Medication Error Management in Private Hospitals in Costa Rica: A Mixed-Methods Evaluation of Practices and Improvement Strategies
Jorge Arturo Villalobos-Madriz, Esteban Zavaleta-Monestel, Ernesto Martínez-Vargas, Abigail Fallas-Mora, Melissa Prado-Rivero, Natalia Bastos-Soto, Gary Cochran

TL;DR
This study evaluates medication error practices in Costa Rican private hospitals and suggests strategies to improve patient safety.
Contribution
The study introduces a mixed-methods approach to assess and improve medication error management in a specific regional healthcare context.
Findings
Hospitals implemented 74% of evaluated medication management practices.
Prescription and transcription stages were most prone to errors.
Most errors were detected before reaching patients, involving general and high-risk drugs.
Abstract
Introduction: Medication errors pose significant risks to patient safety and healthcare quality. This study analyzes the practices of identification and management of these errors in private hospitals in Costa Rica from January 2020 to January 2024. Methodology: A cross-sectional survey was conducted in four private hospitals, evaluating 167 items related to 11 key drug management processes. In addition, a detailed analysis of retrospective data was carried out at one of the participating hospitals to delve deeper into the nature of the errors. Results: The hospitals presented an overall level of implementation of 74% in the practices evaluated. The prescription and transcription stages were the most vulnerable, while most errors were detected before affecting patients. The drugs involved were mainly of general use and high risk. Conclusion: The results highlight the importance of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
