Do patients with ischaemic cardiomyopathy benefit from off-pump coronary bypass surgery? (From the KROK registry)
Kinga Kosiorowska, Marek Jasiński, Roman Przybylski, Marek Deja, Jan Rogowski, Witold Gerber, Jerzy Pacholewicz, Romuald Cichoń, Marek Cisowski, Wojciech Pawliszak, Paweł Bugajski, Michał Krejca, Tomasz Hirnle, Bartłomiej Perek, Zdzisław Tobota, Bohdan Maruszewski

TL;DR
This study compares off-pump and on-pump heart bypass surgery in patients with ischaemic cardiomyopathy, finding short-term benefits for off-pump but better long-term survival with on-pump.
Contribution
The study provides new evidence on the comparative effectiveness of off-pump versus on-pump surgery in ischaemic cardiomyopathy patients using a large national registry.
Findings
Off-pump surgery was linked to lower 30-day mortality and fewer complications.
On-pump surgery showed a modest but significant long-term survival advantage at 10 years.
Short-term benefits of off-pump do not translate to improved long-term survival.
Abstract
This study aimed to compare perioperative outcomes and long-term mortality between off-pump coronary artery bypass grafting and on-pump coronary artery bypass grafting in patients with ischaemic cardiomyopathy who had a left ventricle ejection fraction of ≤35%. A retrospective cohort analysis was conducted using data from the Polish National Registry of Cardiac Surgery Procedures database, encompassing patients who underwent isolated coronary artery bypass grafting in Poland between 2012 and 2022. Patients were divided into two groups: on-pump and off-pump. Propensity score matching was used to balance the groups. The primary outcome was long-term all-cause mortality following surgical revascularization. A total of 9920 patients were included, with 3116 patients in each group after propensity score matching. The median follow-up period was 4 years. The off-pump group was associated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
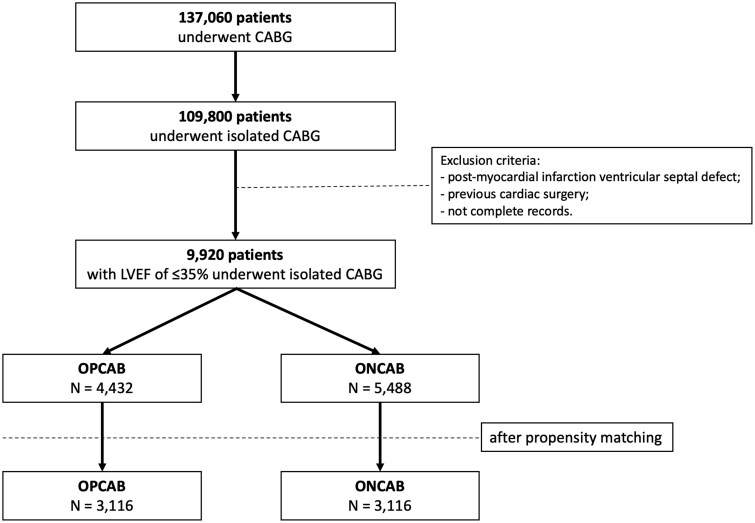 Figure 1
Figure 1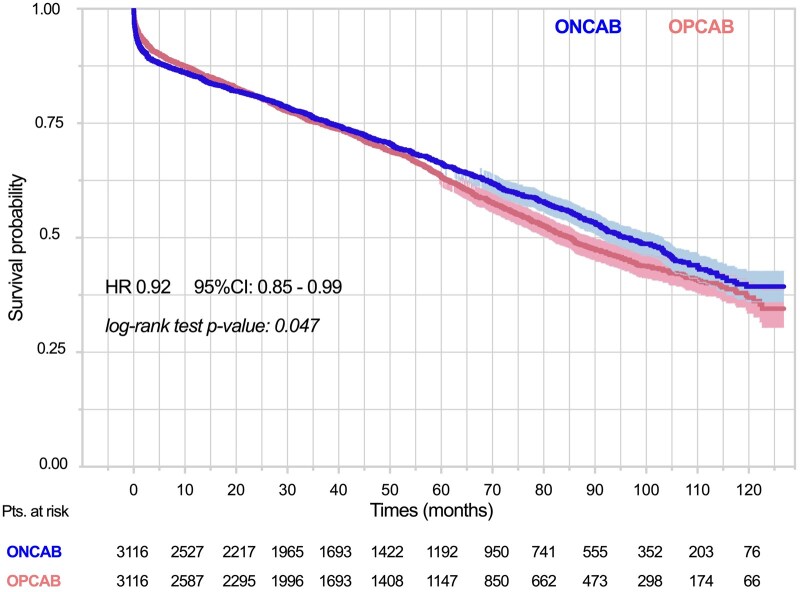 Figure 2
Figure 2| Clinical variables | All patients | Propensity-matched patients | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ONCAB ( | OPCAB ( | SMD | 95% CI |
| ONCAB ( | OPCAB ( | SMD | 95% CI |
| |
| Age, years | 65.93 (8.52) | 66.24 (8.66) | 0.04 | −0.01, 0.08 | 0.078 | 66.23 (8.53) | 66.26 (8.57) | <0.01 | −0.05, 0.05 | 0.89 |
| Male | 4611 (84.0) | 3573 (83.6) | 0.01 | −0.03, 0.05 | 0.57 | 496 (15.9) | 504 (16.2) | −0.01 | −0.06, 0.04 | 0.81 |
| Body mass index | 27.85 (4.45) | 27.81 (4.52) | −0.02 | −0.06, 0.02 | 0.74 | 27.74 (4.49) | 27.7 (4.49) | <0.01 | −0.05, 0.05 | 0.93 |
