Pitfalls of Intraoperative Parathyroid Hormone Monitoring in Achieving Complete Surgical Resection of Ectopic Mediastinal Parathyroid Adenoma: A Case Report and Literature Review
Wakako Nagase, Yujin Kudo, Jun Matubayashi, Ryosuke Amemiya, Maki Tanigawa, Yoshihisa Shimada, Masaru Hagiwara, Masatoshi Kakihana, Toshitaka Nagao, Tatsuo Ohira, Norihiko Ikeda

TL;DR
This case report discusses the use of intraoperative parathyroid hormone monitoring in the surgical removal of a rare mediastinal parathyroid adenoma and highlights the importance of combining it with other diagnostic methods.
Contribution
The paper presents a successful case of using intraoperative parathyroid hormone monitoring and emphasizes the need for additional diagnostic methods to ensure complete tumor removal.
Findings
Intraoperative parathyroid hormone monitoring showed a 22% decrease in hormone levels after resection.
Pathological analysis confirmed complete resection of the ectopic mediastinal parathyroid adenoma.
Postoperative serum parathyroid hormone and calcium levels rapidly decreased with no recurrence observed.
Abstract
Ectopic mediastinal parathyroid adenoma is rare and is generally managed by surgical resection as a definitive treatment. Intraoperative parathyroid hormone (ioPTH) monitoring is valuable for ensuring the complete removal of a target lesion. However, there is no consensus criteria regarding the utilization of ioPTH for complete resection in patients with ectopic mediastinal parathyroid adenomas. A 65-year-old woman presented with asymptomatic hypercalcemia, and was subsequently diagnosed as having hyperparathyroidism. Radiological imaging displayed a solid mediastinal tumor, suspected to be ectopic mediastinal parathyroid adenoma. Surgical resection was performed