Surviving the Deadly Triad: Two Cases of Austrian Syndrome in Southern Switzerland, Associated With Disseminated Streptococcus pneumoniae Infection
Valentina Guerini Giusteri, Marco Bongiovanni, Enos Bernasconi, Marco Pons

TL;DR
This paper presents two rare cases of Austrian syndrome in Switzerland, highlighting the severe complications of Streptococcus pneumoniae infections and the need for combined medical and surgical treatment.
Contribution
The paper contributes two detailed clinical cases of Austrian syndrome with disseminated S. pneumoniae infection, emphasizing the importance of early diagnosis and vaccination.
Findings
Austrian syndrome was diagnosed in two patients with severe complications including meningitis, endocarditis, and septic arthritis.
Both patients had S. pneumoniae isolated from multiple sites and required intensive treatment with antibiotics and surgery.
The cases underscore the importance of vaccination to prevent invasive pneumococcal disease.
Abstract
Austrian syndrome is a rare and life-threatening condition. It is more severe in immunocompromised patients, those with comorbidities, or harmful alcohol consumption. The etiopathogenesis involves hematogenous seeding of Streptococcus pneumoniae and local spread in the infected tissues, presenting with pneumonia, endocarditis, and meningitis. A 68-year-old man was hospitalized for impaired consciousness, left hemiparesis, and aphasia, consistent with meningoencephalitis. A CT scan showed otomastoiditis and bilateral pulmonary consolidations with respiratory failure. A transesophageal echocardiogram revealed endocardial vegetations at the mitral-aortic junction and left ventricular outflow tract, requiring aortic valve replacement. He also developed septic arthritis in both prosthetic hips and bilateral muscular abscesses. The second patient is a 50-year-old man who was hospitalized for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
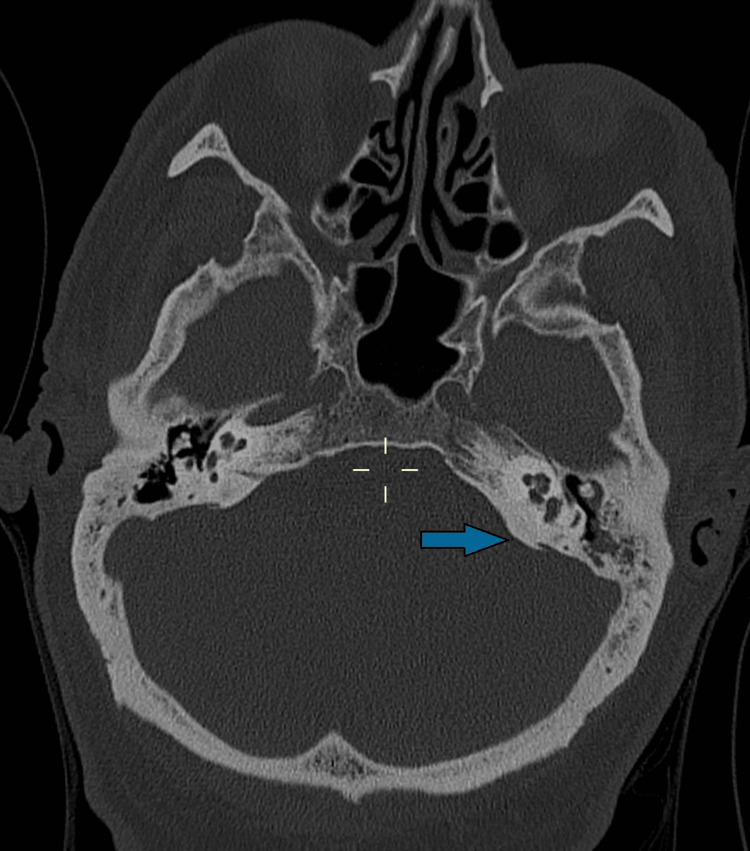 Figure 1
Figure 1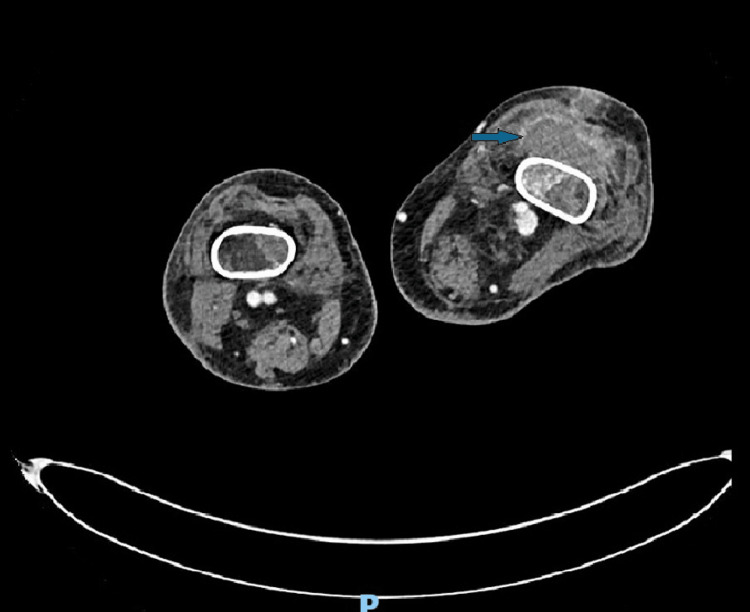 Figure 2
Figure 2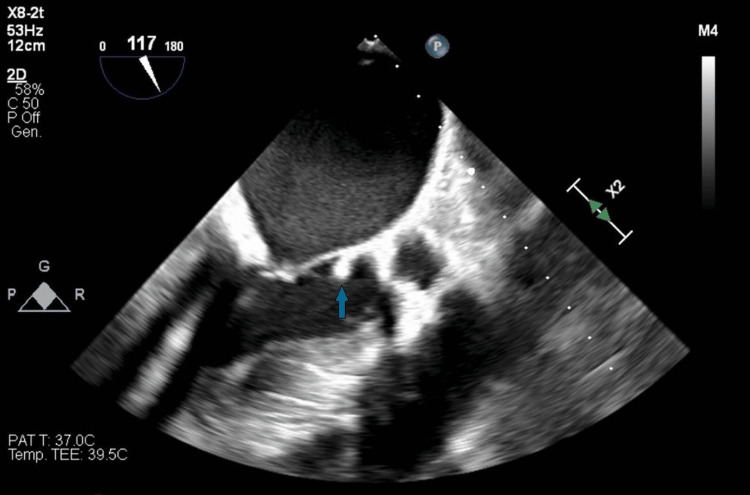 Figure 3
Figure 3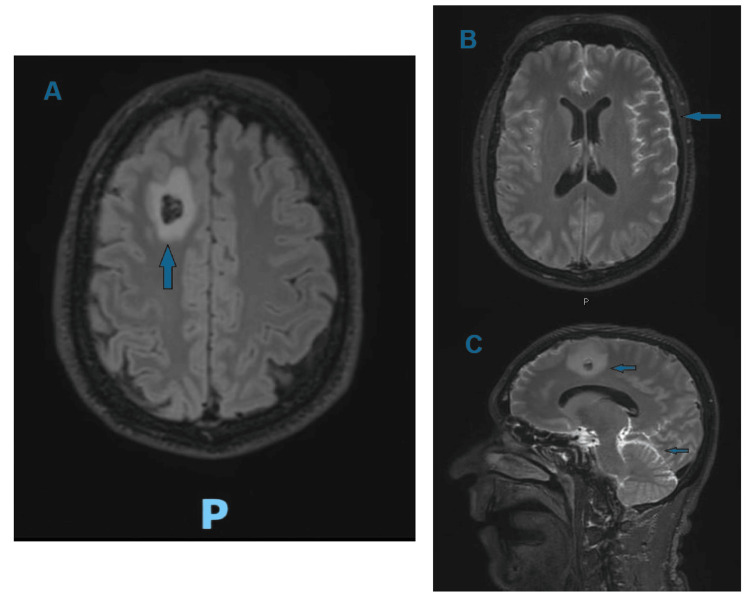 Figure 4
Figure 4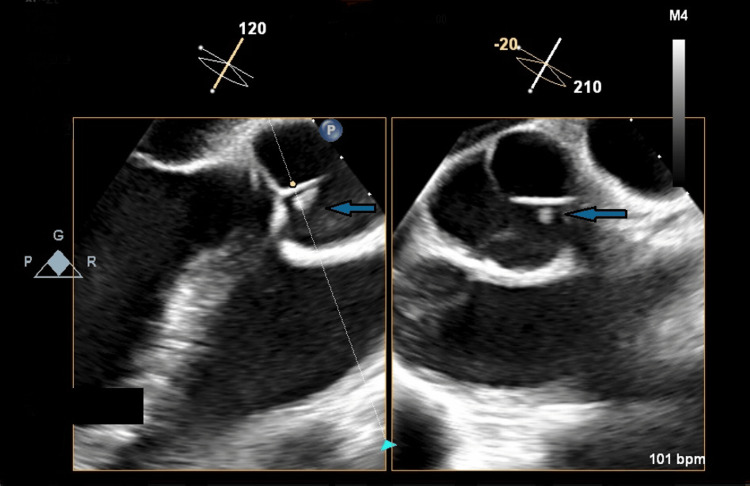 Figure 5
Figure 5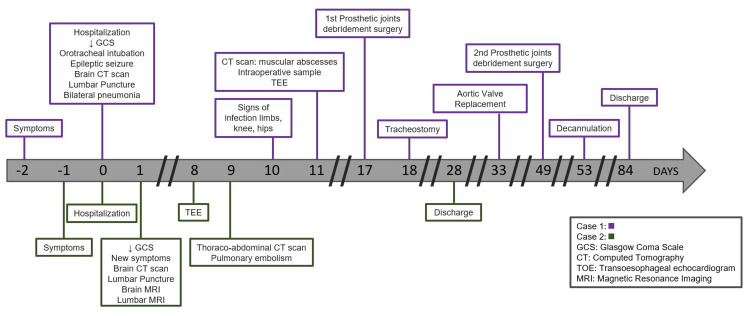 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Infective Endocarditis Diagnosis and Management · Bacterial Infections and Vaccines
Introduction
Austrian syndrome is a condition that involves the triad of meningitis, pneumonia, and endocarditis, caused by Streptococcus pneumoniae. It is a life-threatening clinical condition, and early diagnosis can be challenging. In fact, it carries a high mortality rate, ranging from 20% to 40%, despite aggressive combined medical and surgical management. The exact incidence is not well established, as it depends on various factors such as geographic location, serotype prevalence, and the patient’s comorbidities [1]. The condition has become rarer due to early treatment with penicillin and other beta-lactam antibiotics, as well as the introduction of pneumococcal vaccines [2]. It is classified as a pneumococcal invasive disease (IPD), which consists of the development of pneumococcal infection in normally sterile sites. It tends to be more severe in vulnerable individuals, such as immunocompromised patients, persons with harmful alcohol consumption, and those with multiple comorbidities, such as chronic lung diseases, heart failure, and diabetes mellitus [3]. The main mechanism of occurrence of this condition is thought to be through hematogenous seeding and local spread. However, the development of meningitis, due to pneumococcal crossing of the blood-brain barrier after bloodstream invasion, may be enabled by the release of inflammatory mediators [4].
This report describes two cases of Austrian syndrome that occurred in Southern Switzerland in 2024, characterized by multiple complications and septic emboli, but with a favorable outcome despite prolonged hospitalization.