| EuroSCORE | 4.94 (7.11) | 4.73 (6.54) | −0.02 | −0.06, 0.02 | 0.124 | 4.89 (6.61) | 4.83 (6.39) | 0.01 | −0.04, 0.06 | 0.74 |
| LVEF | 29.84 (5.03) | 29.91 (5.01) | 0.01 | −0.03, 0.05 | 0.48 | 29.88 (4.99) | 29.93 (5.03) | −0.01 | −0.06, 0.04 | 0.67 |
| CCS III | 1692 (30.9) | 16690 (39.2) | 0.17 | 0.13, 0.21 | <0.001 | 1135 (36.4) | 1157 (37.1) | −0.01 | −0.06, 0.03 | 0.56 |
| CCS IV | 1125 (20.6) | 867 (20.4) | 0.01 | −0.03, 0.05 | <0.001 | 659 (21.1) | 653 (21.0) | 0.01 | −0.04, 0.05 | 0.85 |
| Recent myocardial infarction (within 30 days) | 2653 (48.3) | 1866 (43.6) | −0.04 | −0.08, 0.01 | <0.001 | 1479 (47.5) | 1490 (47.8) | −0.07 | −0.57, 0.43 | 0.80 |
| Diseased major coronary arteries | 2.76 (0.5) | 2.46 (0.73) | −0.39 | −0.43, −0.35 | <0.001 | 2.70 (0.52) | 2.70 (0.55) | <0.01 | −0.05, 0.05 | 1.00 |
| Left main stem > 50% | 2099 (38.2) | 1369 (32.0) | −0.08 | −0.12, −0.04 | <0.001 | 1200 (38.5) | 1178 (37.8) | 0.01 | −0.04, 0.06 | 0.58 |
| Preoperative condition | ||||||||||
| Inotropic support | 432 (7.9) | 221 (5.2) | −0.10 | −0.14, −0.06 | <0.001 | 185 (5.9) | 182 (5.8) | <0.01 | −0.05, 0.05 | 0.91 |
| Intravenous nitroglycerin/heparin | 972 (17.7) | 612 (14.3) | −0.08 | −0.12, −0.04 | <0.001 | 522 (16.8) | 520 (16.7) | <0.01 | −0.05, 0.05 | 0.97 |
| Preoperative IABP | 321 (5.8) | 106 (2.5) | −0.16 | −0.19, −0.12 | <0.001 | 75 (2.4) | 77 (2.5) | <0.01 | −0.05, 0.05 | 0.94 |
| Cardiogenic shock | 230 (4.2) | 137 (3.2) | −0.04 | −0.08, −0.01 | 0.013 | 78 (2.5) | 78 (2.5) | <0.01 | −0.05, 0.05 | 0.94 |
| Critical preoperative state | 380 (6.9) | 205 (4.8) | −0.08 | −0.12, −0.04 | 0.000 | 163 (5.2) | 148 (4.7) | 0.02 | −0.03, 0.07 | 0.42 |
| Mechanical ventilation | 97 (1.8) | 46 (1.1) | −0.05 | −0.09, −0.01 | 0.006 | 48 (1.5) | 41 (1.3) | 0.02 | −0.03, 0.07 | 0.52 |
| Comorbidities | ||||||||||
| Renal insufficiency | 609 (1.1) | 553 (12.9) | 0.05 | 0.01, 0.09 | 0.006 | 438 (14.1) | 443 (14.2) | <0.01 | −0.05, 0.05 | 0.88 |
| Smoking | 3685 (67.1) | 2984 (69.8) | 0.06 | 0.02, 0.10 | 0.006 | 2341 (75.1) | 2343 (75.2) | <0.01 | −0.05, 0.05 | 0.98 |
| Chronic lung disease | 593 (10.8) | 457 (10.7) | −0.01 | −0.05, 0.03 | 0.88 | 379 (12.2) | 361 (11.6) | 0.02 | −0.03, 0.07 | 0.51 |
| Arterial hypertension | 4733 (86.2) | 3429 (80.2) | −0.16 | −0.20, −0.12 | <0.001 | 2711 (87.0) | 2731 (87.6) | −0.02 | −0.07, 0.03 | 0.47 |
| Pulmonary hypertension | 579 (10.5) | 508 (11.9) | 0.05 | 0.01, 0.09 | 0.041 | 408 (13.1) | 403 (12.9) | 0.01 | −0.04, 0.06 | 0.8 |
| Hyperlipidaemia | 3745 (68.2) | 2741 (64.1) | −0.11 | −0.13, −0.05 | <0.001 | 2163 (69.4) | 2166 (69.5) | <0.01 | −0.05, 0.05 | 0.96 |