together with ioPTH monitoring. Although a transient increase in intact parathyroid hormone (iPTH) level was noted, a 22% decrease in iPTH level compared with the preoperative peak iPTH level was observed 30 minutes after the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
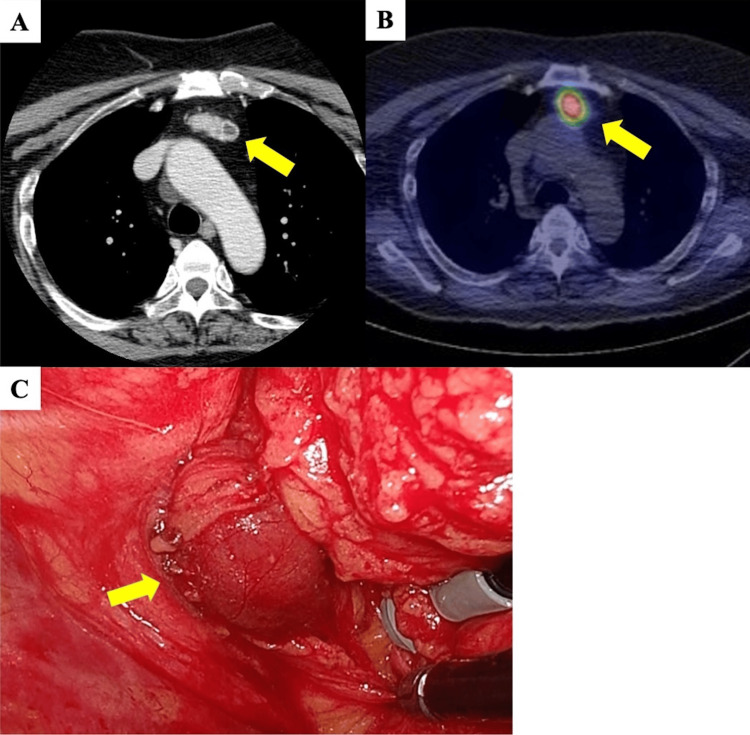 Figure 1
Figure 1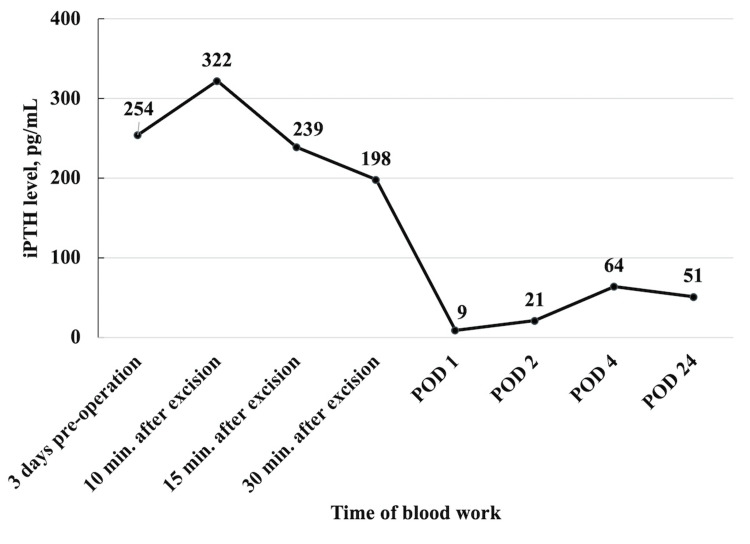 Figure 2
Figure 2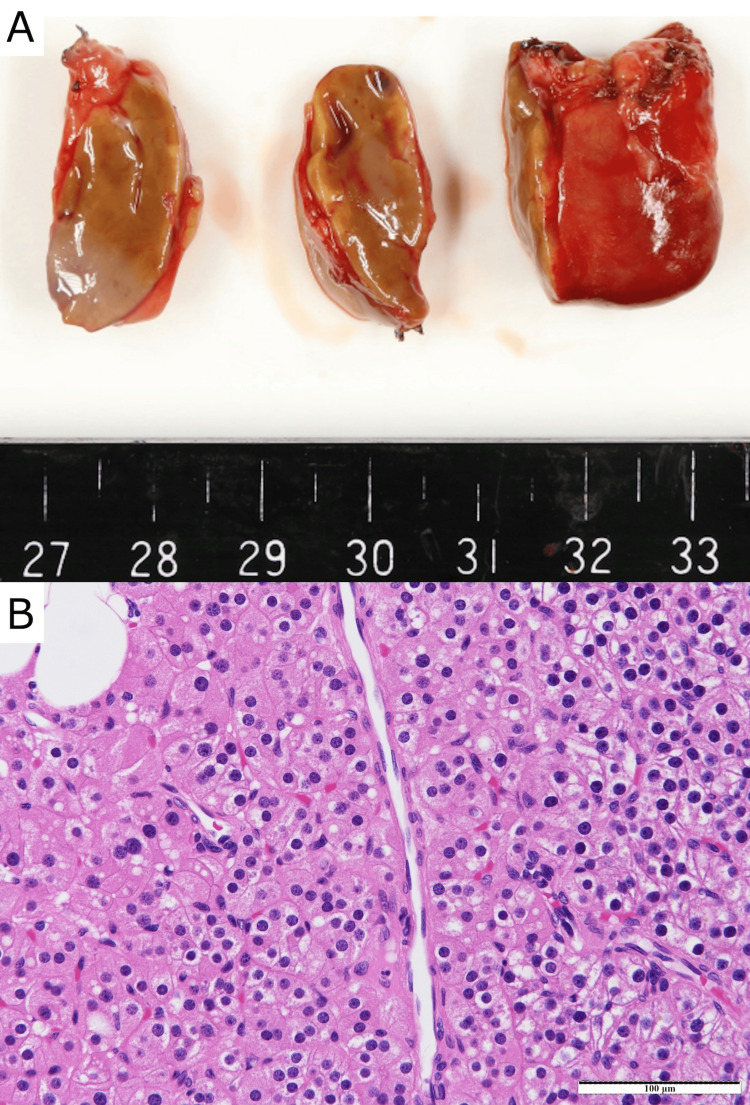 Figure 3
Figure 3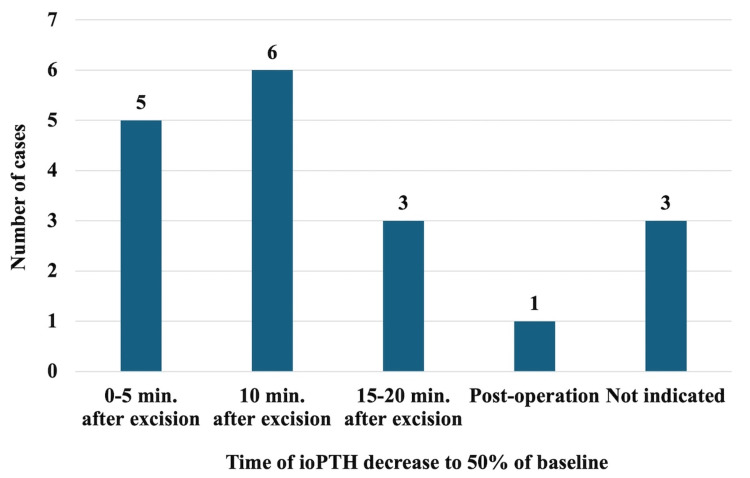 Figure 4
Figure 4| Complete blood count | Normal range | ||
| White blood cells | 6,900 | 2,700-8,800 | /μl |
| Red blood cells | 370x104 | 370-540x104 | /μl |
| Platelet | 21x104 | 14-34.0x104 | /μl |
| Blood chemistry | |||
| AST | 16 | 8-38 | U/l |
| ALT | 15 | 4-44 | U/l |
| LDH | 146 | 106-211 | U/l |
| γ-GTP | 30 | 16-73 | U/l |
| ALP | 156 | 104-338 | U/l |
| T-Bil | 0.37 | 0.20-1.20 | mg/dl |
| Alb | 4.2 | 3.9-4.9 | g/dl |
| Glu | 90 | 60-110 | mg/dl |
| BUN | 19.9 | 8.0-22.6 | mg/dl |
| Cre | 0.86 | 0.40-0.80 | mg/dl |
| eGFR | 51.0 | ml/min/1.73m2 | |
| Na | 141 | 138-148 | mmol/l |
| Cl | 110 | 98-108 | mmol/l |
| K | 4.5 | 3.6-5.2 | mmol/l |
| Ca | 12.7 | 8.2-10.2 | mg/dl |
| P | 1.9 | 2.5-4.7 | mg/dl |
| CRP | <0.02 | <0.30 | mg/dl |
| Endocrine examination | |||
| Intact-PTH | 331 | 10-65 | pg/ml |
| TSH | 1.81 | 0.50-5.00 | μIU/ml |
| FT3 | 2.38 | 2.30-4.30 | pg/ml |
| FT4 | 1.23 | 0.90-1.70 | ng/dl |
| No. | Study | Year | No. of patients | Age (years) | Sex | Tumor location in mediastinum | Surgical approach | Diagnosis | iPTH Reduction ratea | Time of blood work after tumor excision |
| 1 | O’Herrin et al. [ | 2002 | 1 | 43 | F | Anterior | VATS | Hypercellular parathyroid | 87% | 5 min |
| 2 | Luncă at al. [ | 2004 | 1 | 44 | F | Middle | Sternotomy | Parathyroid adenoma | 70% | 20 min |