Case presentation
Case 1
A 68-year-old man was hospitalized with progressively impaired consciousness, left hemiparesis, and aphasia, which began two days prior. His medical history included permanent atrial fibrillation, third-degree atrioventricular block requiring the implantation of a Micra® pacemaker, moderate aortic stenosis, non-ischemic heart failure with mildly reduced ejection fraction, type 2 diabetes, hypertension, obstructive sleep apnea syndrome with nocturnal Continuous Positive Airway Pressure (CPAP), bilateral hip and left knee replacements, and alcohol consumption (4-6 alcohol units per day). His therapy included a direct oral anticoagulant (rivaroxaban), antihypertensive drugs (valsartan, hydrochlorothiazide, amlodipine, torsemide), and oral hypoglycemic medications (metformin and sitagliptin). The patient's Glasgow Coma Scale (GCS) deteriorated to 8 (E3 V1 M4, eye-opening to verbal command, no verbal response, motor response withdraws to pain), requiring orotracheal intubation, and he experienced a concomitant epileptic seizure, for which diazepam (dosage: 10 mg intravenous, administered only once) and levetiracetam (dosage: 1500 mg every 12 hours) were administered. A brain CT scan ruled out hydrocephalus and showed no signs of hemorrhage or ischemia. However, a chest CT scan revealed bilateral pulmonary consolidations. Given the suspicion of meningoencephalitis, due to turbid CSF observed during lumbar puncture (with >1000 leukocytes/µl, predominance of polymorphonuclear cells, glucose 4.9 mmol/l, proteins 1123 mg/dl), empirical therapy with dexamethasone (dosage: 10 mg every 6 hours), ceftriaxone (dosage: 2 g every 12 hours), ampicillin (dosage: 2 g every 4 hours), and linezolid (dosage: 600 mg every 12 hours) was initiated. S. pneumoniae susceptible to penicillin was isolated from both CSF and bronchial aspirate. Treatment was therefore continued with dexamethasone and ceftriaxone. Due to the onset of septic shock, a total body CT scan documented otomastoiditis, identifying the primary source of infection (Figure 1).
CT scan showing left otomastoiditis.
A few days later, the patient developed edema of the left lower limb and of the left knee, along with signs of infection in both hips. A CT scan showed bilateral muscular abscesses (Figure 2): one in the right thigh and five in the left limb (sites: left anterior tibial muscle, left posterior tibial muscle, gastrocnemius and soleus, long flexor of the toes extended to the dorsum of the left foot, and the distal third of the left thigh to the dorsomedial subcutaneous fat of the left calf).
CT scan showing one of multiple muscular abscesses.
The spectrum of the antibiotic therapy was empirically extended with meropenem (dosage: 2 g every 8 hours) and vancomycin (loading dose 1500 mg, then 1250 mg every 12 hours) before the 16S ribosomal polymerase chain reaction from diagnostic knee arthrocentesis confirmed the presence of the same S. pneumoniae. Intraoperative samples from both hips and the left knee also revealed S. pneumoniae, confirming the diagnosis of septic arthritis in the prosthetic joints. Due to the high operative risk associated with prosthesis replacement, the patient underwent debridement surgery, which was repeated twice due to the recurrence of infection at the same sites. A transesophageal echocardiogram was also performed, revealing endocardial vegetations at the mitral-aortic junction and left ventricular outflow tract (Figure 3), with moderate aortic insufficiency, thus confirming Austrian syndrome.
Transesophageal echocardiogram showing vegetation at the mitral-aortic junction.
Hence, given the absence of neurological contraindications on brain MRI, the patient underwent aortic valve replacement without complications. During the prolonged hospitalization, the patient developed several complications including critical illness polyneuropathy, fluctuating neurological status, and delirium, managed with quetiapine, all complicating the gradual weaning from mechanical ventilation, requiring a temporary percutaneous tracheostomy. The patient's condition gradually improved, and the antibiotic regimen was switched to oral amoxicillin (at a dosage of 1 g every 8 hours), to be continued in the long term. The patient was finally discharged to a rehabilitation center after two months of hospitalization.
