Treatment costs of long-term invasive meningococcal disease sequelae: A literature review and Delphi study in Brazil
Noemia Teixeira de Siqueira Filha, Fanny Cortes, Meline Kron, Maira Galdino da Rocha Pitta, Fernando Zanghelini, Bruna de Veras, Tatiane Almeida Menezes, Ana Medina, Lessandra Michelin, Thatiana Pinto

TL;DR
This study estimates the high costs of long-term complications from meningococcal disease in Brazil, highlighting the need for healthcare and social support.
Contribution
The study provides novel cost estimates for IMD sequelae in Brazil using a Delphi survey and microcosting approach.
Findings
Amputations had the highest treatment costs due to hospitalization and therapy.
Caregivers lost significant workdays due to IMD sequelae, especially for multiple limb amputations.
Speech therapy and psychologist sessions were most needed for hearing loss and mental health disorders.
Abstract
•Significant costs varying by sequelae type, care level, and medical procedures.•Delphi survey in Brazil: consensus on high resource use for IMD sequelae, especially in first year.•Highest costs for amputations with hospitalization, medical care, and therapy.•Findings aid in understanding patient & family needs, from healthcare to income loss. Significant costs varying by sequelae type, care level, and medical procedures. Delphi survey in Brazil: consensus on high resource use for IMD sequelae, especially in first year. Highest costs for amputations with hospitalization, medical care, and therapy. Findings aid in understanding patient & family needs, from healthcare to income loss. This study describes and estimates the social and economic impact of Invasive Meningococcal Disease (IMD) sequelae globally and in Brazil. An integrative review was conducted to identify IMD sequelae…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1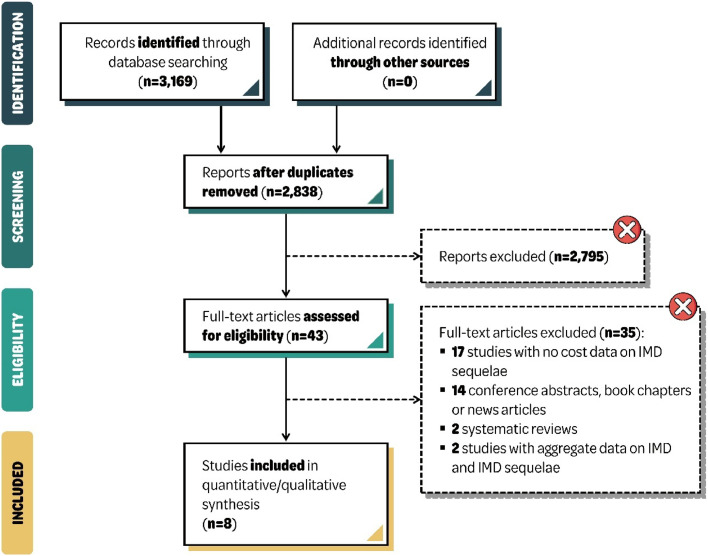 Figure 2
Figure 2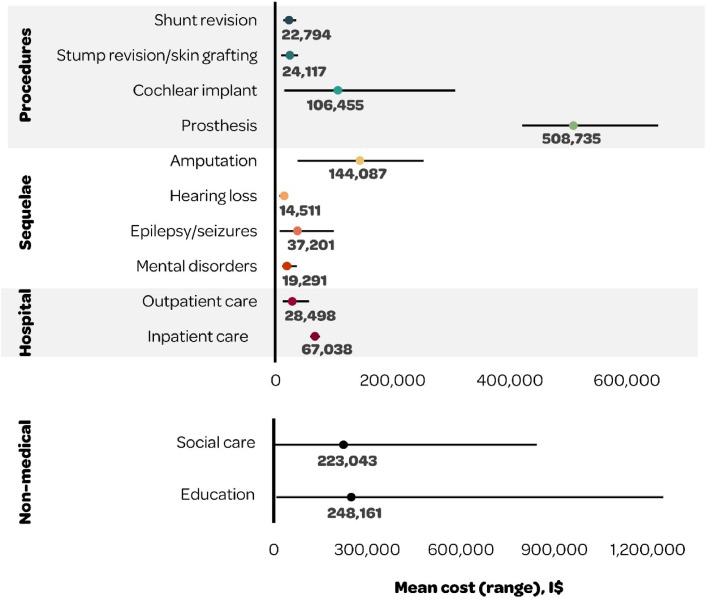 Figure 3
Figure 3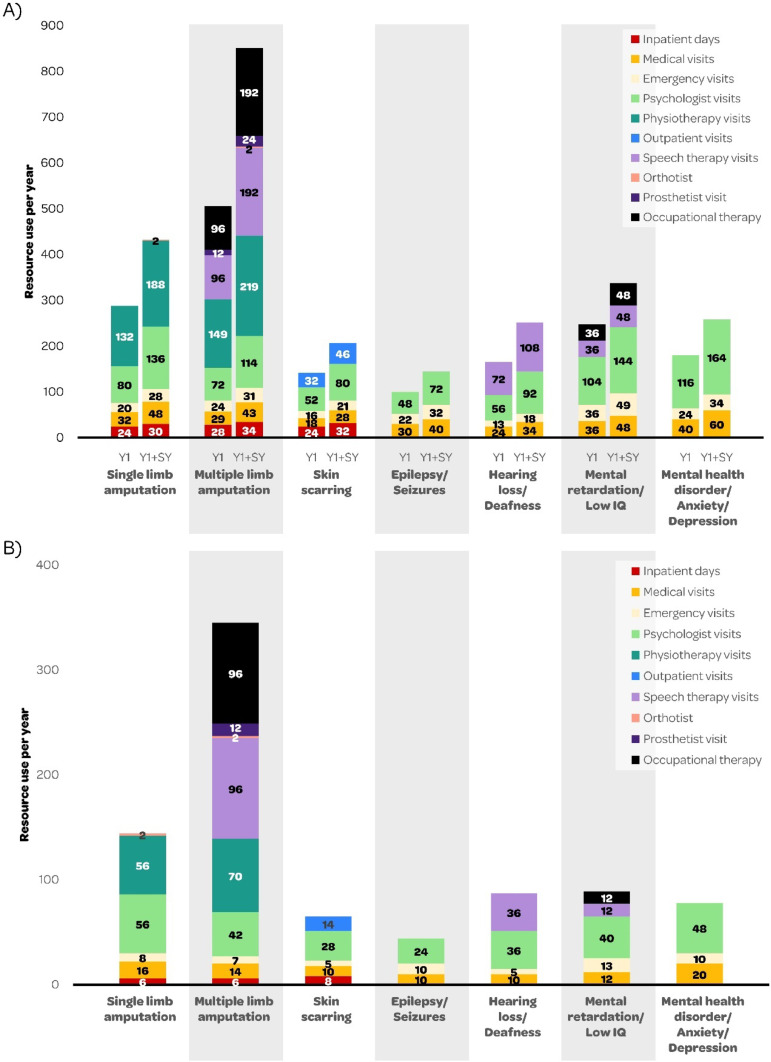 Figure 4
Figure 4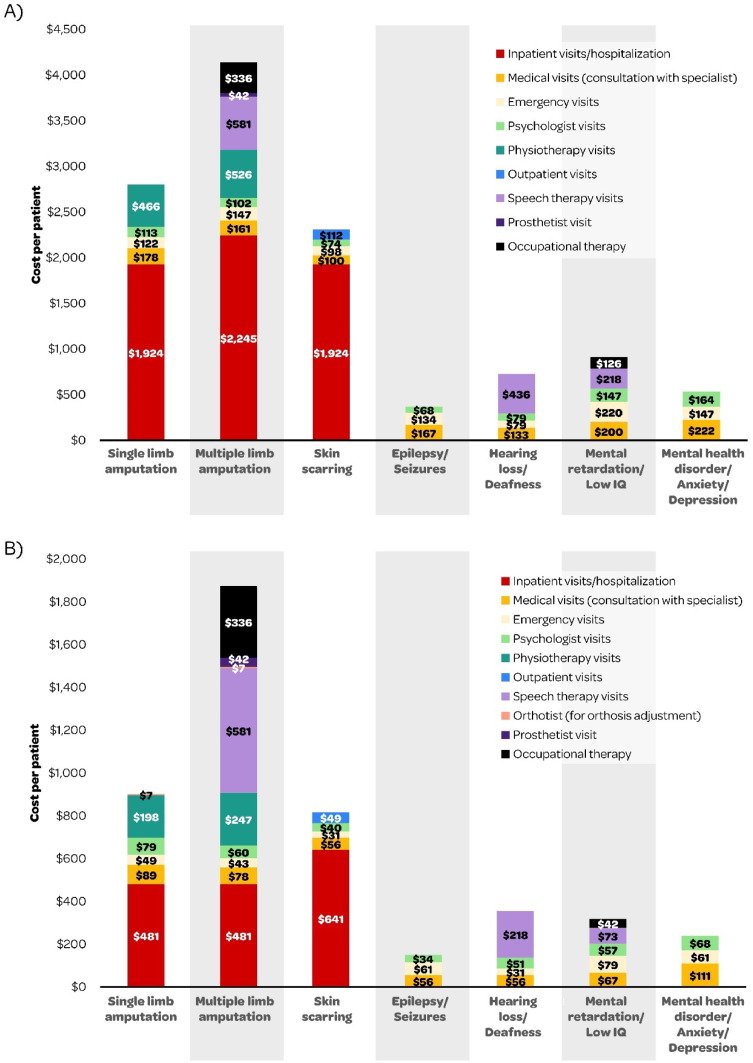 Figure 5
Figure 5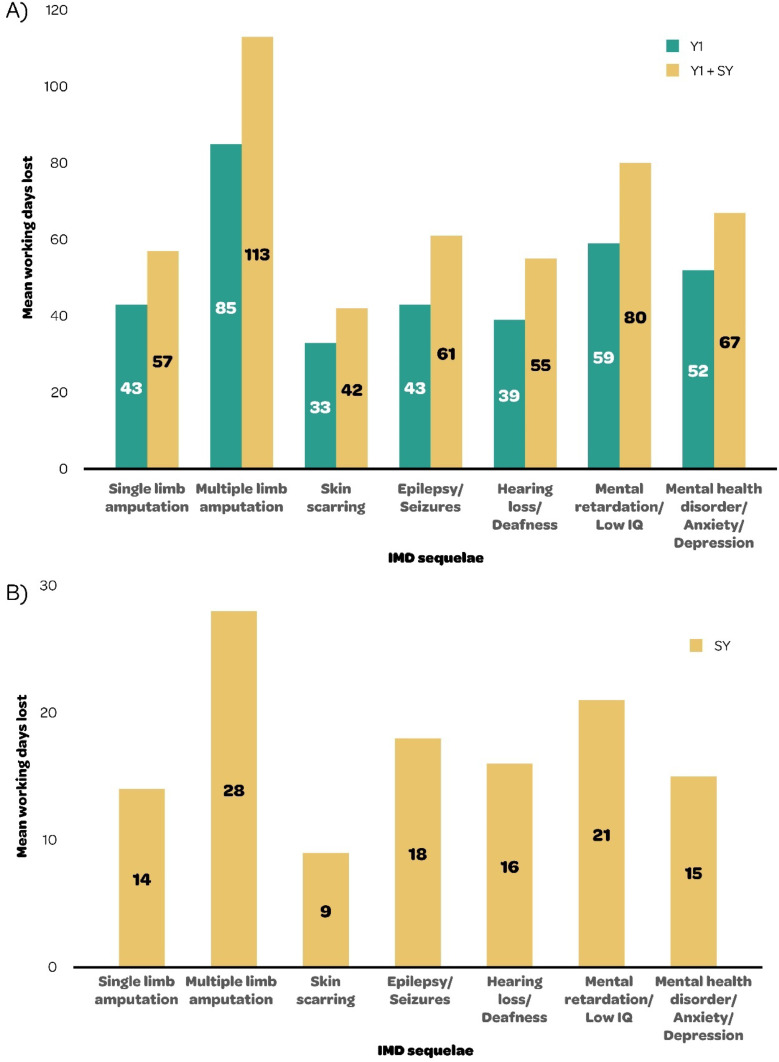 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Cystic Fibrosis Research Advances · Pneumonia and Respiratory Infections
Introduction
Invasive Meningococcal Disease (IMD), caused by the bacterium Neisseria meningitidis, is an uncommon yet severe and life-threatening disease that progresses rapidly and can result in serious and long-term sequelae in survivors. It is the main cause of meningitis and septicemia in children and young adults in Brazil, and is a major public health burden.1
IMD is endemic in Brazil, with periods of hyper-endemicity.1^,^2 Disease incidence has an unpredictable cyclical pattern, varying over time and across regions of Brazil, with the highest rates in infants.3 Of the six serogroups that cause most disease, serogroup B and C are now predominant in Brazil1 and cause most recent outbreaks.4, 5, 6 Case Fatality Rates (CFR) vary annually, as well as by age group and serogroup. In an observational study using Brazilian surveillance data collected over the 2005‒2018 period, estimated CFRs for meningococcal disease in the overall population was approximately 21 % with no notable differences in any particular year or period.7 The CFRs were higher in infants < 1-year, with a mean CFR across 2005–2018 of 23.4 %. The Brazilian Ministry of Health reported a CFR of 24.1 % for serogroup W, 19.2 % for serogroup C, and 17.7 % for serogroup B in 2015.6 In a recent outbreak reported in Brazil, the mortality rate for children < 1-year of age was 23.32/100,000 inhabitants and the CFR in this age group reached 75.0 % (for all serogroups).6 Most reported cases were identified as serogroup B (72.7 %) and other cases were non-serogrouped (27.3 %).6
