A case of esophagogastric junction obstruction due to octopus ingestion
Junya Shimamoto, Hironori Nakahira

TL;DR
A person experienced a blockage at the esophagogastric junction caused by eating an octopus, as seen in an endoscopic image.
Contribution
Reports a rare clinical case of esophagogastric junction obstruction due to octopus ingestion.
Findings
An endoscopic image showed an octopus mass obstructing the esophagogastric junction.
The case highlights unusual causes of gastrointestinal obstructions.
Abstract
Endoscopic image of the stomach. A mass of octopus is obstructing the entrance to the esophagogastric junction.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
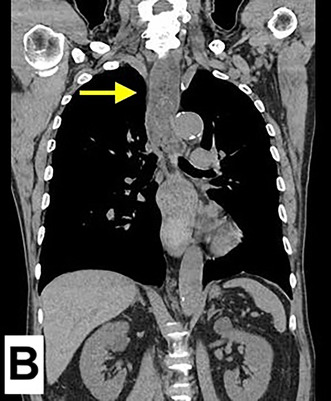 Figure 1
Figure 1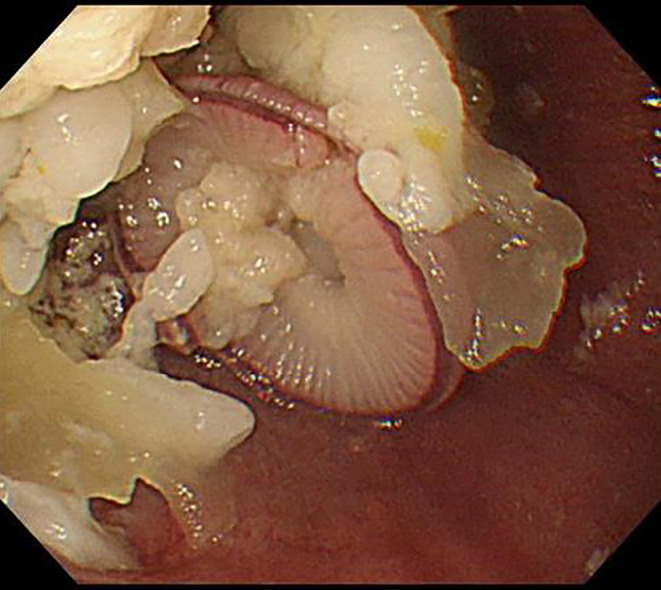 Figure 2
Figure 2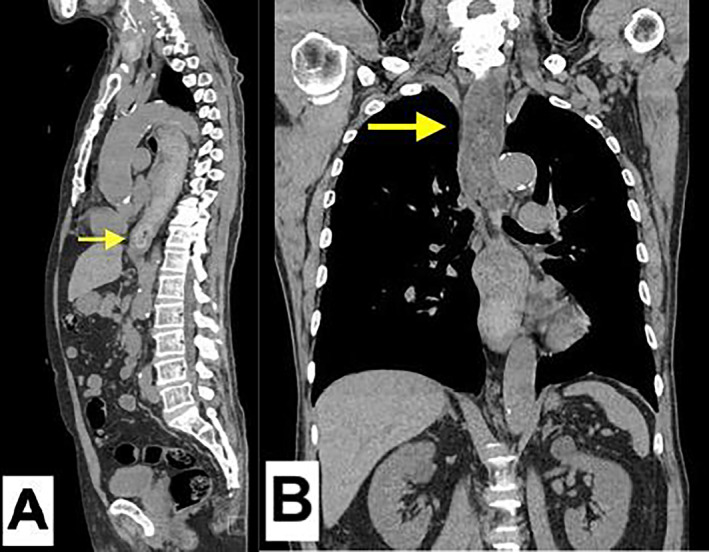 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Airway Management and Intubation Techniques · Restraint-Related Deaths
A 77‐year‐old man presented to the emergency department with chest constriction and persistent vomiting after consuming chopped octopus. A non‐contrast CT scan revealed esophageal dilation with a hyperdense mass obstructing the esophagogastric junction (Figure 1A) and food residues extending into the cervical esophagus (Figure 1B), suggesting significant obstruction and increasing the risk of aspiration. To reduce this risk and improve visibility during endoscopy, a nasogastric tube was inserted approximately 30 cm through the nasal passage, and approximately 50 mL of yellowish, muddy food residues were aspirated. Subsequent esophagogastroduodenoscopy identified an octopus lodged in the distal esophagus (Figure 2). Attempts to remove the octopus using forceps or a retrieval basket were unsuccessful due to its slippery texture, which caused it to disintegrate. Consequently, the push technique1 was employed, successfully advancing the octopus into the stomach and confirming its passage through the esophagogastric junction. Post‐procedural evaluation confirmed that both the stomach and esophagus were intact.
This clinical image report emphasizes two key points. First, it highlights the importance of imaging in the management of patients with gastrointestinal obstruction symptoms. Clinicians must recognize that esophageal obstructions pose a particularly high risk of asphyxiation due to their proximity to the airway, making thorough evaluation and careful preparation essential. While fatalities due to aspiration have been reported even in cases of distal gastrointestinal obstruction under general anesthesia,2 esophageal obstructions require even greater caution. This case underscores the dangers of attempting upper endoscopy without adequate precautions and demonstrates the necessity of assessing aspiration risks beforehand.
Second, this report focuses on the rarity of esophageal obstruction caused by octopus ingestion. Such cases are exceedingly rare, and reports featuring detailed imaging are even less common. Unlike previous reports, which primarily focused on removal techniques, this case emphasizes the diagnostic and procedural value of pre‐endoscopic CT and endoscopic imaging. By placing greater emphasis on imaging, this report offers valuable insights into the safe and effective management of such unique and challenging cases.
AUTHOR CONTRIBUTIONS
JS and HN conducted the endoscopic removal of Octopus. JS wrote the first draft and managed the submission process, and HN checked the draft.
FUNDING INFORMATION
None.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
PATIENT CONSENT
Written informed consent for publication and confidentiality was obtained from the patient.
ETHICS STATEMENT
We confirm that written informed consent was obtained from the patient for publication of the clinical images and accompanying text. The patient was informed that the images and text would be published in a journal accessible to the public, and anonymity was ensured by omitting identifiable information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ASGE Standards of Practice Committee , Ikenberry SO , Jue TL , Anderson MA , Appalaneni V , Banerjee S , et al. Management of ingested foreign bodies and food impactions. Gastrointest Endosc. 2011;73(6):1085–1091. 10.1016/j.gie.2010.11.010 21628009 · doi ↗ · pubmed ↗
- 2Warner MA , Meyerhoff KL , Warner ME , Posner KL , Stephens L , Domino KB . Pulmonary aspiration of gastric contents: a closed claims analysis. Anesthesiology. 2021;135:284–291. 10.1097/ALN.0000000000003831 34019629 · doi ↗ · pubmed ↗