Seroprevalence of Cytomegalovirus Among Pregnant Women at Kawempe National Referral Hospital, Uganda: A Cross-sectional Study
Richard V Katungye, Moses Musooko, Musa Sekikubo, Tobius Mutabazi, Mary Kyohere, Valerie Tusubira, Juliet Nsimire Sendagala, Joseph Peacock, Kirsty Le Doare, Annettee Nakimuli, Abdelmajid Djennad, Abdelmajid Djennad, Agnes Nyamaizi, Agnes Ssali, Alexander Amone, Amusa Wamawobe

TL;DR
This study found that all pregnant women in Kampala, Uganda, had been exposed to cytomegalovirus (CMV), with recent infections more common among those with lower socioeconomic status.
Contribution
The study provides the first detailed assessment of CMV seroprevalence and risk factors among pregnant women in Kampala, Uganda.
Findings
CMV IgG seroprevalence was 100% among pregnant women in Kampala.
5.8% of women had CMV IgM, indicating recent infection.
Lower socioeconomic status was associated with recent CMV infection.
Abstract
Maternal primary cytomegalovirus (CMV) infection is associated with abortion and congenital anomalies. In Uganda, the burden of maternal CMV infection is not well studied. This study thus assessed the seroprevalence and factors associated with CMV infection among pregnant women at Kawempe National Referral Hospital in Kampala. This work forms a part of the PROGRESS study, an observational cohort study undertaken in Kampala, Uganda, between November 2018 and April 2021. We conducted a cross-sectional study between September 2020 and January 2021 among the 639 pregnant women admitted to the labor ward at a government hospital. Sociodemographic, medical, obstetric, and socioeconomic data were collected. Blood samples from study participants were drawn and analyzed for the presence of CMV immunoglobulin G (IgG) and IgM using enzyme-linked immunosorbent assay–based quantitative assays.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
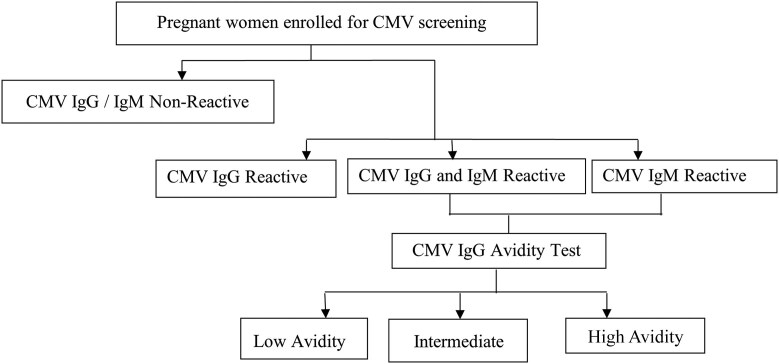 Figure 1
Figure 1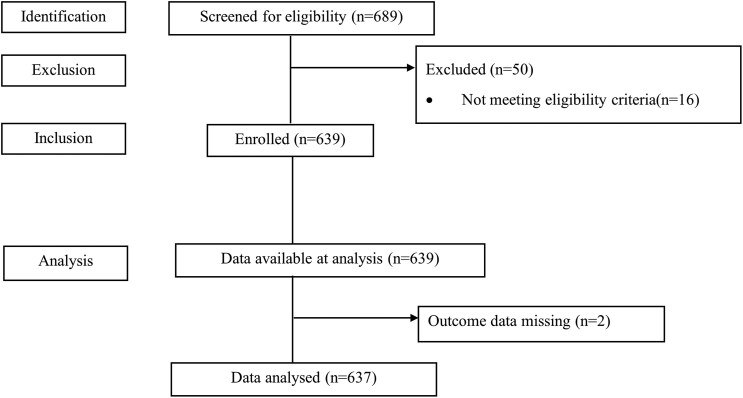 Figure 2
Figure 2| Characteristic | Frequency, No. (%) | Outcome (CMV IgM) | 95% CI | |
|---|---|---|---|---|
| Positive, No. (%) | Negative, No. (%) | |||
| Age | n = 625 | |||
| ≤24 y | 335 (53.6) | 22 (6.6) | 313 (93.4) | 0.43–0.77 |
| 25–34 | 257 (41.1) | 13 (5.1) | 244 (94.9) | 0.19–0.51 |
| ≥35 y | 33 (5.3) | 1 (3.0) | 32 (97.0) | 0.001–0.15 |
| Education level | ||||
| None | 12 (1.9) | 1 (8.3) | 11 (91.7) | 0.001–0.14 |
| Primary | 225 (35.3) | 12 (5.3) | 213 (94.7) | 0.18–0.50 |
| Secondary | 358 (56.2) | 19 (5.3) | 339 (94.7) | 0.34–0.68 |
| Tertiary | 42 (6.6) | 5 (11.9) | 37 (88.1) | 0.05–0.29 |
| Marital status | ||||
| Single | 20 (3.2) | 2 (10.0) | 18 (90.0) | 0.01–0.18 |
| Married | 427 (67.0) | 25 (5.9) | 402 (94.1) | 0.50–0.82 |
| Cohabiting | 190 (29.8) | 10 (5.26) | 180 (94.74) | 0.14–0.44 |
| Wealth | ||||
| Very poor | 389 (61.0) | 21 (5.4) | 368 (94.6) | 0.39–0.73 |
| Poor | 122 (19.2) | 12 (9.8) | 110 (90.2) | 0.18–0.50 |
| Less poor | 126 (19.8) | 4 (3.2) | 122 (96.8) | 0.03–0.25 |
| Body mass index | ||||
| Underweight | 2 (0.3) | 1 (50.0) | 1 (50.0) | 0.001–0.14 |
| Normal | 136 (21.3) | 7 (5.15) | 129 (94.85) | 0.08–0.35 |