| 3 | Profanter at al. [ | 2004 | 1 | 57 | F | Superior | RATS | Parathyroid adenoma | 84% | 10 min |
| 4 | Amar et al. [ | 2004 | 2 | 36 | F | Anterior | VATS | Parathyroid tumor | 97% | Not indicated |
| 57 | F | Anterior | VATS | Adenoma or hyperplasia | 78% | Not indicated | ||||
| 5 | Wild et al. [ | 2006 | 1 | 65 | M | Anterior | VATS | Adenoma | 30% | 5 minb |
| 6 | Moreno et al. [ | 2007 | 1 | 69 | F | Middle | VATS | Parathyroid gland | 95% | Post operation |
| 7 | Kim et al. [ | 2014 | 1 | 59 | F | Anterior | VATS | Parathyroid adenoma | 94% | Not indicated |
| 8 | Schwarzlmüller et al. [ | 2014 | 2 | 72 | F | Middle | Sternotomy | Adenoma | 96% | 10 min |
| 79 | F | Middle | Sternotomy | Adenoma | 97% | 10 min | ||||
| 9 | Dinga Madou et al. [ | 2016 | 1 | 55 | F | Middle | Sternotomy | Adenoma | 68% | 0 min |
| 10 | Elhelf et al. [ | 2017 | 1 | 58 | M | Superior | Mediastinoscopy | Hypercellular parathyroid tissue with minute thymic remnant | 57% | 10 min |
| 11 | Ishikawa et al. [ | 2017 | 1 | 66 | F | Superior | VATS | Adenoma | 85% | 10 min |
| 12 | Mitsuboshi et al. [ | 2019 | 1 | 67 | F | Anterior | Thoracotomy | Adenoma | 87% | 15 min |
| 13 | Medbery et al. [ | 2019 | 1 | 61 | M | Posterior | Thoracotomy | Adenoma | 73% | 5 min |
| 14 | Miller et al. [ | 2019 | 1 | 53 | M | Posterior | Transcervical | Adenoma | 53% | 5 min |
| 15 | Iijima et al. [ | 2022 | 1 | 53 | F | Anterior | RATS | Adenoma | 52% | 15 min |
| 16 | Akin et al. [ | 2022 | 1 | 48 | F | Superior | Transcervical | Adenoma | 86% | 10 min |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Genetic Syndromes and Imprinting · Thyroid and Parathyroid Surgery
Introduction