Studies have estimated that around 20 %–40 % of survivors of the acute phase of IMD will suffer from one or more sequelae.8 A systematic review identified a broad range of 30 different physical and neurological sequelae and 14 psychological and behavioral sequelae resulting from IMD. The most important physical and neurological sequelae, with important quality of life and economic consequences, were renal condition, hearing loss, communication disorders, motor deficits, skin scarring, epilepsy, amputations, mental retardation and blindness. For psychological and behavioral sequelae, the most important were anxiety, depression and attention deficit and hyperactivity disorder.8 Many of these sequelae were still present in long-term follow-up studies,8 highlighting the lifelong burden of disease for IMD survivors and their families and caregivers.9
Although some studies outside Latin America have reported the long-term economic burden associated with IMD, few peer-reviewed studies have estimated the costs associated with IMD in Brazil, and these mainly focused on the healthcare system perspective.4^,^10, 11, 12 Furthermore, the medical costs of long-term sequelae are significant for healthcare systems and can have an important impact on patients’ families, particularly in low- and middle-income countries. In addition to causing productivity and income losses in caregivers who may give up employment to care for a child with long-term disability, patients with sequelae may require special education for learning disabilities and their long-term work prospects may be affected, they may need rehabilitation and long-term care, and social and financial aid.13 Many economic studies do not account for the considerable burden of long-term sequelae on survivors and their families.8
A recent systematic review on the global costs of IMD and sequelae reported around 40 % of IMD patients developed sequelae, and healthcare costs were almost twice as high in patients with sequelae versus without. The review included only studies with primary data collection, thus did not identify non-medical and indirect costs of IMD (e.g., productivity losses) and did not report specific costs of sequelae. In addition, most studies only followed patients until discharge, so long-term rehabilitation and care costs were not identified. There were no studies from Brazil.14
While the social and economic costs of disabling long-term IMD sequelae are poorly known, the direct impact they have on patients and the indirect consequences for caregivers, families and society are believed to be substantial. However, there is no consensus on the costs and medical resource use needed for treating long-term IMD sequelae in Brazil. The objectives of this study were 1) To identify evidence on the economic burden of long-term IMD sequelae from an integrative review with a broad scope, and 2) To conduct a Delphi survey, informed by the evidence identified, to reach consensus on the medical resource use and associated costs needed to treat long-term IMD sequelae in Brazil.
Material and methods
An integrative review with a broad scope was conducted to gather evidence to inform the Delphi survey in Brazil.
Integrative review
