Quantifying the burden of hereditary hemorrhagic telangiectasia on quality of life and psychological health: a cross-sectional study
Anna J. Gong, Marisabel Linares Bolsegui, Emerson E. Lee, Matthew R. Tan, Yong Zeng, Jianqiao Ma, Prateek C. Gowda, Tushar Garg, Clifford R. Weiss

TL;DR
This study finds that hereditary hemorrhagic telangiectasia significantly impacts patients' quality of life, causing depression, anxiety, and fatigue, and highlights the need for better support and interventions.
Contribution
The study quantifies the psychological and quality of life burden of HHT using standardized tools in a large international cohort.
Findings
Severe nosebleeds in HHT patients correlate with higher depression, anxiety, and fatigue scores.
Over half of participants reported significant effects on physical, emotional, and social functioning.
Liver failure and seizures are linked to increased psychological distress and fatigue.
Abstract
Despite the considerable burden that hereditary hemorrhagic telangiectasia (HHT) imposes, few studies have investigated its effect on health-related quality of life (HRQoL). We aimed to assess the impact of HHT on psychosocial QoL and identify demographic and clinical factors associated with lower QoL. We conducted an international, cross-sectional study of 1042 adults with HHT within the Cure HHT network, between 2022 and 2023. We used an online survey that included 5 standardized instruments to evaluate patients’ perceptions of the impact of HHT on their QoL: Epistaxis Severity Score (ESS); Nasal Outcome Score for Epistaxis in Hereditary Hemorrhagic Telangiectasia (NOSE-HHT); Patient-Reported Outcomes Measurement Information System (PROMIS) Fatigue – Short Form 8a – Fatigue interfere scale (PROMIS-Fatigue 8a); Hospital Anxiety and Depression Scale (HADS-A and HADS-D); and Short Form…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
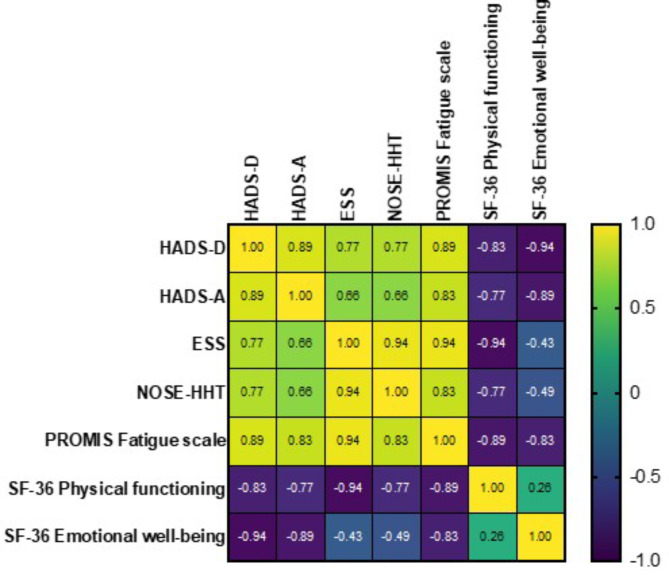 Figure 1
Figure 1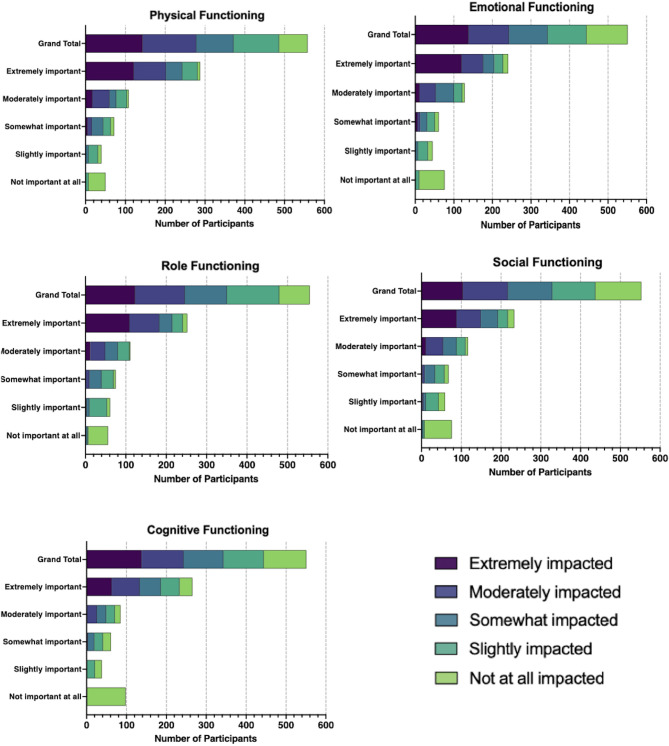 Figure 2
Figure 2- —CureHHT Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Anomalies and Treatments · Tracheal and airway disorders · Vascular Malformations and Hemangiomas
Background
Hereditary hemorrhagic telangiectasia (HHT) is an autosomal dominant multisystem vascular disorder, characterized by the presence of arteriovenous malformations (AVMs) and telangiectasias, especially affecting the skin, nose, lungs, liver, gastrointestinal tract, and central nervous system [1]. The clinical spectrum of this condition is broad, encompassing symptoms ranging from mild to severe epistaxis that frequently result in significant anemia requiring ongoing blood transfusions [1–3]. Gastrointestinal (GI) tract involvement is common. GI AVMs affect up to 80% of patients, with about 30% experiencing bleeding, a major contributor to the anemia seen in nearly half of these patients [1, 2]. 70% of the HHT population experiences liver AVMs, leading to complications such as high-output heart failure, portal hypertension, biliary disease, and neurologic dysfunction [1, 4]. Furthermore, lung AVMs, which are found in up to 40% of individuals, may cause symptoms like dyspnea, pulmonary hypertension, hemorrhage, septic emboli, and stroke. Additionally, cerebral AVMs affect 10–15% of patients, heightening the likelihood of neurologic complications including migraines, seizures, and brain abscesses [5]. This variability in clinical presentation not only complicates diagnosis and management, but also considerably affects the quality of life (QoL) of individuals with HHT [6].