The prevalence of ectopic mediastinal parathyroid adenoma is reported to be 1% to 2% of parathyroid adenomas [1, 2]. Hyperactive tissues within the ectopic lesions secrete an excess amount of parathyroid hormone (PTH), leading to hyperparathyroidism. This condition can result in hypercalcemia or bone mineral disorders, presenting symptoms such as fatigue, bone pain, kidney stones, and gastrointestinal disturbances. Surgical treatment is the first choice for symptomatic primary hyperparathyroidism (pHPT) or asymptomatic pHPT with associated complications [3, 4]. It is particularly noteworthy that in this disease hyperparathyroidism can persist in some patients even after treatment. Furthermore, surgical management techniques that are required for these patients might be unfamiliar to thoracic surgeons who have limited experience with this disease.
Inadequate resection of the hyperfunctioning parathyroid gland is a major issue in surgical treatment for ectopic mediastinal parathyroid adenoma, which can result in inefficient postoperative improvement of pHPT. It may be difficult to identify active parathyroid glands intraoperatively, particularly when they are located deep within the mediastinum or thymus. Intraoperative parathyroid hormone (ioPTH) monitoring has been reported to be a valuable technique for confirming complete tumor resection [5-11]. Although the technique is widely used, and various criteria for the use of ioPTH monitoring have been proposed, a universally accepted method has not yet been established. Therefore, understanding the pitfalls of this technique is crucial to making an accurate decision of complete resection of the responsible tumor. We here report a case of successful thoracoscopic removal of an ectopic mediastinal parathyroid adenoma using ioPTH monitoring, together with a review of previously reported cases.