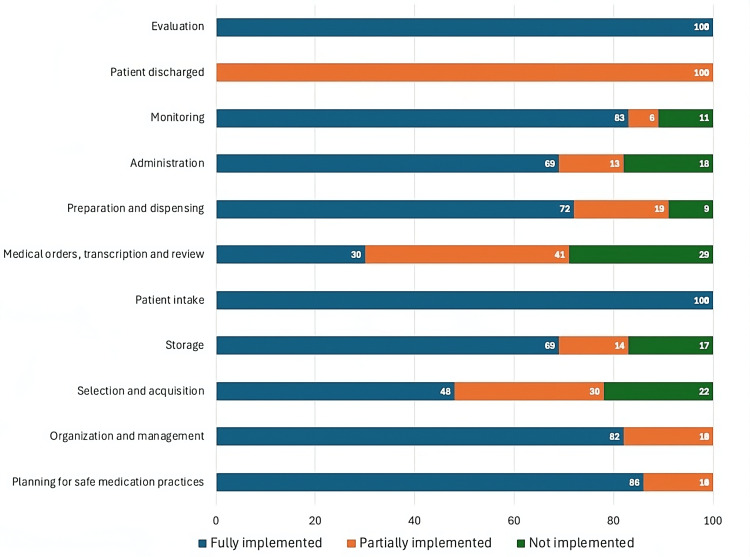 Figure 1
Figure 1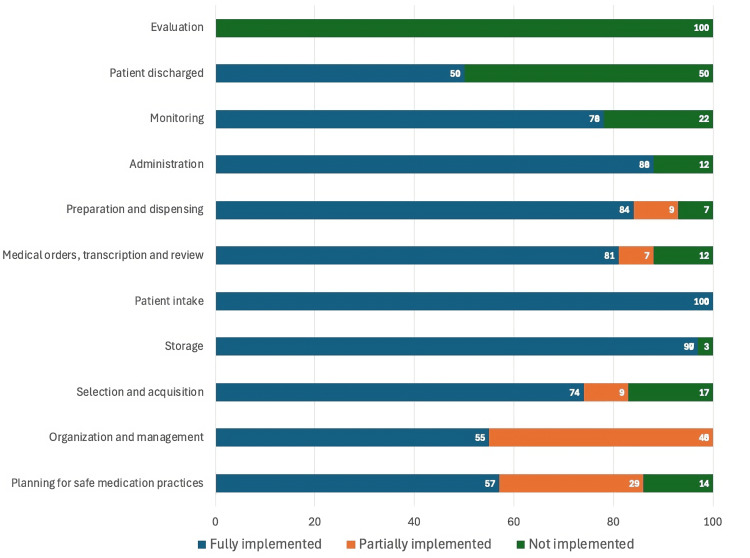 Figure 2
Figure 2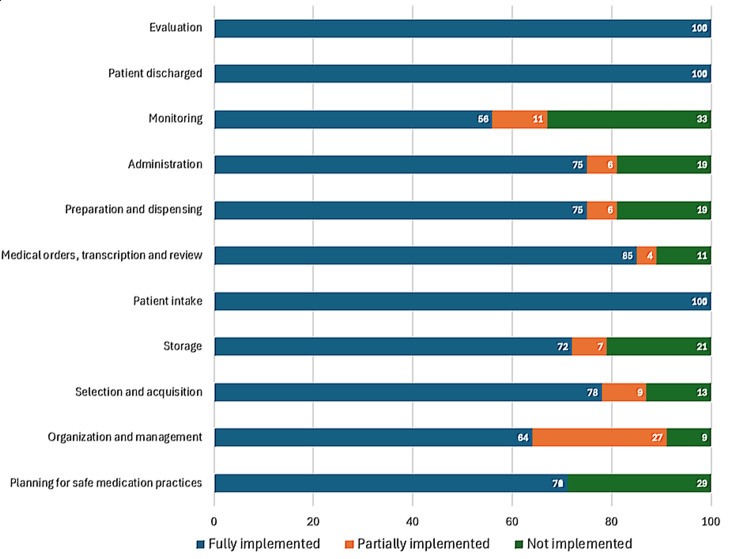 Figure 3
Figure 3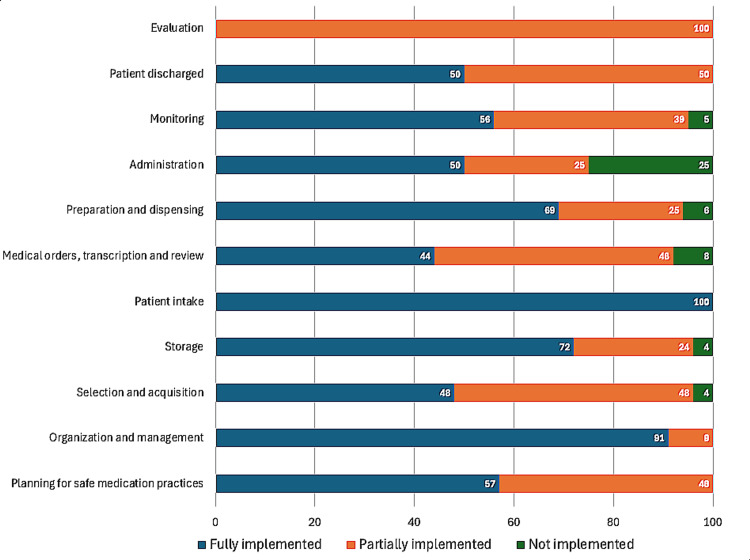 Figure 4
Figure 4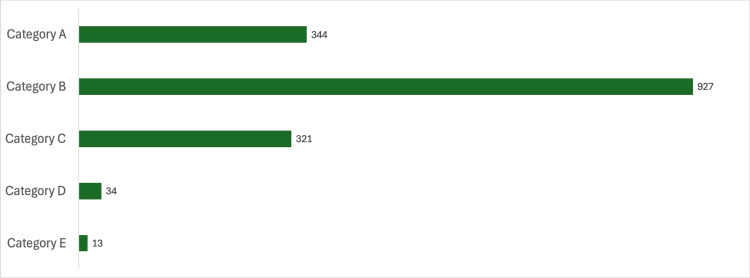 Figure 5
Figure 5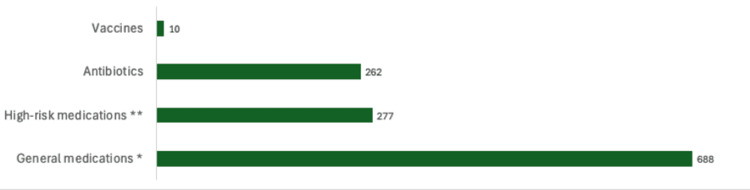 Figure 6
Figure 6| Implemented (%) | Partially implemented (%) | Not implemented (%) | |
| Hospital A | 80 | 15 | 5 |
| Hospital B | 60 | 30 | 10 |
| Hospital C | 74 | 20 | 6 |
| Hospital D | 63 | 27 | 10 |
| Stage of the process at which the error was made | Number of errors made, n(%) |
| Prescription | 706 (43.07) |
| Transcription | 494 (30.14) |
| Dispensation | 132 (8.05) |
| Labeling | 125 (7.63) |
| Administration | 111 (6.77) |
| Storage | 41 (2.50) |
| Conciliation | 29 (1.77) |
| Monitoring | 1 (0.07) |
| Total | 1639 (100) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPatient Safety and Medication Errors · Pharmaceutical Practices and Patient Outcomes · Medical Malpractice and Liability Issues
Introduction
Medications are the most widely used medical intervention worldwide. However, the increase in medication use goes hand in hand with an increased occurrence of medication errors [1]. These represent one of the leading causes of preventable injuries within healthcare systems around the world [2].