| Diabetes | 2184 (39.8) | 1798 (42.0) | 0.05 | 0.01, 0.09 | 0.025 | 643 (20.6) | 656 (21.1) | −0.06 | −0.11, −0.01 | 0.71 |
| Peripheral artery disease | 1414 (25.8) | 924 (21.6) | −0.11 | −0.15, −0.07 | <0.001 | 603 (19.4) | 615 (19.7) | 0.01 | −0.04, 0.06 | 0.73 |
| Cerebrovascular disease | 328 (6.0) | 273 (6.4) | 0.01 | −0.04, 0.04 | 0.43 | 280 (9.0) | 284 (9.1) | −0.04 | −0.54, 0.45 | 0.90 |
| Stroke | 163 (3.0) | 149 (3.5) | 0.02 | −0.01, 0.06 | 0.168 | 107 (3.4) | 113 (3.6) | −0.01 | −0.06, 0.04 | 0.73 |
| Atrial fibrillation | 501 (9.3) | 437 (11.2) | 0.06 | 0.02, 0.10 | 0.003 | 327 (10.5) | 320 (10.3) | 0.01 | −0.04, 0.06 | 0.80 |
| Urgent surgery | 2155 (39.3) | 1762 (41.5) | 0.05 | 0.01, 0.09 | 0.030 | 1369 (43.9) | 1389 (44.6) | −0.13 | −0.65, 0.37 | 0.63 |
| Clinical variables | All patients | Propensity-matched patients | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ONCAB ( | OPCAB ( | SMD | 95% CI |
| ONCAB ( | OPCAB ( | SMD | 95% CI |
| |
| Number of performed grafts | 2.73 (0.79) | 2.11 (0.94) | 0.72 | 0.68, 0.76 | <0.001 | 2.69 (0.78) | 2.12 (0.91) | 0.68 | 0.63, 0.73 | < 0.001 |
| Arterial grafts | 0.98 (0.50) | 1.15 (0.57) | −0.33 | −0.37, −0.29 | <0.001 | 0.95 (0.47) | 1.09 (0.52) | −0.28 | −0.33, −0.23 | <0.001 |
| BIMA | 158 (2.9) | 199 (4.5) | −0.09 | −0.13, −0.05 | <0.001 | 90 (2.9) | 155 (5.0) | −0.11 | −0.16, −0.06 | <0.001 |
| LIMA | 4303 (99.6) | 381 (99.8) | −0.03 | −0.07, 0.02 | 0.29 | 2446 (99.7) | 2719 (99.9) | −0.04 | −0.10, 0.02 | 0.29 |
| Radial artery | 69 (1.26) | 130 (2.93) | −0.01 | −0.16, −0.15 | <0.001 | 39 (1.25) | 99 (3.17) | −0.01 | −0.21, −0.19 | <0.001 |
| Venous grafts | 1.76 (0.83) | 0.96 (0.87) | 0.94 | 0.89, 0.98 | <0.001 | 1.74 (0.85) | 1.03 (0.90) | 0.81 | 0.76, 0.87 | <0.001 |
| Postoperative outcomes | All patients | Propensity-matched patients | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ONCAB ( | OPCAB ( | OR | 95% CI |
| ONCAB ( | OPCAB ( | OR | 95% CI |
| |
| 30-day mortality | 474 (8.6) | 278 (6.3) | 1.33 | 1.11, 1.58 | 0.002 | 284 (9.1) | 198 (6.4) | 1.39 | 1.13, 1.73 | 0.002 |
| IABP intra- and postoperative | 535 (9.7) | 209 (4.7) | 2.05 | 1.72, 2.43 | <0.001 | 242 (7.8) | 148 (4.7) | 1.49 | 1.16, 1.90 | <0.001 |
| Intraoperative MI | 82 (1.5) | 57 (1.3) | 1.04 | 0.73, 1.48 | 0.81 | 50 (1.6) | 46 (1.5) | 0.95 | 0.63, 1.45 | 0.83 |
| Renal insufficiency | 295 (5.4) | 181 (4.1) | 1.22 | 0.91, 1.64 | 0.173 | 184 (5.9) | 140 (4.5) | 1.18 | 0.89, 1.57 | 0.24 |
| Postoperative dialysis | 213 (3.9) | 145 (3.3) | 0.92 | 0.70, 1.20 | 0.55 | 129 (4.1) | 112 (3.6) | 0.83 | 0.61, 1.15 | 0.27 |
| Gastrointestinal complications | 72 (1.3) | 45 (1.0) | 1.07 | 0.72, 1.58 | 0.73 | 44 (1.4) | 35 (1.1) | 0.96 | 0.56, 1.63 | 0.87 |