Health-related QoL (HRQoL) is an essential indicator to assess the broader impact of chronic conditions like HHT, beyond the immediate physical symptoms, to quantify the influence of a medical condition, and to evaluate the effectiveness of therapeutic interventions. It encompasses the patient’s perception of their position in life, in the context of culture, value systems, goals, expectations, standards, and concerns [7–9]. Hence, improvements in HRQoL are recognized as a primary outcome and a critical determinant of therapeutic interventions [10]. Despite the known extensive burden of HHT, research into its psychosocial outcomes remains sparse. Studies have explored the prevalence of anxiety and depression among individuals with HHT [11–14]; however, a deep understanding of how HHT-specific manifestations affect psychosocial aspects of HRQoL requires further exploration.
Furthermore, while the physical effects of HHT, such as epistaxis and AVM-related complications, are well documented, their correlation with HRQoL, including the psychosocial dimension, and different domains of functioning have not been thoroughly investigated. The complexity of HHT symptoms and the way they are managed can profoundly affect individuals’ mental health, social interactions, ability to function, and overall QoL, suggesting a substantial but underexplored area of influence on HRQoL.
This internet-based cross-sectional study aimed to investigate the impact of HHT on HRQoL in a diverse population across North America, South America, Europe, Asia, Australia, and South Africa by exploring the symptomatic burden of HHT and identifying demographic variables that could affect HRQoL. The findings are expected to inform clinical practice and future research, with the ultimate goal of improving quality of life for individuals with HHT.
Methods
Study design
We conducted a cross-sectional survey study funded by the Cure Hereditary Hemorrhagic Telangiectasia (Cure HHT) Foundation in North America, South America, Europe, Asia, Australia, and South Africa to investigate the effects of HHT on psychosocial QoL and explore demographic and clinical factors associated with lower HRQoL.
Study population
After institutional review board approval, patients were recruited from March 2022 through May 2022 through the Cure HHT network, an international patient advocacy group. An online survey link was sent via (1) the Cure HHT patient email list, (2) recruitment during a Cure HHT patient conference, or (3) the Cure HHT website. The eligibility criteria were age of 18 years or older; a definitive diagnosis of HHT, requiring at least 3 of the 4 Curaçao Criteria or positive genetic testing for any of the known HHT mutations (ENGL, ALK-1, SMAD4, HHT3/4) [14, 15], and the ability to understand and participate in the survey. All participants provided written informed consent and all responses were anonymized.
Survey description
Participants responded to a survey battery that included demographic information, clinical history, and questions regarding their perception of the influence of their illness experience on their QoL, the presence of different HHT-related manifestations, and 5 standardized surveys: Short Form-36 (SF-36), Hospital Anxiety Depression Scale (HADS), Epistaxis Severity Score (ESS), Nasal Outcome Score for Epistaxis in Hereditary Hemorrhagic Telangiectasia (NOSE-HHT), and Patient-Reported Outcomes Measurement Information System (PROMIS) Fatigue - Short Form 8a - Fatigue interfere scale (PROMIS-Fatigue 8a) [16].