A medication error refers to any preventable incident caused by the improper use of medications, which can lead to harm to the patient [1]. They can occur at any stage of the medication process, including manufacturing, packaging, storage, and distribution, all the way to prescribing, transcription, review, preparation, labeling, dispensing, administration, and follow-up [1, 3]. These errors are related to professional practice, products, procedures, and healthcare systems [1].
It is estimated that one in 10 patients suffers some harm in a healthcare setting, and one in 20 can be attributed to a medication error, of which half are preventable [4]. In the United States, it represents the sixth most common cause of death, accounting for injuries to approximately 1.3 million people in a one-year period [5,6]. According to data from the World Health Organization, it is estimated that annually, medication errors represent an expense of 42 billion dollars per year for the health sector [4].
The private healthcare system in Costa Rica complements the robust public healthcare system, offering high-quality services with a focus on advanced technology, personalized care, and shorter wait times. Internationally, it stands out for its growing adoption of global standards of quality and safety in care, including the management of medication errors. However, compared to systems in developed countries, challenges remain related to the homogeneous implementation of safe practices and equitable access to technological and training resources. These factors reflect a developing context, where the integration of assessment tools and preventive strategies, adapted to local needs, is key to closing gaps in patient safety [7-10].
Given this, the objective of this work is to analyze the processes of identification and management of medication errors in private hospitals in Costa Rica during the period of January 2020 to January 2024 through the application of a survey to these hospitals. Through this analysis, we seek to describe the nature and frequency of medication errors that occur in these settings, develop an evaluation tool based on international guidelines to measure the effectiveness of medication error management systems, and evaluate the level of implementation of preventive and corrective strategies in the selected hospitals.
The study also aims to identify critical areas for improvement in drug management and provide specific recommendations that allow hospital institutions to optimize the safety of their pharmacotherapeutic processes, with the aim of protecting patients' health and reducing the incidence of adverse drug-related events.
Materials and methods
This study employed a mixed-methods design, integrating a cross-sectional survey with a retrospective analysis of medication error data. This approach was selected to provide a comprehensive understanding of medication error identification and management systems in private hospitals in Costa Rica from January 2020 to January 2024. This study was conducted at Hospital Clinica Biblica, San José, Costa Rica.
The mixed-methods design leveraged the survey to evaluate the implementation of safety practices, identifying strengths and areas for improvement across multiple key processes. The retrospective analysis, in turn, provided detailed insights into the most vulnerable stages, types of errors, and medications involved in a specific hospital. This combination of quantitative and qualitative data ensured a holistic perspective, enhancing the findings' validity and practical applicability.
Sampling method
The study employed purposive sampling to select hospitals and participants, aiming to capture data from a diverse range of healthcare settings. Four Costa Rican private hospitals with varying levels of complexity were included: Hospital A, Hospital B, Hospital C, and Hospital D. Inclusion criteria required hospitals to have established medication management processes and available data on medication errors during the study period. Hospitals were excluded from the study if they lacked complete or consistent records on medication errors during the analysis period, did not have formal protocols for medication management, did not grant authorization to participate, or were not operational throughout the entire study period.
Hospital A has 75 beds, five specialized services, 20 operating rooms, 18 specialties, and three accreditations. Hospital B, with 10 beds, offers three specialized services, two operating rooms, and 28 specialties and has no accreditations. Hospital C features 11 beds, five specialized services, five operating rooms, and 36 specialties and also lacks accreditations. Finally, Hospital D, the largest among the group, has 234 beds, five specialized services, eight operating rooms, 25 specialties, and seven accreditations.
Although an evaluation instrument was applied to four private hospitals in Costa Rica, the specific information related to medication errors and their classification was obtained exclusively from Hospital A. This is because this hospital was the only one with complete data on the occurrence of errors across the various stages of the medication process during the study period. Therefore, the detailed analysis of medication errors is limited solely to this institution.