| Respiratory complications | 386 (7.0) | 240 (5.4) | 1.20 | 0.99, 1.44 | 0.053 | 241 (7.7) | 193 (6.2) | 1.15 | 0.93, 1.43 | 0.20 |
| Neurological complications | 151 (2.8) | 81 (1.8) | 1.38 | 1.04, 1.83 | 0.024 | 91 (2.9) | 63 (2.0) | 1.32 | 0.94, 1.85 | 0.110 |
| Multiorgan failure | 149 (2.7) | 91 (2.1) | 0.82 | 0.55, 1.21 | 0.32 | 99 (3.2) | 66 (2.1) | 1.35 | 0.91, 2.02 | 0.137 |
| Bleeding/tamponade | 303 (5.5) | 161 (3.6) | 1.18 | 0.84, 1.65 | 0.33 | 172 (5.5) | 124 (4.0) | 1.16 | 0.75, 1.81 | 0.47 |
| Rethoracotomy | 316 (5.8) | 165 (3.7) | 1.29 | 0.92, 1.81 | 0.129 | 178 (5.7) | 129 (4.1) | 1.14 | 0.74, 1.76 | 0.56 |
| Readmission to ICU | 83 (1.5) | 92 (2.1) | 0.58 | 0.42, 0.79 | <0.001 | 52 (1.7) | 68 (2.2) | 0.59 | 0.41, 0.87 | 0.008 |
- —Wroclaw Medical University10.13039/501100009687
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Cardiac and Coronary Surgery Techniques · Mechanical Circulatory Support Devices
INTRODUCTION
Ischaemic cardiomyopathy (ICM) manifests as reduced left ventricle ejection fraction (LVEF) due to acute or acute on chronic coronary artery disease, posing a significant global health challenge [1]. Treatment strategies aim to improve coronary blood flow, relieve symptoms and prevent irreversible myocardial damage. Options include medical therapy, percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG), the latter being the gold standard for selected patients [1–3]. Untreated, ICM progresses to heart failure and death. Heart transplantation is considered the ultimate treatment for end-stage ICM but is limited by donor scarcity. Ventricular assist devices offer temporary or long-term support but have significant drawbacks, including high costs, potential complications such as driveline infections and the need for lifelong anticoagulation therapy, making this option challenging for many patients [1]. The landmark STICH trial evaluated various surgical strategies in ICM patients, demonstrating that despite higher initial risks, CABG offers acceptable early mortality rates and long-term benefits, particularly in those with lower LVEF and markedly dilated left ventricle [2, 4–6]. The STICH Extended Study revealed that combining CABG with pharmacological therapy reduces all-cause mortality by 16% compared to optimal medical therapy alone [7]. Notably, CABG in patients with left ventricular failure not only yields better outcomes than conservative treatment but may also reduce all-cause and cardiac-related mortality and the need for repeat revascularization compared to PCI with drug-eluting stents [8]. The choice between off-pump coronary artery bypass grafting (OPCAB) and on-pump coronary artery bypass grafting (ONCAB) techniques is pivotal in ICM patients. Despite initial enthusiasm, OPCAB’s appeal has waned, particularly in low-risk patients [9, 10]. Nevertheless, valid indications persist, suggesting potential benefit in high-risk scenarios.