An integrative review was conducted (protocol CRD42022299697 registered in PROSPERO platform)15 to assess the global evidence on the costs of long-term IMD sequelae, from a payer, patient and societal perspective. The Medline, Embase, Cochrane Library and Lilacs databases were searched on October 20th, 2021 (Supplementary Material available on the Cambridge Core website) (no date restrictions nor filters for country were applied), for studies in English, Portuguese or Spanish, combining search terms relating to meningococcal disease and economic costs. The Rayyan web tool was used for reference management and duplicate removal. Screening of titles and abstracts and full-text articles was conducted by two researchers independently, with any discordances discussed with a third researcher (NTSF or MG) to achieve consensus.
Cost-of-illness studies or economic evaluations in any country addressing the economic impact of long-term sequelae in IMD cases of any age were included. Costs of interest included direct medical costs (e.g., medical resource use and patients’ out-of-pocket expenses for them); direct non-medical costs (e.g., patients’ out-of-pocket expenses for transportation, accommodation and other non-medical resources); indirect costs (e.g., time, income and productivity losses); special education and social care costs; and costs relating to specific sequelae. Studies were excluded if they assessed preventive measures, outbreaks, or diagnosis and treatment without presenting sequelae cost data. Systematic reviews, expert opinion reviews, conference abstracts, editorials, letters, comments, and study protocols were also excluded. Systematic reviews were only considered as a source to identify additional primary studies.
Data were extracted, by two researchers (JM and MK) independently and using the Covidence web tool, on study characteristics (i.e., country, study design, data source, currency, time horizon, study perspective, sample size, age group, and type of sequelae) and outcomes of interest (i.e., direct medical, non-medical and indirect costs, education and social care costs, sequelae-specific costs, cost of medical resources, procedures, services, and length of stay).
The quality of included studies was analyzed using the revised Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist.16
The costs of IMD sequelae are presented by country, time horizon and cost category (e.g., healthcare, social care, education, indirect costs) with a breakdown by type of cost within each category. Costs relating to specific sequelae are presented separately and categorized by physical, neurological and psychological sequelae.
Cost estimates were converted to 2021 International dollars (I$) using the national gross domestic product deflators and the implied purchasing power parity conversion rates from the International Monetary Fund. Currency conversion rates and inflation adjustments were applied using consumer price indexes.17^,^18 Studies that did not indicate the year of cost analysis were assumed to have the same base year as the year of publication.
Delphi survey
A Delphi survey, with two rounds, was conducted to estimate the use of medical and non-medical resources for treating long-term IMD sequelae in Brazil. This type of structured group communication process is used in health sciences to address data gaps, and can provide high levels of evidence when other approaches cannot be used.19
Participants (n = 33) from Brazil (including infectious disease experts from Brazil's public and/or private health system and parents of IMD patients) were invited to participate based on their experience with the treatment of IMD and familiarity with IMD sequelae.