| Overweight | 324 (50.9) | 22 (6.8) | 302 (93.2) | 0.42–0.75 |
| Obese | 175 (27.5) | 7 (4.0) | 168 (96.0) | 0.08–0.35 |
| MUAC | ||||
| ≤23 cm (under nutrition status) | 169 (26.5) | 12 (7.1) | 157 (92.9) | 0.18–0.50 |
| >23 cm (normal nutrition status) | 468 (73.47) | 25 (5.3) | 443 (94.7) | 0.50–0.82 |
| Gravidity | ||||
| 1 | 291 | 18 (6.2) | 273 (93.8) | 0.32–0.66 |
| 2–4 | 275 (43.2) | 17 (6.2) | 258 (93.8) | 0.29–0.63 |
| >4 | 71 (11.1) | 2 (2.8) | 69 (97.2) | 0.01–0.18 |
| Parity | ||||
| Low parity (≤4 pregnancies) | 605 (95.0) | 36 (6.0) | 569 (94.0) | 0.89–0.99 |
| High parity (>4 pregnancies) | 32 (5.0) | 1 (3.1) | 31 (96.9) | 0.001–0.14 |
| HIV status | ||||
| Positive | 29 (4.6) | 0 (0.0) | 29 (100.0) | |
| Negative | 608 (95.4) | 37 (6.1) | 571 (93.9) | |
| History of abortion | ||||
| No | 582 (91.4) | 37 (6.4) | 545 (93.6) | |
| Yes | 55 (8.6) | 0 (0.0) | 55 (100.0) | |
| History of diabetes | ||||
| No | 614 (96.4) | 36 (5.9) | 578 (94.1) | 0.89–0.99 |
| Yes | 23 (3.6) | 1 (4.3) | 22 (95.7) | 0.001–0.14 |
| History of hypertension | ||||
| No | 613 (96.2) | 36 (5.9) | 577 (94.1) | 0.89–0.99 |
| Yes | 24 (3.8) | 1 (4.17) | 23 (95.83) | 0.001–0.14 |
| Variable | Frequency | Positive IgM Outcome, n (%) | Negative IgM Outcome, n (%) | Bivariate Analysis, |
| Multivariate Analysis, |
|
|---|---|---|---|---|---|---|---|
| Age | n = 625 | ||||||
| ≤24 y | 335 | 22 (6.6) | 313 (93.4) | Ref | … | Ref | |
| 25–34 y | 257 | 13 (5.1) | 244 (94.9) | 0.76 (0.37–1.54) | .44 | 0.69 (0.33–1.44) | .33 |
| ≥35 y | 33 | 1 (3.0) | 32 (97.0) | 0.44 (0.06–3.42) | .44 | 0.06 (0.07–4.19) | .53 |
| Education level | |||||||
| None | 12 | 1 (8.3) | 11 (91.8) | 0.67 (0.07–6.38) | .70 | 0.73 (0.07–7.31) | .79 |
| Primary | 225 | 12 (5.3) | 213 (94.7) | 0.42 (0.14–1.25) | .119 | 0.42 (0.12–1.21) | .14 |
| Secondary | 358 | 19 (5.3) | 339 (94.7) | 0.42 (0.15–1.18) | .098 | 0.33 (0.11–0.99) | .05 |
| Tertiary | 42 | 5 (11.9) | 37 (88.1) | Ref | - | Ref | |
| Wealth status | |||||||
| Very poor | 389 | 21 (5.4) | 368 (94.6) | 1.74 (0.58–5.17) | .318 | 1.70 (0.54–5.34) | .36 |
| Poor | 122 | 12 (9.8) | 110 (90.2) | 3.33 (1.04–10.62) | .042 | 3.44 (1.05–11.32) |
|
| Less poor | 126 | 4 (3.2) | 122 (96.8) | Ref | Ref | ||
| BMI | |||||||
| Normal | 136 | 7 (5.1) | 129 (94.9) | Ref | Ref | ||
| Underweight | 2 | 1 (50.0) | 1 (50.0) | 18.43 (1.04–326.42) | .05 | 24.50 (1.30–462.28) |
|
| Overweight | 324 | 22 (6.8) | 302 (93.2) | 1.34 (0.56–3.22) | .51 | 1.28 (0.52–3.14) | .59 |
| Obese | 175 | 7 (4.0) | 168 (96.0) | 0.77 (0.26–2.24) | .63 | 0.71 (0.24–2.14) | .55 |
- —Bill and Melinda Gates Foundation10.13039/100000865
- —St George's, University of London10.13039/501100004337
- —SGUL
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Parvovirus B19 Infection Studies · Herpesvirus Infections and Treatments
Cytomegalovirus (CMV) is the leading cause of congenital infection worldwide [1]. Transplacental spread can occur at any gestational age and presents with a variety of abnormal pregnancy and birth outcomes, occurring in up to 30% of primary and 2% of recurrent CMV infections in pregnancy [2]. Congenital CMV (cCMV) can cause permanent sequelae in about 15% to 18% of births including neurocognitive sequelae, hearing loss, and infant mortality [3, 4].