Case presentation
A 65-year-old woman presented with asymptomatic hypercalcemia that was identified during a routine medical check-up. She had a past medical history of kidney stones, cerebrovascular disease, hypertension, arrhythmia, and hyperlipidemia. Laboratory examination results included a serum calcium level of 12.7 mg/dL, serum phosphate concentration of 1.9 mg/dL, serum alkaline phosphatase activity of 156 IU/L, serum albumin level of 4.2 g/dL, and serum intact parathyroid hormone (iPTH) level of 331 pg/mL. Her renal function was within the normal range, with a serum creatinine level of 0.86 mg/dL and an estimated glomerular filtration rate (eGFR) of 51.0 (mL/min/1.73 m^2^) (Table 1). Her bone density measured by dual-energy X-ray absorptiometry scan demonstrated a young adult mean of 73%. From these results, she was diagnosed as having primary hyperparathyroidism.
Chest computed tomography displayed a 3.3 x 1.4 cm solid mass containing a cyst in the anterior mediastinum (Figure 1A). Technetium-99m-methoxy-isobutyl-isonitrile scintigraphy displayed increased uptake within the mass (Figure 1B). Ultrasound examination of the thyroid did not display any visibly enlarged parathyroid glands. Based on these findings, the lesion was suspected to be an ectopic mediastinal parathyroid tumor, which was causing the pHPT. Surgical resection of the anterior mediastinal tumor was performed using the 4-port video-assisted thoracoscopic surgery (VATS) approach. Intraoperatively, it was initially difficult to identify the tumor owing to the abundant mediastinal fat tissue and the limited space in the anterior thoracic cavity. The phrenic nerve was preserved, and the tumor was identified in the thymic tissue (Figure 1C).
Chest computed tomography (CT) and technetium-99m-methoxy-isobutyl-isonitrile (99mTc-MIBI) scintigraphy and intraoperative findings of the patient(A) Chest CT displayed a 3.3 x 1.4-cm solid mass containing a cyst in the anterior mediastinum (yellow arrow); (B) 99mTc-MIBI scintigraphy displayed increased uptake within the mass (yellow arrow); (C) A round tumor was observed in the anterior mediastinum (yellow arrow).
The tumor was resected en bloc along with the surrounding mediastinal fatty tissue. There is a possibility that the tumor, together with the mediastinal fatty tissue, was compressed when trying to obtain a clear view of the operative field to safely identify the anatomical landmarks.. The levels of ioPTH were measured by drawing peripheral blood at four-time points, namely, five minutes, 10 minutes, 15 minutes, and 30 minutes after removing the ectopic parathyroid tumor. There was a transient increase in the level of ioPTH from 254 to 322 pg/mL five minutes after the resection of the ectopic parathyroid tumor. However, the ioPTH level decreased thereafter, and a 22% reduction compared with the preoperative iPTH level was observed 30 minutes after tumor resection. Details of the iPTH levels are shown in Figure 2. Intraoperative frozen section diagnosis confirmed that the lesion was an ectopic mediastinal parathyroid adenoma.
Results of iPTH measurementsA 22% decrease in iPTH level compared with the preoperative iPTH level was observed at 30 minutes after excision of the parathyroid gland. The iPTH level immediately decreased to within the normal range on postoperative day 1.
Glossy, the excised tumor measured 3.3×2.3×1 cm in size and appeared to be a well-circumscribed mass with a thin fibrous capsule (Figure 3A). Microscopically, the tumor was composed of cells arranged in cord- and nest-like fashion. Many tumor cells with small round nuclei and clear or eosinophilic cytoplasms were observed (Figure 3B). Therefore, the lesion was pathologically diagnosed as parathyroid adenoma. On the day after the operation, the patient’s iPTH level immediately decreased to within the normal range. The patient’s serum calcium level improved to 9.8 mg/dL on the second day after the operation. No signs of hypocalcemia were detected upon careful monitoring. The patient was discharged without any postoperative complications. There was no occurrence of hypocalcemia during the postoperative follow-up period of 1.5 years.