Evaluation tool development and validation
The evaluation tool was developed based on international standards, incorporating guidelines from the American Society of Health-System Pharmacists (ASHP), Joint Commission International (JCI), and the European Medicines Agency (EMA). Designed to comprehensively assess medication management practices, the tool included 167 items organized into 11 key processes. These processes were: planning of safe medication practices, with seven items; organization and management, with 11 items; selection and acquisition of medicines, comprising 23 items; storage, with 29 items; patient admission, covered by one item; medical orders, transcription, and review, with 27 items; preparation and dispensing, including 12 items; administration, with 16 items; follow-up, covered by 18 items; patient discharge, with two items; and evaluation, addressed by one item.
The tool was reviewed and validated by an interdisciplinary committee comprising hospital pharmacists, patient safety specialists, and physicians. The committee ensured that the items comprehensively addressed vulnerabilities at each critical stage of the medication management process.
Data collection
The survey was conducted in January 2024 and was administered in Spanish to professionals responsible for medication error data in each hospital. For publication purposes, the responses were translated into English. Participants evaluated the level of implementation for each item using a three-tiered scale: fully implemented, indicating total compliance; partially implemented, reflecting limited or deficient compliance; and not implemented, signifying no evidence of compliance.
Data analysis
Quantitative data from the survey were analyzed using descriptive statistics to identify patterns, strengths, and areas for improvement. The retrospective analysis of medication error data involved categorizing errors by stage, type, and medication involved. Results from both components were integrated to identify common vulnerabilities and inform tailored strategies for risk mitigation.
Results
Medication error management process assessment tool
A total of 167 items were evaluated and distributed across 11 key processes related to medication error management. The details of these processes and their corresponding evaluations can be found in Appendix A. Table 1 summarizes the individual performance of each hospital as evaluated by the tool.
Figures 1-4 represent the performance of each of the four hospitals in each of the 11 key processes assessed by the Medication Error Management Process Assessment Tool. Of these, it is Hospital A had the highest percentage of processes fully implemented, and Hospitals B and D had the highest percentage of processes classified as "not implemented".
Level of implementation of the processes evaluated by the Medication Error Management Process Assessment Tool in Hospital A
Level of implementation of the processes evaluated by the Medication Error Management Process Evaluation Tool in Hospital B
Level of implementation of the processes evaluated by the Medication Error Management Process Evaluation Tool in Hospital C
Level of implementation of the processes evaluated by the Medication Error Management Process Evaluation Tool in Hospital D
Medication errors
The specific data on medication errors analyzed in this study come only from Hospital A. Although the assessment instrument was applied in four hospitals, Hospital A was the only one that provided complete information on the occurrence of errors in the different stages of the medication process. For this reason, the results classified in terms of stages of the process, severity categories (The National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP)), and types of drugs involved are limited to this institution, allowing for an in-depth analysis of their situation.
During the period between January 2020 and January 2024, a total of 1,605 medication errors were committed in Hospital A, which were classified according to the stage of the medication process where the error was made (Table 2), according to severity (Figure 5), and according to the type of medication (Figure 6).
Classification of medication errors according to their severity as per the NCC MERP classificationNCC MERP: The National Coordinating Council for Medication Error Reporting and Prevention
Classification of medication errors according to medication categories Drugs of wide applicability used in clinical practice for the management of common or less critical diseases; *Medications that carry an increased risk of causing significant harm to the patient when used incorrectly (e.g., blood thinners, anti-cancer agents, concentrated electrolytes).
Figure 5 shows the classification of errors according to their severity according to the classification of the NCC MERP. It is important to note that most of the errors occurred in Category B and that no errors were reported in Categories F, G, H, or I.
Discussion
Medication errors pose a serious threat to patient safety. The main objective of drug therapy is to improve the health and quality of life of those who use it. However, in any healthcare system, errors can occur at various stages of the process, from the storage of medications to their prescription, dispensing, administration, and use by the patient [2,11,12]. These errors have the potential to compromise both the effectiveness of the treatment and the health of the patient, and many of them are perfectly avoidable [11,13].
Improper use of medications can cause harm to the patient when a safe and rational medication use program is not used. Given this, it is of utmost importance that medical staff work together with pharmacists and nurses to provide timely follow-up of pharmacotherapy, especially when reports show that pharmaceutical clinical involvement helps reduce the rate of preventable adverse effects by medications by 78% [14,15].
The evaluation tool developed in this study identified strengths and critical areas for improvement in medication error management systems in Costa Rican private hospitals. Being based on international standards such as those of the ASHP, JCI, and EMA and validated by interdisciplinary professionals in hospital pharmacy, it allows not only a comprehensive analysis of key processes in medication management but also an objective comparison with globally accepted practices, playing a fundamental role in promoting greater standardization in medication-related processes. This tool facilitates the implementation of effective preventive and corrective strategies, promoting a culture of patient safety and improving the quality of pharmacotherapeutic services in the hospital environments evaluated.