A questionnaire was designed based on the integrative review findings to enquire about the use of medical resources for the seven most common types of sequelae identified from the review i.e., single limb amputation, multiple limb amputations, skin scarring, epilepsy/seizures, hearing loss/deafness, mental retardation/low IQ (Intelligence Quotient), and mental health disorder/anxiety/depression. The questionnaire was based on a cohort of Brazilian patients with a confirmed long-term IMD sequelae diagnosis and treated in the SUS and/or private health system. Participants were asked to provide information on medical resource use (e.g., medical visits, specialists, hospital days, rehabilitation, home adaptations) in the first Year (Y1) and in the Subsequent Year (SY) by sequela. In addition, participants were asked about indirect costs (e.g., need for paid caregiver, workdays lost) by sequela.
A week before the first round, a summary of the integrative review findings was emailed to all panel participants who agreed to be part of the study and provided informed consent. The questionnaire was then sent to all participants to start the first round. Participants were requested to complete and return the questionnaires to the research team within one week. Results (mean, minimum and maximum values for each question) from the first round were pooled and emailed to participants in the second round for their validation, in order to reach consensus on the final mean values to be reported.
A microcosting analysis based on the Delphi survey estimates was performed to evaluate the costs associated with treatment of long-term IMD sequelae from the public health system (Sistema Único de Saúde, SUS) SUS perspective. The codes for the procedures and their unit costs were sourced from the Table of Procedures, Drugs, Orthotics, Prosthetics and Special Materials (SIGTAP) from SUS. Cost data were sourced from public Brazilian databases including SIGTAP.20 Hospitals accredited by the SUS are paid by the Ministry of Health budget through reimbursement, and only procedures listed in SIGTAP are reimbursed, using a reference price list to calculate a minimum transfer of values from the Ministry of Health budget to hospitals. Although the reference price list was used for the cost estimates, there may still have been an underestimation of the actual hospital expenditure for long-term IMD sequelae. Considering SIGTAP unit costs only represent federal costs, they were adjusted by a correction factor of 2.8 to obtain the total cost. This correction factor was suggested by the Ministry of Health,21 and was also applied by the Comissão Nacional de Incorporação de Tecnologias (Brazil's National Commission for the Incorporation of Technologies ‒ CONITEC) in a cost-effectiveness analysis of COVID-19 (Coronavirus Disease 2019) vaccines.22^,^23 All costs were recorded in Brazilian Reals (R) based upon the official exchange rate for Jan‒June 2024 (US 5.04).
Results
Integrative review
The search strategy retrieved 2,838 unique records of which eight studies, published from 2011 to 2021, presented costs of IMD sequelae and were included (Fig. 1). All studies reported costs for IMD patients with a range of physical, neurological and psychological sequelae, except one study in the US (United States)24 which did not include psychological sequelae. Study designs included cost of illness (n = 1)25 and cohort studies (n = 2),24^,^26 economic models (n = 1),27 and studies estimating the costs of hypothetical severe IMD cases presenting with meningitis or septicemia (n = 4).28, 29, 30, 31 IMD patients of all ages were included. All studies were conducted in high-income countries and there were no studies identified in Latin America. Costs were provided from the payer perspective, patient and/or societal perspectives.Fig. 1PRISMA flow chart. IMD, Invasive Meningococcal Disease; n, number; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.Fig 1
There were two studies in France,25^,^30 one in Germany,31 one in Spain,29 one in the United Kingdom,28 two in Australia,26^,^27 and one in the US24 (see Table S2 for study details).
Studies in the UK (United Kingdom),28 Spain,29 and France30 estimated the costs associated with the lifetime management of a hypothetical severe case of IMD with sequelae in a young child, presenting either as septicemia or as meningitis. The cases were based on expert and family interviews. In the UK, the lifetime costs of IMD sequelae were assessed from the healthcare payer perspective, including medical, social services, education, and other government costs (e.g., for disability services, lost tax revenue, financial aid).28 In Spain, lifetime sequelae costs were estimated from the payer perspective, including medical, education and social care costs.29 The French study estimated lifetime costs of IMD sequelae from a payer, societal, and patient and health insurance perspective, including medical costs, education costs and revenue loss for parents.30
A cost of illness study in France assessed long-term sequelae costs, up to six years after IMD, using the national claims database (French National Healthcare Data System, [Système National des Données de Santé, SNDS]), in patients of all ages. Costs, from a payer perspective, included medical costs and sick leave and disability compensation.25
There were two modelling studies. A model-based costing study in Germany, in a cohort of hypothetical IMD patients of all ages, estimated sequelae costs over 14-years from a societal perspective, including medical and public health response costs, education costs and parental lost productivity costs.31 An economic model in Australia estimated the lifetime costs of sequelae in adults with IMD aged 20 or 30 years, from a payer and societal perspective, including medical costs, non-healthcare government subsidies, informal caregiver costs, education costs, home/vehicle modification costs, out-of-pocket costs, and productivity loss and premature death costs.27
There were two cohort studies assessing medical costs of IMD sequelae, from a payer perspective, over one year; a cohort study in Australian infants and children included acute hospitalization and readmission costs,26 and a US cohort study in IMD patients of all ages included medical costs based on a claims database analysis.24