Case 2
A 50-year-old man with no notable medical history was hospitalized for lumbar back pain, three syncopal episodes, and fever. All symptoms began the day before, and he had taken 600 mg of ibuprofen for pain relief. The patient’s GCS rapidly deteriorated over the day to 10 (E4 V1 M5, meaning spontaneous eye opening, no verbal response, motor response makes purposeful movement to noxious stimuli), associated with vomiting, aphasia, left-sided neglect, and motor deficit in the right lower limb. Suspecting a spondylodiscitis rapidly complicating with the onset of septic shock, an empirical treatment with cefepime (dosage: 2 g every 8 hours) and vancomycin (loading dose 1750 mg, then 1000 mg every 12 hours) was initiated. A brain CT scan revealed a hyperdense area in the right frontal region with surrounding edema, and a lumbar puncture showed turbid cerebrospinal fluid (with 155 leukocytes/µl, predominance of polymorphonuclear cells, glucose 0.2 mmol/l); S. pneumoniae susceptible to penicillin (serotype 15C) was isolated from both CSF and blood cultures, so the antibiotic treatment was continued with ceftriaxone (dosage: 2 g every 12 hours). An electroencephalogram ruled out an epileptic seizure. A brain MRI documented the suspected diagnosis of septic embolism and showed diffuse pathological leptomeningeal enhancement, confirming the diagnosis of meningoencephalitis (Figure 4).
T2-weighted sequence MRI showing an abscess in the right frontal region (A and C) and leptomeningeal enhancement (B and C).
A lumbar MRI was carried out, indicating enhancement of the nerve roots of the cauda equina as well as spondylodiscitis at the L5-S1 level. To establish other sites of septic localization and given the presence of a cough, a thoracoabdominal CT scan showed bilateral pulmonary consolidations due to the same pathogen. A transesophageal echocardiogram was also performed, finding endocardial vegetation on the aortic valve, confirming Austrian syndrome (Figure 5).
Transesophageal echocardiogram showing vegetation on the aortic valve.
The patient also presented several complications. He developed bilateral segmental and subsegmental pulmonary thromboembolism without hemodynamic instability, as well as bilateral superficial thrombosis in arms and legs. These conditions required oral anticoagulation with dabigatran. The patient’s conditions gradually improved, and he was discharged after one month of hospitalization. The antibiotic treatment was switched to oral amoxicillin after three weeks of intravenous ceftriaxone (dosage: 2 g every 12 hours) and continued for a total of six weeks.
The timeline of events for both cases is reported in Figure 6.
Timeline of events for both cases.
Discussion
First described in the 19th century, Austrian syndrome is characterized by the triad of pneumonia, endocarditis, and meningitis, following a pneumococcal infection. S. pneumoniae is a common cause of otitis, sinusitis, and community-acquired pneumonia [4], which usually have a favorable outcome with effective antibiotic treatment. Nevertheless, several factors increase the risk of developing invasive pneumococcal disease, such as advanced age, male sex, harmful alcohol consumption, previous chronic diseases, and prosthetic joints [3]. One of our patients presents all of these risk factors, particularly alcohol use disorder and chronic conditions such as diabetes, obstructive sleep apnea syndrome, hypertension, and atrial fibrillation.
In addition, our patients were not vaccinated against S. pneumoniae, which could have contributed to the aggressive course of the infection. Many studies have highlighted the key role of immunization in preventing invasive pneumococcal disease [2,5]. The CAPITA trial, involving 84,496 adults over 65 years, demonstrated the efficacy of the 13-valent pneumococcal conjugate vaccine (PCV13) in preventing the first episode of invasive pneumococcal disease [6]. Studies on the 23-valent pneumococcal polysaccharide vaccine (PPV23) found similar results, although its effectiveness appears to be age-dependent [7]. Analogous findings were observed with the 20-valent pneumococcal conjugate vaccine [8].
The typical order of appearance of symptoms and localizations of Austrian syndrome is not certain or well-defined. It is proposed that the primary manifestation and portal of entry is pneumonia, usually bilateral. Meningitis is often recognized later, as neurological symptoms may be initially attributed to delirium, and this can influence the neurological prognosis [3,9]. In our patients, neurological alterations such as progressively impaired consciousness, left hemiparesis, and aphasia were the first signs of the disease, leading to early meningitis treatment. Most patients develop severe impairment of consciousness, with a GCS ≤ 8, as well as respiratory failure requiring invasive ventilation [1]. These situations were present in our cases, confirming the aggressive course of Austrian syndrome.