HHT-related conditions (anemia, heart failure, pulmonary hypertension, and liver failure) were captured using dichotomous (“Yes”/“No”) responses, and their extent was categorized from zero to more than four conditions. Participants were asked about their motivation for improving these diagnoses, using a 5-point Likert scale ranging from “not important at all” to “extremely important” to improve. Additionally, participants rated how various HHT-related manifestations influenced their HRQoL using Likert scales, initially indicating the extent to which they desired improvement in different HHT-related symptoms (epistaxis, shortness of breath, exercise intolerance, fatigue, hemoptysis, hematemesis, etc.). Responses were categorized as desire for improvement, no interest in treatment, or not applicable because of the absence of symptoms. Thereafter, the impact of different HHT-related manifestations on 5 functional domains (physical, cognitive, emotional, social, and role functioning) was evaluated using a 5-point adjective-rating scale ranging from “not impacted at all” to “extremely impacted.” Afterward, participants rated the importance of improving the aforementioned domains of functioning using a 5-point adjective rating scale ranging from “not important at all” to “extremely important” to improve.
Description of the patient-reported outcome measure (PROM)s
The Short Form-36 (SF-36) is a standardized instrument that evaluates Health-Related Quality of Life through eight QoL domains: physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH) [17]. In six of the eight domains, patients are asked to rate their responses on 3- to 6-point scales. The SF-36 assesses two distinct magnitudes: the Physical Component Summary (PCS), which represents the physical dimension, and the Mental Component Summary (MCS), which represents the mental dimension. Each domain contributes in different proportions to the scores of both PCS and MCS. Furthermore, the precise calculation of the PCS and MCS is dependent on specific algorithms that are coded, summed, and transformed onto a scale from 0 (worst health) to 100 (best health) [18].
The Epistaxis Severity Score (ESS), the first standardized severity scoring system in HHT (2010), is a partially validated survey that evaluates individual disease severity and treatment efficacy for HHT-related epistaxis [19, 20]. It assesses six independent predictors of self-described epistaxis severity: frequency, duration, severity, anemia, blood transfusions, and the need for medical attention. After applying standardized coefficients to the responses, the sum yields a raw ESS score, which is then normalized to a 0–10 scale from no epistaxis to most severe epistaxis, with a minimal clinically important difference (MCID) of 0.71 [20, 21].
The Nasal Outcome Score for Epistaxis in Hereditary Hemorrhagic Telangiectasia (NOSE-HHT) is a 29-item HHT symptom-specific survey (2020) that evaluates QOL of individuals with HHT. It assesses the effect of epistaxis severity with sensitivity to change on specific psychosocial metrics, such as physical, functional, and emotional aspects (MCID: 0.46). The result is calculated by dividing the sum of each item response by the total number of questions, obtaining a discrete score that ranges continuously from 0 to 4 [21].
The Patient-Reported Outcomes Measurement Information System (PROMIS) Fatigue - Short Form 8a - Fatigue interfere scale (PROMIS-Fatigue 8a) instrument is an assessment developed by the National Institutes of Health (NIH) to measure symptoms and quality-of-life indicators related to different chronic conditions such as multiple sclerosis and rheumatoid arthritis. It utilizes a T-score system normalized to a mean of 50 and a standard deviation (SD) of 10 based on the US general population, where higher scores indicate increased fatigue [8, 22–24].
Lastly, the Hospital Anxiety Depression Scale (HADS) is a self-rated dual 14-item scale on a 4-point scoring system (from 0 to 3) that measures symptoms of anxiety (HADS-A) and depression subscore (HADS-D) during the previous 7 days. For each component the total maximum score is 21, and higher scores correspond with greater severity of the conditions. A score of 11 or above on either subscale suggests a diagnosis of anxiety or depression [25, 26].
Statistical analysis
Pearson’s and Spearman’s rho correlations evaluated the strength of association between the severity of epistaxis (as defined by ESS and NOSE-HHT scores) and variables such as anxiety, depression, fatigue, physical and mental functioning (assessed by HADS, PROMIS-Fatigue 8a, and SF-36). Additionally, we explored the relationship between demographic variables and the burden of HHT-related health conditions.
Multivariable linear regression was employed to determine the independent effect of epistaxis severity and different demographic factors (age, sex, race, and ethnicity) on HRQoL, while adjusting for demographic covariates and the presence of known HHT-related genetic mutations.
The association between the perceived impact of HHT and the importance attributed by participants to improving five domains of functioning (physical, cognitive, emotional, social, and role) was characterized using Likert scales and Spearman correlation analysis. Tukey’s honest significant difference (Tukey’s HSD) test was applied to compare HADS-A and HADS-D scores, as well as NOSE-HHT and ESS. The non-parametric Kruskal-Wallis test assessed mean differences in demographic and clinical manifestations related to HHT and all included PROs.
Statistical analyses were conducted using Stata Statistical Software: Release 17 (Stata Corp LLC; College Station, TX) and R software [27]. Results were reported with effect size measures to delineate the magnitude of the difference or the strength of the association between the compared groups, with a significance threshold set at P < 0.05. and 95% confidence interval (CI) defining the accuracy of the estimate. GraphPad Prism version 9.5.1 for Windows (GraphPad Software, Boston, MA) [28] was used to create figures.