Macroscopic and microscopic appearance of the tumor(A) Glossy, the excised tumor measured 3.3×2.3×1 cm in size and appeared to be a well-circumscribed mass with a thin fibrous capsule; (B) Microscopically, the tumor was composed of cells arranged in cord- and nest-like fashion. Many tumor cells with small round nuclei and clear or eosinophilic cytoplasms were observed. (Hematoxylin–Eosin staining, × 200 magnification).
Discussion
In the present case, the patient had an ectopic mediastinal parathyroid tumor and presented with primary hyperparathyroidism, and the tumor was resected by VATS together with ioPTH monitoring. Unexpectedly, intraoperative manipulation and compression of the tumor resulted in an initial temporary increase in iPTH level, and the expected significant decrease in iPTH level after resection was not observed. The surgery was completed after intraoperative frozen section analysis confirmed that tumor resection was complete, and the iPTH level decreased on postoperative day one. Our present case demonstrates that upon resection of an ectopic mediastinal parathyroid tumor in a patient with primary hyperparathyroidism, it is crucial to minimize manipulation of the tumor, as compression of the tumor can cause an increase in iPTH level, leading to unreliable intraoperative monitoring results.
The use of ioPTH monitoring has been demonstrated to be beneficial for the resection of ectopic mediastinal parathyroid adenomas [9-12]. Sagan et al. demonstrated the utility of ioPTH monitoring, demonstrating a decrease in the potential failure rate from 21.2% without ioPTH monitoring to an actual 3% when ioPTH was utilized during the surgery [9]. Monitoring of ioPTH provides surgeons with a real-time assessment of parathyroid function and helps to ensure complete removal of the responsible lesion. Although ioPTH monitoring is routinely used and there are several criteria, there are no established standard criteria that have achieved universal consensus. Prior studies have demonstrated a decrease in ioPTH level of more than 50% from the baseline as a valuable criterion for complete resection of primary parathyroid tumors [13, 14]. With regard to ioPTH monitoring, particularly for mediastinal parathyroid tumors, there is no consensus on the degree and timing of PTH reduction that indicates successful surgery.
We performed a literature review of patients who underwent ectopic mediastinal parathyroid tumor resection together with ioPTH monitoring. A literature search was conducted with the keywords [(parathyroid adenoma) OR (parathyroid tumor)] AND (mediastinum OR mediastinal OR (ectopic mediastinal)] by a medical subject heading (MeSH) search in PubMed®. The time frame was set from 1996 to 2023 because rapid PTH measurement became commercially available in 1996. Of the 384 case reports identified, we selected appropriate cases as follows: (1) surgically resected mediastinal parathyroid tumors with ioPTH monitoring reported in detail, (2) reports with less than two cases to avoid overlapping reports, (3) articles in English.
In our comprehensive literature review, a total of 18 cases were identified and analyzed (details are shown in Table 2). The extent of ioPTH reduction and the timing of ioPTH sampling are particularly noteworthy. We found that 17 patients showed a reduction in ioPTH levels by more than 50% from the initial levels. The decrease was approximately 80% to 90% in most cases. There was one patient (case five) in whom the ioPTH reduction rate was less than 50% after the initial resection of pericardial fat tissue in the anterior mediastinum. Consequently, further neck exploration was performed, resulting in the excision of an enlarged parathyroid gland and a 67% reduction in ioPTH levels five minutes post-excision. In such cases, the use of the “Wisconsin Criteria” is recommended, which requires that the PTH value is at least 50% lower than the pre-excision level at either five, 10, or 15 minutes post-excision if the PTH at five minutes is increased from the baseline, that number becomes the “new baseline”, and a sample is drawn 20 minutes from this timepoint [15]. However, in our present case, a transient increase in ioPTH levels was observed, without a marked subsequent decrease during the operation. This could be caused by inadvertent compression of the tumor owing to the presence of abundant mediastinal fat during the surgery.