The consolidated results obtained through the application of the evaluation tool in the four Costa Rican hospitals reflect a high level of implementation of safe medication practices, while non-implemented processes represent only a minimal proportion. This level of implementation is comparable to the findings reported in Spain, where a multicenter study conducted in intensive care medicine services identified a notable level of compliance with these practices, with no relevant differences based on hospital size or type of service provided [16].
Similarly, in this study, notable differences were observed between the hospitals evaluated in Costa Rica, both in the overall percentage of implementation (sum of the results of each of the processes evaluated) (Table 1) and in the results of the implementation of specific processes (Figures 1-4). For example, while some hospitals achieved complete implementation in certain key processes, others demonstrated notably lower levels of implementation, or even none at all in some critical areas, as illustrated in the graphs in Figures 1-4.
Variability in implementation levels between hospitals is a common phenomenon, influenced by factors such as organizational culture, national and international standards applied, and the availability of specific resources in each institution [17].
These differences highlight the need to design specific strategies for each hospital, focusing on areas that require priority improvements. The application of tools such as the one used in this study facilitates not only the identification of these critical areas but also the standardization of safe practices in medication management. This homogenization is key to guaranteeing patient safety and raising the quality of the health system [18,19]. Likewise, the findings underscore the importance of aligning practices with international standards and strengthening institutional resources, essential elements to optimize safety in pharmacotherapeutic processes.
The analysis of medication errors reported between January 2020 and January 2024 by Hospital A, the study center, and the only one that provides these data, identified a total of 1,639 errors during this four-year period. These errors were distributed throughout the different stages of the medication process, with the prescription and transcription phases standing out as the most vulnerable, with 43.07% (n=706) and 30.14% (n=494) of errors, respectively.
The combination of data from the cross-sectional survey and retrospective analysis provided a comprehensive understanding of medication error management in private hospitals. While the survey offered a broad perspective on the implementation of good practices in four institutions, the retrospective analysis of Hospital A allowed for a detailed exploration of specific errors, their stages, severity, and types of drugs involved.
It is estimated that during the pandemic period, between 50% and 60% of medication errors occurred during the prescription stage [20,21]. Similarly, a study carried out in 2021 in a hospital in Indonesia allows these findings to be compared with international data, revealing that prescription errors were also the most frequent type of medication error, accounting for 54.40% of the total errors recorded [22]. Although the period of analysis of both studies does not coincide, these data provide a relevant perspective on the behavior of this type of error in different contexts, highlighting the importance of implementing global strategies to prevent them and improve patient safety.
These results reflect the high susceptibility of these stages due to the inherent complexity of the processes, the reliance on accuracy in communication, and potential limitations in support systems [23].
It is especially important to point out what a prescription error consists of since this stage is the starting point of pharmacological treatment and has a cascading effect on the rest of the process [24]. Prescription errors encompass critical activities such as labeling, packaging, dispensing, patient education, and monitoring during medication use. Identifying and addressing these issues is critical to ensuring patient safety, as any failure in this phase can lead to serious adverse consequences that affect the efficacy of treatment and put the patient's life at risk [25,26].
The analysis of medication errors occurring during the study period, classified according to their severity, showed that, as can be seen in Figure 5, most of the errors reported corresponded to Category B according to the NCC MERP classification. This implies that most errors were identified before reaching the patient, which reflects the effectiveness of the prevention and early detection systems implemented in the institution.
A notable agreement is observed with the results obtained in other studies reported in the literature. For example, in a study conducted in Mexico between June 2020 and September 2022, 37% of medication errors reported during that period were also classified as Category B, corresponding to the category with the most error reports [27]. This suggests that, regardless of the geographical context, health systems that implement effective monitoring strategies are able to detect a noteworthy proportion of errors in the early stages, thus avoiding negative consequences for patients [28]. These results reinforce the importance of strengthening prevention and screening mechanisms at all levels of the medication process as a key strategy to improve patient safety [29,30].
Likewise, the results show that the medication errors during the study period were predominantly associated with widely prescribed drugs, followed by high-risk drugs, including anticoagulants, opioids, antineoplastic agents, or concentrated electrolytes, and, to a lesser extent, vaccines. This behavior coincides with what has been observed in the results of other studies where the most common errors tend to involve drugs widely used in clinical practice, such as analgesics, anti-inflammatories, and laxatives, mainly due to their high frequency of prescription and administration [2,31].