Results
Patient-reported illness characteristics
Of 1042 patients initially recruited, 565 (54.2%) completed the survey. The mean (standard deviation [SD]) age was 56.1 (13.6) years. Most participants were female (72.6% [410/565]), White (93.6% [529/565]), non-Hispanic (91.3% [516/565]), and from North America (57.5% [325/565]), and a majority reported having a known HHT-related genetic mutation (66.5% [376/565]) (Table 1). Anxiety was present in 22% of the participants (162/565), and depression and severe fatigue in 10% (58/565) respectively. The most affected component of the SF-36 was energy (mean score 35, SD 20.7), followed by the physical component summary (mean 40.8, SD 41.8) (Table 2). More than half the participants (51.6% [292/565]) reported having 3 or more HHT-related conditions. The mean age demonstrated a positive trend with the number of HHT-related health conditions, indicating that an increased burden of disease could be correlated with advancing age. Specifically, the mean age rose incrementally from 52.1 years in participants with no conditions to 58 years in those with four or more conditions. Notably 80.9% (72/89) of those with more than four conditions were female, pointing to a potential sex-related predisposition to developing a greater number of HHT-related health complications (Table 3).
Table 1. Demographic description of the study populationPatient populationTotal N 565Age,** mean (SD)**56.1 (13.6) Sex
N (%) Male155 (27.4)Female410 (72.6) Race White529 (93.6)Asian11 (1.9)Black or African American9 (1.6)American Indian or Alaska Native5 (0.9)Native Hawaiian or Other Pacific Island1 (0.2)Other10(1.8) Ethnicity Hispanic, Latino, or of Spanish origin44 (7.8)Non- Hispanic, Latino, or of Spanish origin516 (91.3)Missing5 (0.9) Geographic region North America325 (57.5)South America8 (1.4)Europe51 (9.0)Asia7 (1.2)Oceania17 (3.0)Africa1(0.2)Missing163 (28.8) Patients with known genetic mutations associated with HHT 376 (66.5)
Table 2. Description of the patient reported outcome measurements (PROMs) describing the severity of epistaxis (ESS and NOSE-HHT), anxiety (HADS-A), depression (HADS-D), fatigue (PROMIS-Fatigue-8a), and physical and mental functioning (SF-36) of the study populationPatient populationTotal (%)ESS,** mean (SD)5 (2.1)Mild (1–4)188 (33)Moderate (4–7)266 (47)Severe (7–10)111 (20)NOSE-HHT, mean (SD)1.7 (0.8)Mild (0–1)126 (22)Moderate (1.01-2)239 (42)Severe (> 2)200 (36)HADS-D, mean (SD)6.3 (4)Normal (0–7)369 (65)Borderline abnormal (8–10)107 (19)Abnormal (11–21)89 (16)HADS-A, mean (SD)8 (4.3)Normal (0–7)275 (49)Borderline abnormal (8–10)128 (22)Abnormal (11–21)162(22)PROMIS-Fatigue 8a, mean (SD)**60 (8.5)Normal limits (20–54)159 (28)Mild (55–60)106 (19)Moderate (61–70)242 (43)Severe (71–80)58 (10) SF-36
mean (SD) General Health44.3 (22)Physical Function60.5 (29)Physical Limitations40.8 (41.8)Emotional Limitations50.6 (43.7)Energy35 (20.7)Emotional62.3 (20)Social58 (31)Pain64 (27)AVM, arteriovenous malformation; CI, confidence interval; ESS, Epistaxis Severity Score; GI, gastrointestinal; HADS-A, Hospital Anxiety and Depression Scale (Anxiety); HADS-D: Hospital Anxiety and Depression Scale (Depression); NOSE-HHT, Nasal Outcome Score for Epistaxis in Hereditary Hemorrhagic Telangiectasia; PROMIS-Fatigue 8a, Patient-Reported Outcomes Measurement Information System Short Form 8a - Fatigue interfere scale, SD, standard deviation; SE, standard error; SF-36, Short Form-36