Table 1 presents the breakdown of costs by country, time horizon and cost category, including direct medical costs (e.g., hospital, outpatient), costs for special education needs, social care costs, and indirect lost productivity costs for patients and/or their parent(s). The total costs by country are also presented, which include the costs of treating specific sequelae (presented separately in Table 2 where applicable).Table 1. Breakdown of costs of long-term IMD sequelae by country (International dollars [I)(Y1)Lifetime (or >Y1°)Direct medical costsGermany3114 Ya Acute phase (hospital, outpatient, rehabilitation, outbreak management)NR/NA17,614Australia261 YAcute care, readmission9,490NRAustralia261 YAcute care, first hospitalization34,983NRAustralia27LifetimeAcute admissionNR16,859Spain29LifetimeAcute care, meningitisNR175,669UK28LifetimeAcute care, meningitisNR238,291Spain29LifetimeAcute care, septicemiaNR216,814UK28LifetimeAcute care, septicemiaNR274,454US241 YHospitalization94,561NRFrance30LifetimeHospitalization (Societal), septicemiaNR87,745France30LifetimeHospitalization (Societal), meningitisNR68,710Germany3114 Ya Medical cost, sequelaeNR35,509France256 YHospital and community care, multiple sequelae31,880NRFrance256 YHospital and community care, multiple sequelae (Y2)NR28,427France256 YHospital and community care, multiple sequelae (Y5)NR12,270France256 YHospital and community care, single sequela20,467NRFrance256 YHospital and community care, single sequela (Y2)NR15,276France256 YHospital and community care, single sequela (Y5)NR7,119US241 YOutpatient16,700NRUK28LifetimeOutpatient, meningitisNR35,335France30LifetimeOutpatient (Societal), meningitisNR28,289Spain29LifetimeOutpatient, meningitisNR28,435UK28LifetimeOutpatient, septicemiaNR56,936France30LifetimeOutpatient (Societal), septicemiaNR42,512Spain29LifetimeOutpatient, septicemiaNR14,170Australia27LifetimeLong-term healthcare costNR12,661Australia27LifetimeLong-term disability careNR12,059US241 YHome health/equipment4,149NRUS241 YPhysician visits3,507NRUS241 YAncillary care2,544NRUS241 YPharmacy2,237NRUS241 YEmergency department1,550NRUS241 YLaboratory712NRSpecial education costsFrance30LifetimeEducation, meningitisNR1,249,674Spain29LifetimeEducation, meningitisNR240,771UK28LifetimeEducation, meningitisNR9,360France30LifetimeEducation, septicemiaNR149,967Spain29LifetimeEducation, septicemiaNR47,076UK28LifetimeEducation, septicemiaNR8,118Social care costsSpain29LifetimeSocial care, meningitis51,8881,431,364°UK28LifetimeSocial care, meningitisNR28,368Spain29LifetimeSocial care, septicemia44,626843,744°UK28LifetimeSocial care, septicemiaNR4,175Indirect costsGermany3114 Ya Productivity loss, patient or parent (Friction cost)NR1,783Germany3114 Ya Productivity loss, patient or parent (Human capital approach)NR129,953France30LifetimeRevenue loss, parent, meningitisNR238,064France30LifetimeRevenue loss, parent, septicemiaNR115,432Total costs by country and perspectiveFrance30LifetimeTotal (Patient/Insurance), meningitisNR386,922Total (Patient/Insurance), septicemiaNR152,237Total (Payer), meningitisNR2,490,100Total (Payer), septicemiaNR997,204Total (Societal), meningitis240,1632,877,023°Total (Societal), septicemia249,4951,149,441°Australia27Lifetimea Total (Payer)NR14,593a Total (Societal, Friction cost)NR25,188a Total (Societal, Human capital approach)NR56,707Spain29LifetimeTotal (Dictionary, #143), meningitis189,767532,076°Total (Dictionary, #143), septicemia261,993951,294°Total (Societal), meningitisNR2,204,209Total (Societal), septicemiaNR1,842,115UK28LifetimeTotal (Societal), meningitis701,0954,907,644°Total (Societal), septicemia571,2713,426,176°US241 YTotal (Payer)125,961NRIMD, Invasive Meningococcal Disease; UK, United Kingdom; US, United States; Y, Year; NR, Not Reported.° Some studies split costs by Year 1 and > Year 1 costs.aScholz et al. (2019)31 and Wang et al. (2019)27 provided some average costs per IMD case including non-sequelae cases.Table 2. Mean costs relating to specific sequela, by country (International dollars [I)Y1Lifetime (or > Y1)Physical sequelaeFrance255 YAmputation54,01823,653Australia23LifetimeAmputation, digit36,805Australia23LifetimeAmputation, single limb141,937Australia23LifetimeAmputation, multiple limbs253,519Australia23LifetimeArthritis6,695France255 YMotor deficits19,9747,421France30LifetimeProsthesis420,975UK22LifetimeProsthesis452,974Spain21LifetimeProsthesis652,225France255 YRenal disease25,67312,895Australia23LifetimeRenal failure, chronic281,316Australia23LifetimeSkin grafting8,969Spain21LifetimeStump revisions, skin grafting25,310UK22LifetimeStump revisions, skin grafting38,072France255 YSkin scarring44,87019,262Neurological sequelaeFrance255 YBlindness, severe visual impairment14,1468,025Australia23LifetimeBlindness44,203Australia23LifetimeBrain injuries25,402Australia23LifetimeChronic migraine11,038France255 YEpilepsy19,0316,223UK22LifetimeEpilepsy6,532Australia23LifetimeEpilepsy80,858Spain21LifetimeEpilepsy99,610Australia23LifetimeHearing loss, adaptation strategies6,435Australia23LifetimeHearing loss, hearing aid15,920Germany2014 YHearing loss25,509France255 YHearing loss, unilateral10,5042,065France255 YHearing loss, bilateral35,4954,900France255 YHearing loss, cochlear implant13,8412,719Spain21LifetimeHearing loss, cochlear implant14,349Australia23LifetimeHearing loss, cochlear implant21,179UK22LifetimeHearing loss, cochlear implant306,564France255 YMental retardation28,98829,802France255 YNeurological deficit, severe22,1299,879Spain21LifetimeShunt revision surgery12,689France30LifetimeShunt revision surgery23,181UK22LifetimeShunt revision surgery32,511France255 YSpeech or communication problems19,9174,518Australia23LifetimeSpeech problems, severe25,402Psychological sequelaeFrance255 YAnxiety11,2162,215Australia23LifetimeAnxiety, generalized disorder11,038UK22LifetimeBehavioral problems14,643France255 YDepression17,7536,074Australia23LifetimeDepression15,201France255 YHyperactivity syndrome14,9551,770Germany2014 YPsychological problems10,816Spain21LifetimePsychological problems36,283UK, United Kingdom; Y, Years.
Significant differences were observed for costs of education (range: I1,249,674) and social care (range: I843,744), which can vary according to the type and number of sequelae and the type or availability of services. For education, services may include special education needs, learning support assistance, school adaptations and equipment, transport from and to school, and specific services such as speech and language therapy and physiotherapy. For social care, costs may include day-care centers for activities, social care assessments, home visits and reviews.28, 29, 30
Costs associated with specific physical, neurological or psychological sequelae were reported in all countries except the US (Table 2). Costs of managing each sequela differed by study, with the highest costs observed for amputations, prosthesis, and chronic renal failure, among physical sequelae; hearing loss requiring cochlear implant and epilepsy among neurological sequelae; and psychological problems and depression, among psychological sequelae (Table 2). From the payer perspective, mean costs varied substantially by type of sequelae (e.g., I144,087 for amputation), by type of care (e.g., I67,038 for inpatient care), and by medical procedure (e.g., I508,735 for prosthesis).