This study compares OPCAB and ONCAB techniques in high-risk ICM patients, evaluating their perioperative outcomes and impact on long-term mortality.
MATERIALS AND METHODS
Data source
This retrospective, multicentre cohort study used data from the Polish National Registry of Cardiac Surgery Procedures (KROK) for patients undergoing isolated CABG at cardiac surgery centres in Poland. The registry serves as a comprehensive repository for all cardiac surgeries conducted across Poland. It mandates data transfer from participating centres under the agreement with the Polish Ministry of Health. The registry includes crucial information on patients’ preoperative status, risk factors, operative techniques, perioperative course and early outcomes. Long-term all-cause mortality data were obtained by linking to the National Health System records, ensuring comprehensive follow-up. To maintain strict confidentiality, all data were blinded, preventing the identification of patients and their respective treatment centres. This approach aligns with the highest standards of data protection and ethical research conduct. The study was performed in accordance with the ethical principles outlined in the Declaration of Helsinki. The institutional bioethics committee reviewed the study and officially exempted it from further ethical review due to its retrospective nature and the use of anonymized data from the national registry. Consequently, the requirement for patient consent was waived. Furthermore, the study protocol was found to adhere to all applicable ethical standards for scientific research, reinforcing the integrity of the research methodology and the reliability of the findings.
Study population
The study included patients who underwent primary isolated CABG between January 2012 and July 2022, with preoperative LVEF of ≤35%. Exclusions were: (i) post-myocardial infarction ventricular septal defect, (ii) previous cardiac surgery and (iii) incomplete records. Patients were divided into two groups based on the surgical technique employed: ONCAB and OPCAB. In order to avoid selection bias, we conducted the analysis according to the ‘intention-to-treat’ principle. Patients who were initially assigned to the OPCAB group but were later converted to ONCAB were still analysed within the OPCAB group, preserving the integrity of the original treatment assignment. A flowchart illustrating the study cohort is shown in Fig. 1.