Table 3. Relationship between the demographic variables and the burden of HHT-related health conditionsFactorLevelZero conditionsOne conditionTwo conditionsThree conditionsFour conditionsMore than four conditionsMissingTotal (N = 565)47 (8.3%)65 (11.5%)81 (14.3%)114 (20.1%)89 (15.7%)89 (15.7%)80 (14.1%)Age (years), mean (SD)52.1 (14.3)56 (14.4)56 (15)54.7 (14.3)56.7 (12.2)57.6 (11.2)58. (12.8)SexFemale33 (70.2%)44 (67.7%)58 (71.6%)86 (75.4%)66 (74.2%)72 (80.9%)51 (63.7%)Male14 (29.8%)21 (32.3%)23 (28.4%)28 (24.6%)23 (25.8%)17 (19.1%)29 (36.2%)Hispanic, Latino, or of Spanish origin2 (4.3%)7 (10.9%)9 (11.1%)6 (5.3%)3 (3.4%)4 (4.5%)13 (16.9%)RaceWhite43 (91.5%)63 (96.9%)78 (96.3%)111 (97.4%)85 (95.5%)80 (89.9%)69 (86.2%)Asian3 (6.4%)2 (3.1%)1 (1.2%)1 (0.9%)01 (1.1%)3 (3.8%)Black001 (1.2%)01 (1.1%)6 (6.7%)1 (1.2%)Native Hawaiian or Pacific Island00001 (1.1%)00American Indian or Alaska Native0001 (0.9%)1 (1.1%)1 (1.1%)2 (2.5%)Missing1 (2.1%)01 (1.2%)1 (0.9%)1 (1.1%)1 (1.1%)5 (6.2%)Geographic LocationNorth America30 (62.9%)31 (47.7%)46 (56.8%)71 (62.3%)50 (56.2%)48 (53.9%)49 (61.3%)South America01 (1.5%)02(1.8%)01 (1.1%)3 (3.7%)Europe2 (4.2%)6 (9.2%)7 (8.6%)8 (7%)8 (8.9%)6 (6.7%)5 (6.2%)Oceania1 (2.1%)1 (1.5%)1 (1.2%)2 (1.8%)2 (2.2%)7 (7.9%)2 (3.7%)Asia1 (2.1%)1 (1.2%)01 (1.1%)01 (1.2%)South Africa001 (1.2%)0000Missing13 (27.7%)26 (40.0%)26 (32.1%)24 (21.1%)28 (31.5%)27 (30.3%)19 (23.8%)Genetic mutation associated with HHT?33 (70.2%)41 (63.1%)56 (69.1%)77 (67.5%)51 (57.3%)64 (72.7%)54 (70.1%)Type of mutationENG OR HHT16 (12.8%)11 (16.9%)19 (23.5%)28 (24.6%)12 (13.5%)16 (18.0%)14 (17.5%)ALK-1 OR HHT2 OR ACVRL14 (29.8%)11 (16.9%)20 (24.7%)17 (14.9%)17 (19.1%)12 (13.5%)11 (13.8%)SMAD402 (3.1%)3 (3.7%)2 (1.8%)4 (4.5%)6 (6.7%)4 (5.0%)Another mutation1 (2.1%)01 (1.2%)2 (1.8%)1 (1.1%)1 (1.1%)1 (1.2%)Unknown12 (25.5%)15 (23.1%)13 (16.0%)22 (19.3%)14 (15.7%)27 (30.3%)20 (25.0%)Not tested01 (1.5%)06 (5.3%)3 (3.4%)2 (2.2%)3 (3.8%)Missing14 (29.8%)25 (38.5%)25 (30.9%)37 (32.5%)38 (42.7%)25 (28.1%)27 (33.8%)HHT, Hereditary hemorrhagic telangiectasia; SD, standard deviation
Correlates for anxiety, depression, and fatigue in patients with HHT
Spearman’s correlation analyses revealed a positive correlation between the severity of epistaxis and measures of anxiety, depression, and fatigue (Fig. 1). The median scores for each PRO increased in proportion to the intensity of epistaxis (severe epistaxis ESS > 7), evidenced by higher HADS-A (10; 95% confidence interval [CI] 7–13), HADS-D (8; 95% CI 5–11), and PROMIS-8a Fatigue scale (65.3; 95% CI 61.3–69.8) scores, respectively. Physical and mental abilities declined as the severity of the epistaxis increased. The physical component summary (PCS) of the SF-36 was substantially more affected than the mental component summary (MCS) (45 versus 56 in participants who reported severe epistaxis) (Table 4).