Mean costs were calculated across studies adopting the provider perspective and applying a lifetime horizon (Fig. 2). The unweighted mean lifetime costs were: I58,314–75,763)30 for inpatient care; I12,059–56,936) for outpatient care27, 28, 29, 30; and for sequelae, they were I11,038 for anxiety to I36,283 for general psychological problems)[27](#bib0027), [28](#bib0028), [29](#bib0029); I37,201 (range: I6,532–99,610) for epilepsy/seizures[27](#bib0027), [28](#bib0028), [29](#bib0029); I14,511 for hearing loss (range: I21,179 for cochlear implant)27 ; I36,805 for single amputation to I252,519 for multiple amputations).[27](#bib0027) The unweighted mean lifetime costs of medical procedures[27](#bib0027), [28](#bib0028), [29](#bib0029), [30](#bib0030) were I508,735 (range: I106,455 (range I24,117 (range I22,794 (range: I248,161 (range: I223,043 (range: I4,175–843,744).[28](#bib0028), [29](#bib0029), [30](#bib0030)Fig. 2. Mean discounted lifetime costs and range (I) of long-term IMD sequelae. I$, International Dollars; IMD, Invasive Meningococcal Disease.Fig 2
Delphi panel
The previously described evidence was used to support the development of a Delphi questionnaire aimed to estimate medical Resource Use (RU) and caregiver productivity loss during the First Year (Y1) and the Subsequent Year (SY) for the most frequently reported sequelae in the literature (e.g., amputation, skin scars, hearing loss, epilepsy, mental retardation and mental health disorders, Fig. S1). Of the 33 participants invited to participate in the Delphi survey, five confirmed participation and provided informed consent, including three infectious disease doctors and two mothers of IMD patients. The survey group included individuals with diverse backgrounds and perspectives i.e., healthcare providers versus patients’ parents, public versus private sector, from different regions of Brazil (i.e., São Paulo in the Southeast, Pernambuco in the Northeast, Paraná in the South, Minas Gerais in the Southeast, and Rio de Janeiro in the Southeast).
All participants completed and returned the questionnaire in Round 1 and provided validation of the pooled results in Round 2. The Delphi survey reached a consensus on the mean, minimum and maximum values for most resources used. However, one participant did not answer all the questions and disagreed with the values reported for the number of physiotherapy sessions (i.e., participant reported 8 vs. 6 from the other participants) and the average number of working days lost (i.e., participant reported no value for SY vs. 28 days from the other participants). Both questions related to multiple limb amputations after the first year.
Additional comments provided by the participants highlighted that severity can have an important impact on the burden of IMD sequelae, including the need for rehabilitation or consultations; and the presence of multiple sequelae can affect burden and costs significantly. A case story by one participant highlighted the nature of long-term healthcare resource use and indirect costs (e.g., four months in the intensive care unit, various procedures and treatments including tracheostomy for seven months, need for home oxygen, prosthesis and use of orthoses due to amputations which required changes with growth, the need for a caregiver, and the need for parental caregiving as home care was only provided for eight months).
From the results of the Delphi survey, Fig. 3 presents the mean medical resource use needed to treat the seven sequelae, in the first Year (Y1) and the Subsequent Year (SY) of IMD (see Supplementary File for Delphi results by round).Fig. 3. Mean medical resource use (days or visits) by IMD sequela in (A) Year 1 (Y1) and Y1 + Subsequent Year (SY) and (B) subsequent year ‒ results from the Delphi survey for Brazil. IMD, Invasive Meningococcal Disease; IQ, Intelligence Quotient.Fig 3
The use of medical resources was significantly higher during Y1 compared with SY for all sequelae. Patients with single limb and multiple limb amputations had the highest overall medical resource use. All cases with a sequela required medical doctor visits (18‒40 in Y1 vs. 10‒20 SY), emergency department visits (13‒36 in Y1 vs. 5‒13 SY) and psychologist visits (48‒116 in Y1 vs. 24‒56 SY). Patients with amputations and skin scarring also required many inpatient hospital days (24‒28 in Y1 vs. 6‒8 SY). Patients with single or multiple limb amputations required physiotherapy visits (132‒149 in Y1 vs. 56‒70 SY) and orthotist visits (2 SY), and those with multiple limb amputation required 12 prosthetist visits (in Y1 and SY). There were 96 occupational therapist visits (in Y1 and SY) for patients with multiple limb amputations, and also for patients with mental retardation (36 in Y1 vs. 12 SY). Patients with skin scarring required outpatient visits for dressing (32 in Y1 vs. 14 SY). Patients with hearing loss or deafness required speech therapy visits (72 in Y1 vs. 36 SY) (Fig. 3).
The estimated per-patient costs of medical resource use to treat long-term IMD sequelae in the first and subsequent years of IMD are presented in Fig. 4. For amputation of a single limb, we estimated a cost of 902.73 for Y1 and SY, respectively. These costs were almost doubled (1,874.39 in SY) for multiple limb amputation. Costs for treatment of skin scarring sequelae were 816.19 in SY. For IMD-associated seizures, we estimated that the per-patient cost was 150.67 for SY, excluding the anticonvulsant therapy (which are mainly out of pocket expenses and reported by one of the respondents in the Delphi panel). For hearing loss, Y1 and SY costs were estimated at 355.11, respectively. It is noteworthy that hearing aid costs are not included in these estimates. Medical resource use costs were also estimated for mental retardation (317.44 for SY) and IMD-associated mental health disorders (240.22 for SY).Fig. 4. Total cost per patient (USD) by IMD sequela in (A) Year 1 (Y1) and (B) Subsequent Year (SY) ‒ results from the microcosting approach for Brazil. IMD, Invasive Meningococcal Disease; USD, US Dollar.Fig 4
Fig. 5 presents the mean number of working days lost for the treatment of the seven long-term IMD sequelae, in Y1 and Y1 + SY.Fig. 5. Mean number of working days lost by sequela, in (A) Year 1 (Y1) and Y1 + Subsequent Year (SY) and (B) subsequent year ‒ results from the Delphi survey for Brazil. IMD, Invasive Meningococcal Disease; IQ, Intelligence Quotient; Y, Year.Fig 5
The Delphi survey shows that all sequelae were associated with multiple working days lost, ranging from 33 for skin scarring to 85 for multiple limb amputations in Y1, and from 9 for skin scarring to 28 for multiple limb amputations SY. The mean number of working days lost was considerably higher in Y1 versus SY for all sequelae, representing an important indirect cost driver (Fig. 5). In addition, participants reported needing a paid caregiver for most of the sequelae in Y1 and SY.