Flowchart of the study cohort
In our study, the term ‘critical preoperative state’ is defined as a condition in which patients require immediate and significant medical interventions prior to undergoing surgery. These interventions may include the administration of intravenous heparin, nitroglycerin, intra-aortic balloon pump (IABP) support or inotropes. Patients categorized as being in a critical preoperative state are typically unstable and may present with life-threatening conditions, necessitating urgent or emergent care to stabilize their condition before revascularization.
This definition distinguishes ‘critical preoperative state’ from ‘urgent revascularization’, which involves procedures performed during the same hospital admission but does not necessarily indicate a life-threatening condition. While patients in urgent revascularization may receive intravenous heparin or nitroglycerin as part of their management, they do not require intensive preoperative interventions such as IABP or inotropes. The patients identified within the ‘critical preoperative state’ category were at a higher risk, as the need for such intensive measures signifies a more severe level of instability.
Study end-points
The primary end-point was long-term all-cause mortality. Secondary end-points included the assessment of grafts performed, postoperative complications, as well as the intensive care unit (ICU) and hospital length of stay. Long-term survival was analysed and compared between the groups without differentiating specific causes of death.
Statistical analysis
Summary statistics were calculated to describe the data, with continuous variables reported as means ± standard deviations and categorical variables expressed as counts and percentages. For cases from the KROK database with up to 5% missing data, the multiple imputation by chained equations (MICE) algorithm was applied to handle missing values. Covariate balance was assessed using standardized mean differences (SMD), with an SMD <0.1 considered indicative of good balance between groups. Overlap assessment involved visually inspecting the propensity score distributions of the ONCAB and OPCAB groups, confirming sufficient common support. Statistical analyses were conducted using the Chi-squared test for qualitative variables and Student’s t-test for quantitative variables, whereas analyses on the matched data using paired tests to account for the dependency introduced by matching. Univariate logistic regression was conducted on both the entire cohort and the matched sample. Kaplan–Meier analysis was used to evaluate long-term survival, with the proportional hazards assumption assessed using scaled Schoenfeld residuals. A two-sided P-value <0.05 was considered statistically significant. All analyses were conducted using R software within the RStudio environment.
RESULTS
A total of 137 060 coronary artery disease surgeries were reported during the study period, with 109 800 patients undergoing isolated CABG. Of these, 9920 patients with a preoperative LVEF of ≤35% were included in the final analysis, of which 44.7% underwent OPCAB. In the OPCAB group, 110 patients (2.5%) required conversion to ONCAB, and the 30-day mortality rate for those converted patients was 25.5%. Detailed preoperative and postoperative characteristics of the entire cohort are presented in Table 1.
After propensity score matching, 3116 patients from the ONCAB group were matched with 3116 patients from the OPCAB group. The ONCAB group had a significantly higher mean number of performed grafts, with a greater use of venous grafts, while the OPCAB group received more arterial and bilateral internal mammary artery (BIMA) grafts. There was no significant difference in the use or left internal mammary artery (LIMA) grafts between the groups (Table 2).
In terms of postoperative outcomes, the ONCAB group demonstrated a significantly higher 30-day mortality rate (9.1% vs 6.4%, P = 0.002; OR 1.39). Additionally, the ONCAB group experienced a higher incidence of intra- or postoperative intraaortic balloon pump (IABP) use. Although not statistically significant, the ONCAB group also exhibited a higher rate of postoperative complications (Table 3). Moreover, the length of ICU stay was significantly longer in the ONCAB group (3.39(6.54) days vs 2.78(5.43) days, P < 0.001), as was the total length of hospital stay (10.15(10.26) days vs 9.59(10.12) days, P < 0.001). The mean follow-up time was similar between the groups, and no significant difference in overall mortality was observed (P = 0.28).