Fig. 1. Spearman correlation analysis
Table 4. Spearman Rho correlation between epistaxis severity (defined by ESS and NOSE-HHT scores) and anxiety, depression (HADS-A, and HADS-D), fatigue (PROMIS-Fatigue 8a), physical and mental functioning (SF-36)ESS categoriesHADS-AHADS-DPROMIS-Fatigue 8aSF-36 physical component summary (PCS)SF-36 mental component summary (MCS) Mild 6 (4–10)4 (2–7)56.6 (50.4–63.3)84.2 (52.5–95)72 (48–84) Moderate 7 (4–11)6 (4–9)61.3 (54.6–65.3)65 (40–85)64 (48–80) Severe 10 (7–13)8 (5–11)65.3 (61.3–69.8)45 (20–70 )56 (40–68 ) Spearman rho (95% CI) 0.2 (0.1–0.3)0.3 (0.2–0.4)0.3 (0.2–0.4)−0.3 (− 0.4 to − 0.3)−0.2 (− 0.3 to − 0.1) NOSE-HHT
Mild 6 (3–9)3 (2–6)53.6 (49.2–60.4)85 (65–95)76 (60–88) Moderate 6 (4–10)5 (3–7)58.5 (52.5–63.3)75 (55–90)68 (52–80) Severe 10 (7–13)9 (6–11 )65.3 (61.3–69.8)40 (20-62.5)52 (40–64) Spearman rho (95% CI) 0.3 (0.2–0.4)0.5 (0.4–0.6)0.5 (0.4–0.6)−0.5 (− 0.5 to − 0.4)−0.4 (− 0.4 to − 0.3)
The multivariable linear regression analysis revealed that in patients with severe epistaxis, for each ESS unit increase, we observed an average increase of 2.4 points in HADS-A, 3.3 points in HADS-D, and 8 points in the PROMIS-Fatigue 8a, after adjusting for other factors. In addition, liver failure and shortness of breath were strongly positively correlated with higher HADS-A, HADS-D, and PROMIS-Fatigue 8a scores. Conversely, White race was negatively correlated with the NOSE-HHT score (− 0.28;−0.55,−0.01) and older participants exhibited lower HADS and PROMIS-Fatigue 8a scores. These findings suggest that individuals with severe epistaxis and HHT-related comorbid diagnoses such as liver failure, seizures, and shortness of breath are more likely to experience greater anxiety, depression, and fatigue. Patients with heart failure showed the most substantial reduction in physical ability. Liver failure was the second most important covariate for a lower PCS score (ß = −30; −46.6 to − 13.2). Female and elderly participants demonstrated a more pronounced negative impact on their physical ability, with lower PCS scores, while White race was associated with a higher PCS score. Age inversely correlated with all quality of life measures except the MCS, where it showed a slight positive association. No significant correlation was observed between race or sex and MCS score (Supplement 2:eTable 1). Moreover, ANOVA with Tukey’s post hoc analysis indicated that individuals categorized as abnormal HADS-A (mean [SD] 2.1 [0.8]) and HADS-D (2.4 [0.7]) had higher mean NOSE-HHT and ESS than those in the normal category (1.3 [0.7] and 4.6 [2.0], respectively) (Supplement 2:eTable 2).
Correlates for epistaxis severity and other HHT-Related symptoms
The Kruskal-Wallis test revealed a significant difference between the ESS categories among participants with prior epistaxis-related treatment (5.2), anemia (5.6), pulmonary hypertension (6.1), shortness of breath (5.5), hemoptysis (5.8), headache (5.4) (all p < 0.001); lung AVMs (4.6), SMAD4 genetic mutation (5.2), heart failure (5.9) (all p = 0.001); and seizures (6.2) (p = 0.004) (Supplement 2: eTable 3).
Patient-reported impact and desire to improve HHT-related manifestations and areas of functioning
The most common symptoms that affected HRQoL and prompted a strong desire for improvement were nosebleeds (92.2%), fatigue (78.9%), shortness of breath (60.9%), exercise intolerance (58.9%), and headaches (49.6%) (Supplement 2:eTable 4). Notably, anemia was rated by 47.4% of the participants as extremely important to improve (Supplement 2:eTable 5).
The perceived impact and importance of improving different HHT manifestations on separate areas of functioning provided noteworthy insights into the wide-ranging consequences of HHT on patients’ daily lives (Fig. 2). Participants reported their physical functioning as the most “extremely impacted” domain (25.3%), followed by role functioning (24.8%), emotional functioning (21.9%), social functioning (18.4%), and cognitive functioning (11.3%). Nearly half of the participants (49.3%) reported either “extremely” or “moderately” impacted physical functioning (Supplement 2:eTable 6). Moreover, the proportion of participants who reported it as “extremely important” to improve their physical, cognitive, and emotional functioning was approximately twice as great as that of participants reporting these domains as “extremely impacted” (Supplement 2:eTable 7). Participants who rated their cognitive (17.9%) and physical (14.1%) domains as “somewhat or slightly impacted” still considered it “extremely important” to improve these areas of functioning. Spearman correlation analysis revealed a significant positive correlation between the 5-point adjective rating scales measuring the level of impact and the level of importance of improving all 5 domains of functioning: emotional functioning (r = 0.64), role functioning (r = 0.64), social functioning (r = 0.62), physical functioning (r = 0.59) (all p < 0.0001), and cognitive functioning (r = 0.63) (p < 0.001).
Fig. 2. Five-point Likert scales of perceived impact and level of importance on HHT-related functional domains
Discussion
Our findings provide insight into how HHT-related manifestations affect the psychosocial health of individuals living with this condition. People with HHT often suffer from more than three HHT-related conditions and confront substantial challenges in their daily lives, resulting in a decline in their HRQoL. Symptoms contributing to this decline included epistaxis, fatigue, shortness of breath, exercise intolerance, and headaches, and these were strongly correlated with anxiety, depression, and fatigue. In addition, anemia emerged as the condition that participants prioritized for improvement. Our analysis reveals a strong correlation between epistaxis severity and lower QOL measurements, emphasizing the profound psychosocial implications of this symptom.