CMV is ubiquitous in African countries, with seroprevalence in pregnancy ranging from 88% to 100% [5, 6] and a cCMV rate of ∼3% despite preexisting maternal immunity. It is strongly associated with maternal HIV infection [7]. The consequences for infants with cCMV have not been widely studied in Africa, but there is emerging consensus that cCMV may be a cause of significant morbidity and mortality.
Low socioeconomic status, poor sanitation, and poor housing conditions are among the factors associated with CMV infection [8, 9]. Uganda has a rapid annual population growth rate of about 3.3%, and the majority of people in urban centers are of low socioeconomic status, living in communities with poor housing and sanitation [10]. In these settings, the sero-prevalence of CMV among children aged <1 year is 83% [11], which contrasts with the rate observed in European countries, where CMV exposure occurs among older children.
Data on the magnitude of CMV among pregnant women in Uganda are limited despite the potentially significant cCMV burden among infants. Consequently, CMV screening services in antenatal care programs to detect mothers at high risk of congenital transmission have not been embraced. This study therefore determined the seroprevalence of CMV and associated factors among pregnant women and their infants at Kawempe National Referral Hospital.
This paper forms part of a supplement based on the PROGRESS study. The seroepidemiology of maternally derived antibodies against group B Streptococcus in Mulago/Kawempe Hospitals Uganda (PROGRESS) study aimed to describe the causes of infectious mortality and morbidity as well as the seroepidemiology of group B streptococcal infection—the major cause of neonatal sepsis worldwide—in Kampala, Uganda [12].
METHODS
Study Design
This was a cross-sectional study conducted between September 2020 and January 2021 among 637 pregnant women admitted to the labor ward at Kawempe National Referral Hospital. Participant recruitment sites for the studies that form part of this supplement are detailed in a flowchart available in the supplementary material of another paper published in this issue [13].
Study Setting
Kawempe National Referral Hospital (KNRH) is a tertiary referral hospital in Kampala, located in central Uganda. Kampala city has a population of about 1 610 500; 827 797 are women [14]. KNRH offers free health care services and specializes in obstetrics, gynecology, pediatrics, and neonatal care services. On average, the facility conducts 70 labor ward admissions daily and 23 434 deliveries annually [15]. The highest percentage of patients admitted at the facility are low–socioeconomic status members of the community who reside in the city slums, which are characterized by poor sanitation and hygiene conditions. The labor ward is a very busy site that is run by a skilled team of health workers led by a specialist, with 3–5 residents, 1 medical officer, 2–3 intern doctors, and several cadres of midwives operating in shifts; it runs on a 24-hour basis.