Kaplan–Meier analysis
Kaplan–Meier survival analysis revealed distinct trends over time for the OPCAB and ONCAB groups. At the 1-month mark, the survival rate in the OPCAB group was 94.6% (95% CI: 93.7–95.3), compared to 92.4% (95% CI: 91.6–93.4) in the ONCAB group. By 24 months post-surgery, the survival rates between the two groups had equalized. However, from this point onward, a gradual trend of improved survival emerged in the ONCAB group. At the 10-year follow-up, survival in the OPCAB group was 36.9% (95% CI: 31.1–38.7), while in the ONCAB group, it was 39.4% (95% CI: 36.9–42.3), with a statistically significant difference favouring ONCAB (P = 0.047) (Fig. 2).
Kaplan–Meier survival curves, stratified by surgical strategy, in the matched patient cohort
DISCUSSION
Over the 10-year study period, approximately 110 000 operations for isolated coronary artery disease were conducted in Poland, with 9% of these patients presenting with ICM. Roughly half of this population underwent OPCAB. The findings of this study contribute to the ongoing debate regarding the comparative outcomes of OPCAB and ONCAB in patients with severe left ventricular dysfunction. Despite the advancements in surgical techniques and perioperative care, our results indicate that ONCAB is associated with higher early postoperative risks compared to OPCAB, particularly in terms of 30-day mortality.
Over the years, CABG has shown long-term benefits in patients with ischaemic heart disease, outperforming conservative pharmacological therapy or PCI alone [8, 11, 12]. Early results are acceptable, but perioperative complications affect early survival. The STICH trial indicated that prolonged cardiopulmonary bypass time was the only surgical factor affecting in-hospital outcomes [4]. The choice of surgical strategy in ICM patients remains debated [13–17].
While some studies suggest advantages for OPCAB, recent research show increased risks of haemodynamic instability and urgent conversion to ONCAB in ICM patients [15, 17–20]. In our cohort, the conversion rate was low (2.5%), but the 30-day mortality rate among converted patients was high (25.5%). In contrast, Ueki et al. reported a higher conversion rate (6.1%) but a lower mortality rate (12.5%), while The Society of Thoracic Surgeons data indicated a 5.2% conversion rate with a further reduced mortality of 9.3% [16, 18]. The high mortality in converted patients may be due to haemodynamic instability during surgery.
Numerous studies have investigated the perioperative outcomes in ICM patients [13, 15–18]. OPCAB has been associated with lower incidence of in-hospital mortality, reoperation for bleeding, transfusion requirements, postoperative neurologic events, mediastinitis and prolonged mechanical ventilation [9, 17, 18]. OPCAB has been suggested to be safer in patients with renal insufficiency, potentially resulting in fewer cases of postoperative acute renal failure [21]. In our study, ONCAB was associated with higher 30-day mortality and more frequent readmissions to the ICU. However, long-term survival analysis revealed a slightly significant difference in favour of the ONCAB group at the 10-year follow-up. Zhou et al. [16] reported no significant difference in all-cause mortality, cardiovascular death or major adverse cardiovascular events between OPCAB and ONCAB over 10 years, despite an initial higher perioperative risk in the OPCAB group. Keeling et al. [17] found no differences in early mortality between the groups; however, after risk adjustment, in-hospital mortality was lower in the OPCAB group.
Takagi et al. [22] suggested that incomplete revascularization and worse graft patency may contribute to worse 5-year survival after OPCAB. Similarly, Kim et al. [23] reported worse long-term results after OPCAB. However, Carmona et al. [24] found better early outcomes in OPCAB patients, though no long-term survival benefit. It is important to note that none of these studies categorized patients based on LVEF. Major randomized trials, such as ROOBY and CORONARY, also failed to demonstrate consistent benefits for OPCAB [20, 24]. In the CORONARY trial, the composite outcome of death, stroke, myocardial infarction, renal failure or repeat revascularization at 5 years was similar between OPCAB and ONCAB groups [25]. However, the low number of high-risk ICM patients (<6%) in these studies complicates their analysis. Another meta-analysis showed early mortality reduction after OPCAB surgery in ICM patients, but this benefit did not last in the long term [15].