Discussion
This study used an integrative review to identify the costs of long-term IMD sequelae from the payer, patient and societal perspectives. The findings informed a Delphi survey achieving a consensus from experts on the medical resources needed to treat specific IMD sequelae and their cost in Brazil, as well as the associated working days lost.
The review captured evidence from only high-income countries, on long-term direct medical costs, education and social care costs, and lost productivity costs associated with a range of physical, neurological and psychological IMD sequelae. There is a lack of evidence for Brazil, South America and other developing/emerging upper-middle income countries. The Delphi survey, among five medical experts and parents of IMD patients with sequelae, was the first study to provide information for Brazil on medical resource use and workdays lost for IMD sequelae. The findings highlight the significant resources needed, especially in the first year following IMD, for physical sequelae (e.g., limb amputations, skin scarring), neurological sequelae (e.g., epilepsy, hearing loss, mental retardation) and psychological sequelae (e.g., anxiety, depression). Patients with multiple limb amputations had the highest resource use (e.g., 28 inpatient days, 24 emergency visits, 29 doctor visits, 12 prosthetist visits, 72 psychologist visits, 96 speech therapy and occupational therapy visits, and 149 physiotherapy sessions in the first year alone), findings aligned with the integrative review. In the subsequent year, there was a decline in the number of inpatient days (6), medical visits (14), emergency visits (7), psychologist visits (42) and physiotherapy visits (70), other medical resource use remained high e.g., speech therapy (96) and occupational therapy (96). Participants commented on patients’ needs for long-term rehabilitation, and the presence of multiple sequelae. In one case story, the participant described the continuous need for changes to prostheses as the patient grew. These examples highlight the likely lifelong need for medical and other resources, which may not be fully captured in the Delphi survey. The microcosting approach allowed for an estimation of per-patient treatment costs, showing the substantial economic burden associated with the selected IMD sequelae. It is noteworthy that purchase of provisional and permanent orthosis as well as hearing aid costs and anticonvulsant use (for IMD-associated seizures) are not included in these estimates. In addition to the high healthcare burden, there was an important indirect cost driven by workdays lost; as caregivers of patients with IMD sequelae can expect to lose 33 to 85 working days in the first year due to sequelae.
Treatment cost estimates add to the body of evidence related to the economic burden of IMD in Brazil that has been mainly assessed from the healthcare perspective.4^,^10, 11, 12 In a study focusing on outbreak costs (i.e., disease surveillance and outbreak management), total costs have been estimated as high as three times the gross domestic product per capita.4 Another study estimated the direct hospital costs (2008‒2018) of several vaccine-preventable diseases; for IMD, over 24,000 hospitalizations occurred during the study period (almost 245,000 hospital days) costing the health system R 47,156,734.49.[11](#bib0011) A cost of illness study (only available as a conference abstract) estimated the direct medical costs (from the Unified Health System [*Sistema Único de Saúde*, SUS]) of IMD in 2,651 infants with IMD from 2007 to 2015, and the costs of their sequelae until the age of 18 years. The study assumed 23.9 % of cases had at least one sequela, the most common being deafness (28 %), epilepsy (28 %), amputation (9 %) and skin necrosis (9 %). The acute phase costs for diagnosis, inpatient care and chemoprophylaxis of contacts amounted to US1.1 million (2016USD); and sequelae treatment costs were estimated at US1,000–1,500 (2006 Brazilian Reals) in children under nine years, and sequelae costs were highest for neurological impairment (R19,154 including indirect costs).10 In a cost-effectiveness analysis assessing the impact of meningococcal vaccination in Brazil, authors estimated the input parameters for costs (direct and indirect) of treatment for IMD sequelae to range from R48,259 (neurological and hearing impairments).32 Variations in cost estimates were observed across the literature, depending on the type of care, treatments, and time-horizon taken into account. As highlighted by Itria and colleagues, input parameters for treatment costs of sequelae may substantially impact the cost-effectiveness assessment of vaccination.32
The integrative review was able to capture a broader range of study designs than traditional systematic reviews, including bottom-up costing studies for severe IMD cases with long-term disabilities, that were defined from expert interviews. These data provide new and important insights into the long-term needs of IMD patients and their families, and the significant healthcare, patient and societal costs of the disease. Key strengths of the Delphi survey were the inclusion of healthcare providers from public and private health sectors in Brazil, and parents of IMD patients providing a family perspective and details from a case study. The methodological approach, using anonymous participation and allowing freedom of expression, made it possible to avoid conflicts of interest within the group and to minimize dominance of researchers from any region that could influence the results.
No sequelae costing data were identified from low- and middle-income countries or Latin America, where the financial burden on patients and families may be even more severe due to precarious healthcare systems, and difficult to access or unavailable long-term and specialized healthcare services. In these circumstances, patients and caregivers are more likely to incur severe economic loss due to high out-of-pocket expenditures, income loss and reduced productivity.13 Impoverishment as a result of catastrophic health expenditure33 was not considered by any of the studies included in this review, but may well be applicable for IMD cases in developing countries. Furthermore, vulnerable people in the lowest socio-economic strata are at greater risk of infection, for example, from living in overcrowded housing. The risk and economic burden of IMD and its long-term sequelae may also be increased due to multimorbidity, such as HIV/AIDS (human immunodeficiency virus/acquired immunodeficiency syndrome) and smoking, which are also more prevalent in these countries.34
This study also has some limitations. The integrative review included cost estimates from severe case studies (i.e., studies reporting costs for two severe patients) which may not be generalized to all IMD patients. While healthcare costs were provided for specific sequelae in some studies, the indirect, education and social costs were not broken down by sequela. Heterogeneity in the types and severity of sequelae, the cost components included, and the study designs and methodologies made comparisons difficult. Sequela costs are likely to vary by severity, however, this level of detail was not available. Pooling data across studies was difficult, therefore, due to heterogeneity across countries and settings, differences in time horizons used, and lack of data on the severity of sequela, which is a major driver of resource use and costs. Low recruitment in the Delphi survey, with no participants from the North and Midwest regions of Brazil, also affected the generalizability of the findings, given the regional and cultural diversity in Brazil. In addition, as IMD can have a wide range of sequelae which can vary in severity across patients, the findings cannot be generalized across the IMD population, due to the low number of participants in the Delphi survey. More research is needed to obtain more granular data across a range of IMD patients from multiple regions of Brazil.