Another crucial factor is the timing of the blood tests. As shown in Figure 4, the most common time at which ioPTH levels were observed to decrease to below 50% of the baseline was five to 10 minutes after tumor resection. This was owing to the inherent characteristic of PTH having a short half-life (about three to five minutes) [3]. Previous reports have indicated potential pitfalls in ioPTH monitoring. An increase in the ioPTH level five minutes after tumor resection, or an ioPTH spike may result in false-negative results of ioPTH monitoring [15-17]. In our patient, ioPTH levels were measured up to 30 minutes after tumor resection, but no decrease below 50% of the baseline was observed. However, due to the findings of preoperative imaging suggesting a single responsible active gland and the diagnosis of a pathological frozen section diagnosis confirming complete resection of the tumor, we considered that the surgery was accomplished. Studies have mentioned that when pressure is applied to a parathyroid gland, it triggers the release of hormones, leading to an elevation in peripheral blood levels [5]. The transient increase in ioPTH levels above the preoperative baseline in this patient was likely caused by compression of the tumor during surgery, which subsequently decreased over time.
Timepoints at which ioPTH values decreased to below 50% of baseline (pre-operation or pre-excision) in cases from the literature reviewThe most common time to observe a decrease in ioPTH levels to below 50% of baseline was 5 to 10 minutes after tumor excision.
Conclusions
We successfully resected an ectopic mediastinal parathyroid adenoma from a patient, but a sufficient reduction in ioPTH level could not be confirmed intraoperatively. Although ioPTH monitoring is an important indicator of the complete resection of ectopic mediastinal parathyroid adenomas, it is very important to be aware that the surgical technique has the potential to inadvertently increase ioPTH levels, which may make the evaluation difficult. Serum PTH has a short half-life of three to five minutes, necessitating a comprehensive evaluation of the result. Careful ioPTH monitoring procedures and appropriate surgical techniques are the key to the successful treatment of ectopic mediastinal parathyroid adenomas.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence and location of ectopic abnormal parathyroid glands Am J Surg Phitayakorn R Mc Henry CR 41842319120061649055910.1016/j.amjsurg.2005.10.049 · doi ↗ · pubmed ↗
- 2The anatomic basis of parathyroid surgery Ann Surg Wang C 2712751831976125948310.1097/00000658-197603000-00010 PMC 1344236 · doi ↗ · pubmed ↗
- 3The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism JAMA Surg Wilhelm SM Wang TS Ruan DT 95996815120162753236810.1001/jamasurg.2016.2310 · doi ↗ · pubmed ↗
- 4Ectopic parathyroid glands and their anatomical, clinical and surgical implications Exp Clin Endocrinol Diabetes Noussios G Anagnostis P Natsis K 60461012020122317499510.1055/s-0032-1327628 · doi ↗ · pubmed ↗
- 5Improved success rate in reoperative parathyroidectomy with intraoperative PTH assay Ann Surg Irvin GL 3rd Molinari AS Figueroa C Carneiro DM 87487822919991036390210.1097/00000658-199906000-00015 PMC 1420835 · doi ↗ · pubmed ↗
- 6Intraoperative parathyroid hormone testing improves cure rates in patients undergoing minimally invasive parathyroidectomy Surgery Chen H Pruhs Z Starling JR Mack E 58358713820051626928510.1016/j.surg.2005.06.046 · doi ↗ · pubmed ↗
- 7Value of intraoperative parathyroid hormone monitoring Ann Surg Oncol Sharma J Milas M Berber E Mazzaglia P Siperstein A Weber CJ 4934981520081802679710.1245/s 10434-007-9683-2 · doi ↗ · pubmed ↗
- 8Worldwide trends in the surgical treatment of primary hyperparathyroidism in the era of minimally invasive parathyroidectomy Arch Surg Sackett WR Barraclough B Reeve TS Delbridge LW 1055105913720021221516010.1001/archsurg.137.9.1055 · doi ↗ · pubmed ↗