Study Population and Procedures
Pregnant women who were admitted to the labor ward at Kawempe National Referral Hospital between September 21, 2020, and January 15, 2021, and met the study eligibility criteria were systematically enrolled into the study. In order to randomly select participants, research assistants screened every 10th pregnant woman attending care for enrollment into the study. A participant was enrolled if she was aged 15–49 years, was pregnant and admitted to the labor ward, and gave full written informed consent to participate in the study. Research assistants collected data on sociodemographic characteristics (age, marital status, highest level of education, and wealth [determined by income and possession of household items]), medical characteristics (weight, height, gravidity, parity, mid-upper arm circumference [MUAC], body mass index [BMI; determined as a woman's weight in kilograms divided by the square of height in meters], history of hypertension, diabetes, tuberculosis, and HIV status), and behavioral characteristics (alcohol consumption and smoking status), which were recorded using Research Electronic Data Capture (REDCap) tools [16]. Venous blood samples from each participant were collected into Serum Separator Tube (SST) vacutainers. The sample was centrifuged on site and sent to the Medical Research Council–Uganda Virus Research Institute (MRC-UVRI) laboratory for CMV serology analysis. All infants had a nasal swab taken by a trained health care worker before discharge. Swabs were also sent to MRC-UVRI for real-time polymerase chain reaction (PCR).
Laboratory Analysis
Laboratory analyses were conducted at MRC-UVRI laboratory, which is accredited by the International Standards Organization (#ISO-15189-2012) and Good Clinical Laboratory Practices (GCLP) Accreditation Scheme-UK (#01908). CMV IgG and IgM were detected using the quantitative Elecsys CMV Immunoglobulin Assay. The assay detection range for IgG and IgM was 0.25–500 µ/mL, where the threshold for reactive titer was >1 µ/mL (specificity 96.6% and sensitivity 100% vs specificity 92.3% and sensitivity 93.9%, respectively). The CMV IgG low avidity index test was conducted on all IgM-positive samples using the Elecsys CMV IgG Avidity Assay. Low avidity was defined at <45%, indicating the highest risk of vertical transmission. Intermediate avidity ranged from 45% to 54.9%, and high avidity was defined at ≥55%, indicating the lowest risk of vertical transmission (assay sensitivity 94.8%, specificity 95.8%). All assays were run on a COBAS-601 analyzer, where daily quality control and calibration were performed. Infants born to women with a positive IgM were subjected to a CMV PCR test. The algorithm for evaluation of cytomegalovirus infection is presented in Figure 1.
Algorithm for evaluation of cytomegalovirus infection in pregnancy. Abbreviations: CMV, cytomegalovirus; Ig, immunoglobulin.
Data Management and Analysis
Univariate analyses were conducted to describe the sociodemographic and medical characteristics of the study population. Results were categorized as CMV negative or CMV positive. First, to determine the seroprevalence of CMV, which was defined as past exposure to CMV and indicated by the presence of CMV IgG antibodies in serum using a quantitative enzyme-linked immunosorbent assay (ELISA), we divided the number of pregnant women who tested CMV (IgG) positive by the total number of study participants. CMV IgG positive was defined as having CMV serum titer values ≥1.0 units/mL. Logistic regression analyses were conducted to determine factors associated with CMV among pregnant women. The primary outcome was a woman testing CMV IgM positive, defined as having a CMV serum titer cutoff index ≥1.0. All statistical tests were 2-sided with adjusted odds ratios that were presented with their 95% CIs and P values. At the multivariate level, statistical significance was considered for the factors whose P values were <.05. Analysis was undertaken using STATA, version 15 (Stata Corp LP, College Station, TX, USA).
RESULTS
Study Population
The study enrolled 639 pregnant participants, from whom 637 samples were analyzed. Two of the 639 samples were not included in the final analysis for having faint labels that could not be read. Details are illustrated in Figure 2. The median age (interquartile range) of the study participants was 24 (21–29) years, and 26.5% (169/637) of women had an MUAC <23 cm. The majority of participants (56.2%, n = 358) reported some secondary education. About 9% (55/637) of the study participants had a history of previous abortion. HIV prevalence among the study population was 4.6%. There was no congenital abnormality recorded. Details of the sociodemographic and medical characteristics of the study population are presented in Table 1.
Study flowchart.
Seroprevalence of CMV Infection and Associated Factors
The seroprevalence of CMV IgG was 100% (637/637), and the seroprevalence of CMV IgM was 5.8% (37/637). The IgG avidity index for all CMV IgM–positive samples was >45% (low risk of vertical transmission), and all infants born to women with positive IgM had a negative CMV PCR.