While the integrative review and Delphi survey confirmed that long-term IMD sequelae impose a severe economic burden on patients and the healthcare system, evidence gaps remain concerning patient out-of-pocket costs and the impact specific to low and middle-income countries. Future studies may address these gaps by adopting standardized costing approaches in Latin American countries to provide more accurate evidence for the region.
This study provides valuable information on the types of medical resources and non-health services needed to support IMD patients with long-term sequelae and can help inform policy makers about the need to finance and improve access to such services. The study also shows the high healthcare burden and budget impact of long-term sequelae. Results indicate that indirect costs from caregiver lost productivity contribute to the economic burden, and public policies and social protection mechanisms may be needed to protect families from financial hardship as a consequence of IMD sequelae.
Authors’ contributions
Concept and design: Thatiana Pinto.
Acquisition of data: Noemia Teixeira de Siqueira Filha, Fanny Cortes, Meline Kron, Maira Galdino da Rocha Pitta, Fernando Zanghelini.
Analysis and interpretation of data: Noemia Teixeira de Siqueira Filha, Fanny Cortes, Meline Kron, Maira Galdino da Rocha Pitta, Fernando Zanghelini, Bruna de Veras, Tatiane Almeida Menezes, Ana Medina, Lessandra Michelin, Thatiana Pinto.
Drafting of manuscript: Noemia Teixeira de Siqueira Filha, Fanny Cortes, Meline Kron, Fernando Zanghelini, Thatiana Pinto, Bruna de Veras.
Critical revision of the paper for important intellectual content: Noemia Teixeira de Siqueira Filha, Fanny Cortes, Meline Kron, Maira Galdino da Rocha Pitta, Fernando Zanghelini, Bruna de Veras, Tatiane Almeida Menezes, Ana Medina, Lessandra Michelin, Thatiana Pinto.
Obtaining funding: Noemia Teixeira de Siqueira Filha, Fanny Cortes, Meline Kron, Maira Galdino da Rocha Pitta, Fernando Zanghelini, Bruna de Veras, Tatiane Almeida Menezes, Ana Medina, Lessandra Michelin, Thatiana Pinto.
Administrative, technical, or logistic support: Noemia Teixeira de Siqueira Filha, Fanny Cortes, Meline Kron, Maira Galdino da Rocha Pitta, Fernando Zanghelini, Bruna de Veras, Tatiane Almeida Menezes, Ana Medina, Lessandra Michelin, Thatiana Pinto.
Supervision: Thatiana Pinto.
Financial support
GSK funded this study (VEO-000045). GSK was involved in all stages of study conduct, including analysis of the data. GSK also took in charge all costs associated with the development and publication of this manuscript.
Conflicts of interest
Ana Medina, Bruna de Veras, Lessandra Michelin and Thatiana Pinto are employed by GSK. Thatiana Pinto holds financial equities in GSK. Maira Galdino da Rocha Pitta, Noemia Teixeira de Siqueira Filha and Tatiane Almeida Menezes received funding from GSK for the submitted work. These authors declare no other financial and non-financial relationships and activities. Fanny Cortes, Fernando Zanghelini and Meline Kron declare no financial and non-financial relationships and activities and no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Silveira M.M.Mc Bride A.J.A.Trotter C.L.Invasive meningococcal disease in Brazil: a literature review Vittalle – Rev Ciências Saúde 322020165173
- 2Chicuto L.A.D.de Moraes C.Cássio de Moraes J.Sáfadi M.A.P.A critical analysis of serogroup B meningococcal disease burden in Brazil (2001‒2015): implications for public health decisions Hum Vaccin Immunother 162020194519503195178410.1080/21645515.2019.1700710 PMC 7482866 · doi ↗ · pubmed ↗
- 3Presa J.V.de Almeida R.S.Spinardi J.R.Cane A.Epidemiological burden of meningococcal disease in Brazil: a systematic literature review and database analysis Int J Inf Dis 8020191371463064120010.1016/j.ijid.2019.01.009 · doi ↗ · pubmed ↗
- 4Constenla D.Carvalho A.Alvis Guzmán N.Economic impact of meningococcal outbreaks in Brazil and Colombia Open Forum Infect Dis 22015 ofv 1672668882510.1093/ofid/ofv 167PMC 4682177 · doi ↗ · pubmed ↗
- 5de Moraes J.C.Barata R.B.Meningococcal disease in São Paulo, Brazil, in the 20th century: epidemiological characteristics Cad Saude Publica 212005145814711615815210.1590/s 0102-311x 2005000500019 · doi ↗ · pubmed ↗
- 6Ministério de Saúde. Secretaria de Vigilância em Saúde e Ambiente. Secretaria de Atenção Especializada à Saúde. Secretaria de Atenção Primária à Saúde. Nota técnica conjunta n° 46 2023. Available at: https://www.alagoas 24horas.com.br/wp-content/uploads/2023/10/Nota-Tecnica-Conjunta-no-462-023-SVSA-SAES-SAPS-MS.pdf. (Accessed December 10, 2023).
- 7Aparecido Nunes A.De Jesus Lopes De Abreu A.Cintra O.Cintra M.A.C.T.Barbosa Coelho E.Nogueira Castro De Barros E.Meningococcal disease epidemiology in Brazil (2005‒2018) and impact of Men C vaccination Vaccine 3920216056163335826210.1016/j.vaccine.2020.11.067 · doi ↗ · pubmed ↗
- 8Shen J.Begum N.Ruiz-Garcia Y.Martinon-Torres F.Bekkat-Berkani R.Meszaros K.Range of invasive meningococcal disease sequelae and health economic application - a systematic and clinical review BMC Public Health 22202210783564195510.1186/s 12889-022-13342-2PMC 9153861 · doi ↗ · pubmed ↗