This study underscores the heterogeneous nature of HHT and the need for comprehensive management strategies to address the diverse manifestations of the disease. Our outcomes revealed that women and older participants experienced a more negative effect on their physical well-being. The majority of study subjects identified as White, and they exhibited better physical functioning than the other racial and ethnic groups. In addition, the representation of other ethnicities was considerably lower, which may reflect the demographic composition of the cohort or suggest potential disparities in disease prevalence and health outcomes across different races within the HHT population. Age was negatively correlated with PCS but positively correlated with MCS, suggesting an association between increasing age and improved mental well-being. Despite variations in the perceived impact severity of functional limitations, participants consistently expressed a strong desire for improvement across all domains, suggesting that they recognize the benefit of addressing these specific domains, even if the perceived impact may not be as pronounced as the strong desire for improvement.
The negative outcomes of HHT are comparable to those of other chronic diseases, resulting in lower levels of physical and psychological QoL compared to those without this condition [8, 12, 13, 16, 20]. Various HHT-related conditions have consistently been linked to poorer outcomes and reduced QoL [6, 13, 14, 18, 29, 30]. Different standardized validated instruments, such as the ESS [14, 20], SF-36 [13, 29], PROMIS- Fatigue 8a [31], EuroQol 5-dimension 3-level version [32], social index [12], non-standardized questionnaires [30], and interviews [11], have been used to measure physical, emotional, and social domains in individuals with HHT. However, the influence of this condition on HRQoL is often underestimated, and the understanding of HRQoL may still benefit from further research to explore dimensions not fully addressed by existing instruments [6, 31, 33].
Important associations have been reported between the severity of epistaxis and fatigue levels in individuals with HHT, a condition often complicated by fatigue due to iron deficiency anemia from nosebleeds [34, 35]. Nevertheless, while the relationship between general fatigue and HHT is documented [36, 37], our analysis contributes to the literature by specifically examining how variations in epistaxis severity influence fatigue levels. This aspect has not been distinctly addressed previously, revealing a gap in direct data correlating epistaxis severity with fatigue levels in HHT [1, 2]. Seizures, an uncommon but disturbing type of HHT-related complication, were identified as a significant predictor (p < 0.05) of worse HRQoL, and the established association between epilepsy and depression and lower QoL corroborates our findings [10, 38, 39]. Current research on the consequences of multiple chronic conditions on HRQoL is limited [40]. Despite this, it seems plausible that there is a synergistic effect of different HHT-related manifestations, including epistaxis, liver failure, cerebral AVM, and seizures, on QoL and psychological health.
Moreover, patients with HHT and comorbid liver and gastrointestinal AVMs demonstrated remarkably lower PCS scores than the general population (43.8 vs. 50). Previous studies have indicated that patients with New York Heart Association (NYHA) class III heart failure exhibit SF-36 scores only one-third as high as the non-diseased population in the domains of physical functioning, bodily pain, general health, vitality, and role functioning [41–44]. This study builds upon prior research by specifically examining the significance of heart failure within patients with HHT, reaffirming the connection between heart failure and diminished physical ability.
Our analyses revealed that demographic factors such as age and sex have an effect on the HRQoL of patients with HHT, as seen in other chronic conditions. The phenotype of HHT is age-dependent, and most of the patients exhibit a complete penetrance after the age of 40 (e.g., GI bleeding is rare before age 50 years) [1, 45]. Likewise, advanced age in patients with HHT has been previously associated with increased physical limitations and worse psychosocial quality of life and QoL scores [12–14, 46]. Our findings showed an increased number of HHT-related comorbid diagnoses in elderly participants, but we found better mental and psychological QoL in the same age group when compared to their younger counterparts. Although young people with HHT usually experience less severe symptoms and older patients bear the vast majority of the HHT-related disease burden, QoL might improve as individuals adapt to living with their illness [6, 21, 47]. Older adults with HHT may have developed more mechanisms to cope with their disease because of their experience navigating their diagnosis, possibly decreasing anxiety and fatigue [6]. These findings highlight the significance of age and experience in adapting to the effects of HHT on individuals’ overall QoL.
The pronounced negative consequences on physical functioning in women may reflect broader trends of sex-specific disparities in health outcomes and suggest that female patients with HHT might experience more severe physical manifestations or have different coping mechanisms compared to male patients. Previous studies have indicated that women have more pronounced liver involvement, a higher prevalence of pulmonary AVMs, and a greater requirement for invasive procedures than men [48, 49]. Because of their longer lifespan, women endure a higher prevalence of physical and psychological illnesses and lower QoL than males [49, 50].