Our results indicate that OPCAB is associated with a lower 30-day mortality rate, despite a higher incidence of intraoperative conversion to ONCAB. The OPCAB group also experienced shorter ICU and hospital stays, though the ONCAB group tended to show better long-term survival.
Study limitations
As a multicentre registry, the KROK database is not free of limitations related to invalid data entry. Despite continuous efforts to eliminate these shortcomings, adequate validation of the collected data is still necessary before the analysis. In addition, the propensity-matching analysis did not eliminate potential bias; however, this was partially compensated by a large dataset. Additionally, the learning curve implicating surgical experience and its impact on selection bias and outcomes was not assessed in this study. Moreover, data on left ventricular function were limited to LVEF parameters; other parameters such as left ventricular diameter of diastolic dysfunction that might have affected outcomes were not available. Although follow-up was achieved for all patients in our series, due to the verification of deaths in the national registry, we were unable to precisely compare mortality due to cardiovascular causes. Finally, the study lacked access to reintervention data, which could provide valuable insights into long-term survival outcomes.
CONCLUSION
In conclusion, while OPCAB is associated with reduced early postoperative mortality, these short-term advantages do not translate into improved long-term survival. The choice between OPCAB and ONCAB should be individualized, taking into account both short-term and long-term outcomes, as well as factors such as patient-specific risks, comorbidities and surgical expertise. Tailoring the decision to each patient’s unique clinical profile is crucial for optimizing surgical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bakaeen FG , Gaudino M, Whitman G et al; Invited Experts. 2021: The American Association for Thoracic Surgery Expert Consensus Document: coronary artery bypass grafting in patients with ischemic cardiomyopathy and heart failure. J Thorac Cardiovasc Surg 2021;162:829–50.e 1.34272070 10.1016/j.jtcvs.2021.04.052 · doi ↗ · pubmed ↗
- 2Velazquez EJ , Lee KL, Deja MA et al; STICH Investigators. Coronary-artery bypass surgery in patients with left ventricular dysfunction. N Engl J Med 2011;364:1607–16.21463150 10.1056/NEJ Moa 1100356 PMC 3415273 · doi ↗ · pubmed ↗
- 3Neumann FJ , Sousa-Uva M, Ahlsson A et al; ESC Scientific Document Group. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J 2019;40:87–165.30165437
- 4Wrobel K , Stevens SR, Jones RH et al Influence of baseline characteristics, operative conduct, and postoperative course on 30-day outcomes of coronary artery bypass grafting among patients with left ventricular dysfunction: results from the Surgical Treatment for Ischemic Heart Failure (STICH) trial. Circulation 2015;132:720–30.26304663 10.1161/CIRCULATIONAHA.114.014932 PMC 4551105 · doi ↗ · pubmed ↗
- 5Panza JA , Velazquez EJ, She L et al Extent of coronary and myocardial disease and benefit from surgical revascularization in ischemic LV dysfunction [corrected]. J Am Coll Cardiol 2014;64:553–61.25104523 10.1016/j.jacc.2014.04.064PMC 4129547 · doi ↗ · pubmed ↗
- 6Mahesh B , Peddaayyavarla P, Ong LP et al Cardiac surgery improves survival in advanced left ventricular dysfunction: multivariate analysis of a consecutive series of 4491 patients over an 18-year period. Eur J Cardiothorac Surg 2016;50:857–66.27165769 10.1093/ejcts/ezw 134 · doi ↗ · pubmed ↗
- 7Velazquez EJ , Lee KL, Jones RH et al; STICHES Investigators. Coronary-artery bypass surgery in patients with ischemic cardiomyopathy. N Engl J Med 2016;374:1511–20.27040723 10.1056/NEJ Moa 1602001 PMC 4938005 · doi ↗ · pubmed ↗
- 8Kang SH , Lee CW, Baek S et al Comparison of outcomes of coronary artery bypass grafting versus drug-eluting stent implantation in patients with severe left ventricular dysfunction. Am J Cardiol 2017;120:69–74.28483202 10.1016/j.amjcard.2017.03.261 · doi ↗ · pubmed ↗