7: 89–92.33665539 10.1016/j.jvscit.2020.08.034PMC 7902998 · doi ↗ · pubmed ↗
- 2Mann A, Liu E, Naji F. Persistent sciatic artery aneurysm presenting with acute limb ischemia: case report and review of the literature. Ann Vasc Surg Brief Rep Innov 2022; 2: 100062.
- 3Togni Filho PHA, Leite ALSV, Sampaio MP, et al. Case report: persistent bilateral complete sciatic artery associated with aneurysmal degeneration. J Vasc Bras 2024; 23: e 20230151.39286309 10.1590/1677-5449.202301512 PMC 11404772 · doi ↗ · pubmed ↗
- 4Farkouh ME, Stone GW, Lala A, et al. Anticoagulation in patients with COVID-19: JACC review topic of the week. J Am Coll Cardiol 2022; 79: 917–28.35241226 10.1016/j.jacc.2021.12.023PMC 8884342 · doi ↗ · pubmed ↗
- 5Al-Samkari H, Karp Leaf RS, Dzik WH, et al. COVID-19 and coagulation: bleeding and thrombotic manifestations of SARS-Co V-2 infection. Blood 2020; 136: 489–500.32492712 10.1182/blood.2020006520 PMC 7378457 · doi ↗ · pubmed ↗
- 6Cheruiyot I, Kipkorir V, Ngure B, et al. Arterial thrombosis in coronavirus disease 2019 patients: a rapid systematic review. Ann Vasc Surg 2021; 70: 273–81.32866574 10.1016/j.avsg.2020.08.087PMC 7453204 · doi ↗ · pubmed ↗
- 7Merad M, Martin JC. Pathological inflammation in patients with COVID-19: a key role for monocytes and macrophages. Nat Rev Immunol 2020; 20: 355–62.32376901 10.1038/s 41577-020-0331-4PMC 7201395 · doi ↗ · pubmed ↗
- 8Varga Z, Flammer AJ, Steiger P, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020; 395: 1417–8.32325026 10.1016/S 0140-6736(20)30937-5PMC 7172722 · doi ↗ · pubmed ↗