Additional evidence has revealed that Asian individuals have a higher incidence of pulmonary AVMs when compared with the other racial and ethnic groups, while Hispanic or Latino individuals may develop more cerebral AVMs [51, 52]. Understanding the association between race and ethnicity and psychosocial health related to HHT will provide valuable information for identifying potential health disparities to develop tailored and equitable interventions.
Limitations
Several limitations should be acknowledged. First, the use of self-reported survey data and reliance on a specific patient advocacy group network may introduce selection and response biases, potentially limiting the generalizability of the findings across different populations. Moreover, the cross-sectional survey design prevents us from establishing causal relationships. We must recognize that the full extent of HHT’s negative effects on patients’ HRQoL may not be entirely understood because of the absence of a dedicated HHT-specific instrument capable of accurately capturing PROs for this condition [31]. Only 2 of the 4 validated QoL instruments specific to HHT (ESS and NOSE-HHT) were included, as neither the QoL-HHT nor the HHT-QoL instrument was published at the time of this study [6, 31].
Conclusions
This study addresses a gap in the literature by examining how HHT-related manifestations affect patients’ psychosocial health and QOL. While severe epistaxis has predominated as one of the most prevalent and debilitating symptoms, it provides only a narrow view of the impact of HHT. Our findings emphasize the multifaceted impact of HHT on patients’ lives and how several HHT-related manifestations might be associated with adverse psychological outcomes and low QoL. Also, various demographic factors such as age, sex, and race have shown notable correlations with reduced physical ability and adverse psychological outcomes. Acknowledging the full scope of HHT’s negative effects is essential for a more nuanced understanding and management of this condition, improving patient care and effective target interventions.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Donald J, Stevenson DA et al. Hereditary Hemorrhagic Telangiectasia. In: Adam MP, Everman DB, Mirzaa GM, Pagon RA, Wallace SE, Bean LJ, editors. Gene Reviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993 [cited 2023 Feb 12]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK 1351/20301525 · pubmed ↗
- 2Locke T, Gollamudi J, Chen P. Hereditary Hemorrhagic Telangiectasia (HHT). Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls Publishing; 2022 [cited 2023 Feb 12]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK 578186/35201714 · pubmed ↗
- 3Bayrak-Toydemir P, Mao R, Lewin S, Mc Donald J. Hereditary hemorrhagic telangiectasia: An overview of diagnosis and management in the molecular era for clinicians. Genet Med [Internet]. 2004 [cited 2023 Jun 9];6:175–91. Available from: https://www.nature.com/articles/gim 20043910.1097/01.gim.0000132689.25644.7c 15266205 · doi ↗ · pubmed ↗
- 4Kotronoulas G, Maguire R, Harrow A, Di Domenico D, Croy S, Kearney N. What is the value of the routine use of patient-reported outcome measures toward improvement of patient outcomes, processes of care, and health service outcomes in cancer care? A systematic review of controlled trials. [cited 2023 Mar 14]; Available from: https://core.ac.uk/reader/158368143?utm_source=linkout 10.1200/JCO.2013.53.594824711559 · doi ↗ · pubmed ↗
- 5Martinent G, Carrot M, Chirac A, Dupuis-Girod S, Fargeton A-E, Blois Da Conceição S et al. Hereditary hemorrhagic telangiectasia and health-related quality of life: a qualitative investigation. Qual Life Res [Internet]. 2020 [cited 2023 May 26];29:1291–9. Available from: 10.1007/s 11136-020-02415-710.1007/s 11136-020-02415-731907872 · doi ↗ · pubmed ↗
- 6Zarrabeitia R, Fariñas-Álvarez C, Santibáñez M, Señaris B, Fontalba A, Botella LM et al. Quality of life in patients with hereditary haemorrhagic telangiectasia (HHT). Health Qual Life Outcomes [Internet]. 2017 [cited 2023 May 24];15:19. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 5259834/10.1186/s 12955-017-0586-z PMC 525983428114930 · doi ↗ · pubmed ↗
- 7Geisthoff UW, Heckmann K, D’Amelio R, Grünewald S, Knöbber D, Falkai P et al. Health-related quality of life in hereditary hemorrhagic telangiectasia. Otolaryngology - Head and Neck Surgery [Internet]. 2007 [cited 2023 May 24];136:726.e 1-726.e 10. Available from: https://www.sciencedirect.com/science/article/pii/S 019459980603606010.1016/j.otohns.2006.12.01917478205 · doi ↗ · pubmed ↗
- 8Merlo CA, Yin LX, Hoag JB, Mitchell SE, Reh DD. The effects of epistaxis on health-related quality of life in patients with hereditary hemorrhagic telangiectasia. International Forum of Allergy & Rhinology [Internet]. 2014 [cited 2023 Feb 17];4:921–5. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/alr.2137410.1002/alr.2137425145809 · doi ↗ · pubmed ↗