Typically, pneumococcal endocarditis involves left-sided valves (especially the aortic valve), and patients do not develop vasculitic signs. An early surgical approach is essential to prevent cardiogenic shock, as only 17% of cardiac vegetations regress with antibiotic therapy alone [9-12]. In our first case, there was a three-week delay before performing the valve replacement due to the patient’s conditions. In the second case, cardiac surgery was not performed due to the absence of valvulopathy; nonetheless, the prognosis was not affected.
Septic arthritis in Austrian syndrome is uncommon but can be a complication of infective endocarditis, with knee involvement being the most frequent [13]. In our first patient, both hips and the left knee were affected, while the second one developed spondylodiscitis, underscoring the severity of both cases.
In the matter of antibiotic treatment, even though the choice depends on the sensitivity results, a third-generation cephalosporin is frequently used, after an initial period of empirical broad-spectrum antibiotic therapy [1,14,15]. We adopted the same pathway, ending with ceftriaxone and finally amoxicillin.
Vaccination plays a fundamental role in preventing invasive pneumococcal infections. Healthcare strategies must be implemented at local and global levels to identify at-risk individuals and promote vaccination in these sub-groups.
Conclusions
Several valuable key points can be highlighted from our case. Firstly, it is essential to suspect Austrian syndrome in patients with a pneumococcal infection who also present other risk factors. Secondly, there is a high chance of rapid dissemination, even to foci apart from the three typical localizations, which must be promptly recognized. Thirdly, early diagnosis allows for a more aggressive approach in the context of an extremely serious illness. Therefore, rapid, combined medical and surgical treatment is crucial to offer the patient a better chance of recovery. Finally, it is mandatory to strengthen the role of immunization in preventing the development of Austrian syndrome and, more generally, invasive pneumococcal disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Austrian syndrome: report of one case and a systematic review of case reports - new insights Clin Med (Lond) Madu A Alex-Okoro T Okoduwa A Cotton J 1002052420243864913810.1016/j.clinme.2024.100205 PMC 11109293 · doi ↗ · pubmed ↗
- 2Systematic review and meta-analysis of the efficacy and effectiveness of Pneumococcal vaccines in adults Pathogens Farrar JL Childs L Ouattara M Akhter F Britton A Pilishvili T Kobayashi M 12202310.3390/pathogens 12050732 PMC 1022219737242402 · doi ↗ · pubmed ↗
- 3Austrian syndrome: resurgence of an old and deadly triad J Intensive Med Rivera K Viles D Zielonka M Izurieta C Martínez TR Menéndez D 261264420243868179110.1016/j.jointm.2023.06.006PMC 11043638 · doi ↗ · pubmed ↗
- 4Pneumococcus beyond an Austrian syndrome - a case report ID Cases Guerreiro G Monteiro AP Coelho L Póvoa P 028202210.1016/j.idcr.2022.e 01486 PMC 898075435392600 · doi ↗ · pubmed ↗
- 5Vaccine effectiveness of the pneumococcal polysaccharide and conjugated vaccines in elderly and high-risk populations in preventing invasive pneumococcal disease: a systematic search and meta-analysis Eur Clin Respir J Sikjær MG Pedersen AA Wik MS Stensholt SS Hilberg O Løkke A 21683541020233669875010.1080/20018525.2023.2168354 PMC 9870017 · doi ↗ · pubmed ↗
- 6Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults N Engl J Med Bonten MJ Huijts SM Bolkenbaas M 1114112537220152578596910.1056/NEJ Moa 1408544 · doi ↗ · pubmed ↗
- 7A systematic review of studies published between 2016 and 2019 on the effectiveness and efficacy of pneumococcal vaccination on pneumonia and invasive pneumococcal disease in an elderly population Pathogens Berild JD Winje BA Vestrheim DF Slotved HC Valentiner-Branth P Roth A Storsäter J 9202010.3390/pathogens 9040259 PMC 723810832260132 · doi ↗ · pubmed ↗
- 8Case-fatality rate of invasive pneumococcal disease caused by various serotypes-an analysis of nationwide surveillance data from Israel, 2009-2018 Clin Microbiol Infect Wieder-Finesod A Yahav D Rubin C 2262323120253955134310.1016/j.cmi.2024.11.018 · doi ↗ · pubmed ↗