It is estimated that widely prescribed drugs account for more than 50% of errors reported in medium- and high-complexity hospitals and approximately 38% in high-risk drugs [31].
In general, widely prescribed drugs tend to be more involved in prescription and transcription errors, while high-risk drugs excel in errors during administration, due to the requirement for greater precision in their handling [31-33].
While it is true that widely prescribed drugs have a lower potential for harm than high-risk drugs or vaccines, their high turnover in pharmacies increases the impact on patient safety. This underscores the need to implement prevention strategies targeting not only high-risk drugs but also those in widespread use, improving prescribing, reviewing, and administration processes. Communication strategies are of paramount importance in reducing errors, along with a multi-center approach that includes technology, pharmacist involvement, standardized processes, and strong safety culture that are essential for the mitigation of medication errors [34-35].
Limitations of the study
This study has several limitations that should be considered when interpreting its results. First, the retrospective analysis was based exclusively on Hospital A data, which restricts the generalization of the findings to other private hospitals in Costa Rica, especially those with limited resources or less developed practices in medication error management. In addition, the cross-sectional survey, although robust in its design, depended on the self-reporting of the participating hospitals, which may introduce biases related to the accuracy or completeness of the responses. Despite these limitations, the study provides a solid basis for future research and strategies to improve patient safety in the private hospital context.
Likewise, no direct comparison between the participating hospitals was conducted. This decision was made due to the inherent differences in hospital levels and certifications. These factors influence the implementation of medication error management practices, making direct comparisons between institutions with varying complexities and accreditations methodologically inappropriate.
Conclusions
This study provides critical findings on the management of medication errors in private hospitals in Costa Rica, emphasizing the prescription and transcription stages as the most vulnerable and highest-priority areas for intervention. The effectiveness of existing error detection systems was also demonstrated, particularly in Hospital A, where a notable proportion of errors were intercepted before reaching patients. To address these issues, targeted training programs should focus on mitigating vulnerabilities in these critical stages, while advanced technologies like electronic prescribing and automated dispensing systems can further enhance safety. Standardized protocols must be reinforced to ensure consistency, and foster a culture of open, non-punitive error reporting is essential for continuous improvement. Expanding the use of the evaluation tools to public hospitals and other institutions in the region could help identify specific challenges and promote standardized practices. Aligning local procedures with international standards would strengthen healthcare systems, enhance patient safety, and improve treatment outcomes, offering a comprehensive approach to advancing medication error management and healthcare quality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The effective strategies to avoid medication errors and improving reporting systems Medicines (Basel) Mutair AA Alhumaid S Shamsan A 46820213456408810.3390/medicines 8090046 PMC 8468915 · doi ↗ · pubmed ↗
- 2Risk factors associated with medication administration errors in children: a prospective direct observational study of paediatric inpatients Drug Saf Westbrook JI Li L Woods A 5455564720243844362510.1007/s 40264-024-01408-6PMC 11116173 · doi ↗ · pubmed ↗
- 3Prevalence, contributing factors, and interventions to reduce medication errors in outpatient and ambulatory settings: a systematic review Int J Clin Pharm Naseralallah L Stewart D Price M Paudyal V 135913774520233768240010.1007/s 11096-023-01626-5PMC 10682158 · doi ↗ · pubmed ↗
- 4Medication without harm 12 2024 32024 https://www.who.int/initiatives/medication-without-harm
- 5Preventing the medication errors in hospitals: a qualitative study Int J Afr Nurs Sci Salar A Kiani F Rezaee N 100235132020
- 6Preventable medication harm across health care settings: a systematic review and meta-analysis BMC Med Hodkinson A Tyler N Ashcroft DM 3131820203315345110.1186/s 12916-020-01774-9PMC 7646069 · doi ↗ · pubmed ↗
- 7Health system in Costa Rica (Article in Spanish)Public Health Mex Sáenz M del R Acosta M Muiser J Bermúdez JL 156167532011 http://www.scielo.org.mx/scielo.php?script=sci_abstract&pid=S 0036-36342011000800011&lng=es&nrm=iso&tlng=es 21877081 · pubmed ↗
- 8Primary Health Care as a strategy for the work of health professionals in Costa Rica (Article in Spanish)Rev Hisp Cienc Salud Canales-Mejicano JC 145146302019 https://uhsalud.com/index.php/revhispano/article/view/411