Pregnant women who were poor as compared with the less poor ones were about 3 times more likely to have CMV infection (adjusted odds ratio, 3.44; 95% CI, 1.05–11.32; P = .04). Details are summarized in Table 2.
DISCUSSION
The results from this study indicate universal CMV exposure in this population and low transmission risk. Several studies conducted among pregnant women in Africa have reported equally high levels of CMV exposure; 88.4% among pregnant women in Kenya [5], 96% among Egyptian women [6], 88.6% in Ethiopia [17], 99.6% in Zimbabwe [18], 100% in Namibia [19], and 73.9% among pregnant women attending antenatal clinics in Tanzania [20]. This low risk of vertical transmission was supported by the negative PCR results in infants, indicating that cCMV may not be vertically acquired in our population and early postnatal transmission may account for the high seropositivity rate by the age of 1 year in Uganda [11].
In this study, pregnant women in the lower wealth percentile were 3 times more likely to have recent CMV infection compared with the highest percentile. These findings are consistent with previous studies conducted in the United States and Canada that found a higher burden of CMV among people of low socioeconomic status compared with those with a higher status [9, 21–23]. The probable reason for the higher prevalence of CMV infection among the poor could be due to poor hygiene standards among the urban poor population. Increased risk of CMV exposure has previously been associated with poor standards of living [24, 25]. It is notable that part of the catchment area of our study has densely populated slums characterized by poor housing and sanitation facilities, which could explain the extremely high risk of CMV exposure among the study population.
Limitations
This study acknowledges several limitations. A single CMV ELISA titer may not offer a sufficiently conclusive result; hence serial titers may be required for confirmation, although the study was not designed to follow women longitudinally. No formal neurodevelopmental assessment of infants occurred, so we cannot completely rule out neurodevelopmental sequelae.
CONCLUSIONS
Despite universal CMV IgG seroprevalence, a moderate proportion of 5.8% had CMV infection in pregnancy, and this was common among the poor population of women. Our findings demonstrate a need for better screening policies for women and children to investigate the true burden of cCMV in Uganda.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Manicklal S, Emery VC, Lazzarotto T, Boppana SB, Gupta RK. The “silent” global burden of congenital cytomegalovirus. Clin Microbiol Rev 2013; 26:86–102.23297260 10.1128/CMR.00062-12PMC 3553672 · doi ↗ · pubmed ↗
- 2Boppana SB, Rivera LB, Fowler KB, Mach M, Britt WJ. Intrauterine transmission of cytomegalovirus to infants of women with preconceptional immunity. N Engl J Med 2001; 344:1366–71.11333993 10.1056/NEJM 200105033441804 · doi ↗ · pubmed ↗
- 3Korndewal MJ, Oudesluys-Murphy AM, Kroes ACM, van der Sande MAB, de Melker HE, Vossen ACTM. Long-term impairment attributable to congenital cytomegalovirus infection: a retrospective cohort study. Dev Med Child Neurol 2017; 59:1261–8.28990181 10.1111/dmcn.13556 · doi ↗ · pubmed ↗
- 4Buca D, Di Mascio D, Rizzo G, et al Outcome of fetuses with congenital cytomegalovirus infection and normal ultrasound at diagnosis: systematic review and meta-analysis. Ultrasound Obstet Gynecol 2021; 57:551–9.33030767 10.1002/uog.23143 · doi ↗ · pubmed ↗
- 5Maingi Z, Nyamache AK. Seroprevalence of cytomegalo virus (CMV) among pregnant women in Thika, Kenya. BMC Res Notes 2014; 7:794.25392013 10.1186/1756-0500-7-794PMC 4247150 · doi ↗ · pubmed ↗
- 6Kamel N, Metwally L, Gomaa N, Sayed Ahmed WA, Lotfi M, Younis S. Primary cytomegalovirus infection in pregnant Egyptian women confirmed by cytomegalovirus Ig G avidity testing. Med Princ Pract 2014; 23:29–33.24052007 10.1159/000354758 PMC 5586833 · doi ↗ · pubmed ↗
- 7Bates M, Brantsaeter AB. Human cytomegalovirus (CMV) in Africa: a neglected but important pathogen. J Virus Erad 2016; 2:136–42.27482452 10.1016/S 2055-6640(20)30456-8PMC 4967964 · doi ↗ · pubmed ↗
- 8Enders G, Bäder U, Bartelt U, Daiminger A. Zytomegalievirus-(CMV-) durchseuchung und häufigkeit von CMV-primärinfektionen bei schwangeren frauen in Deutschland. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2003; 46:426–32.