The Impact of Avatar Appearance on the Persuasiveness of a Short Video Encouraging Physical Activity: A Randomized Observational Study
Momoko Tohyama, Ryo Momosaki, Kazuma Tora, Tsuyoshi Okuhara

TL;DR
This study found that avatars wearing white coats were seen as more persuasive and acceptable in health communication videos compared to those in hoodies.
Contribution
The study introduces the concept of medical avatars in health communication and evaluates their persuasiveness and acceptability.
Findings
Avatars in white coats (medical avatars) were rated higher in persuasiveness and acceptability than those in hoodies (nonmedical avatars).
Participants with prior avatar experience found medical avatars more persuasive and acceptable than nonmedical avatars.
Abstract
Background Avatars have been used as tools for communication in various fields. However, the characteristics of avatars useful for health communication remain unclear. This study aimed to examine the impact of medical avatars (MAs) on health communication. Methodology An anonymous questionnaire survey was conducted among individuals aged 18-59 years. Participants were randomly assigned to view one of four avatar-based videos (medical male, nonmedical male, medical female, or nonmedical female avatar). In this study, MAs were defined as those wearing white coats, while nonmedical avatars (NAs) wore hoodies. Total scores for perceived persuasiveness of the video, avatar acceptability, and exercise self-efficacy were then compared between the MA and NA groups. Results Overall, 309 participants were included in the analysis, with 160 (51.8%) classified into the MA group and 149 (48.2%)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
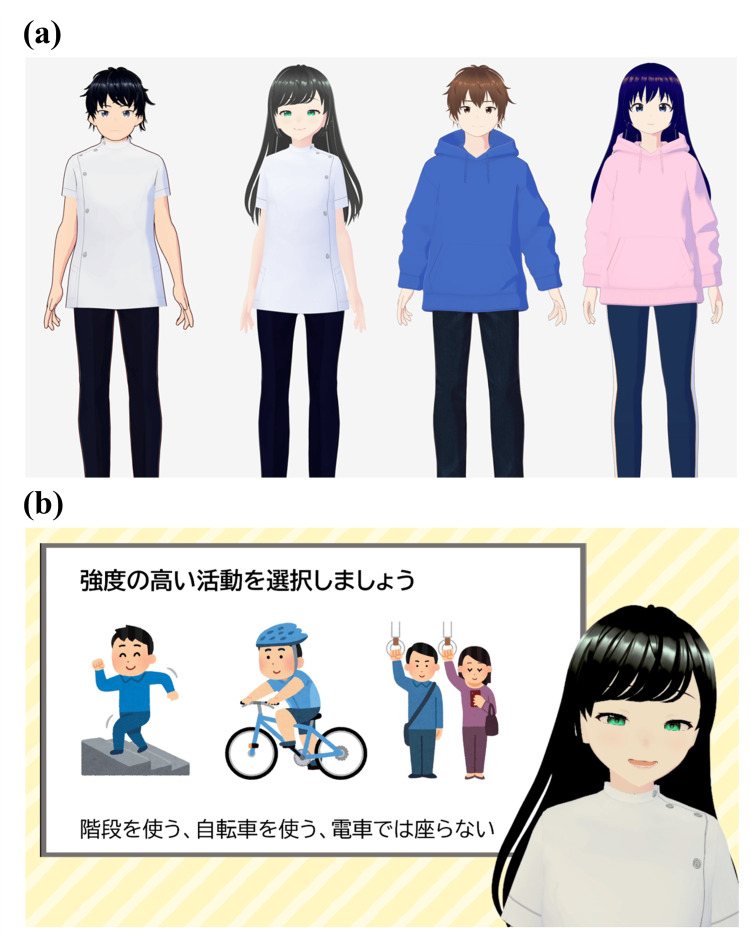 Figure 1
Figure 1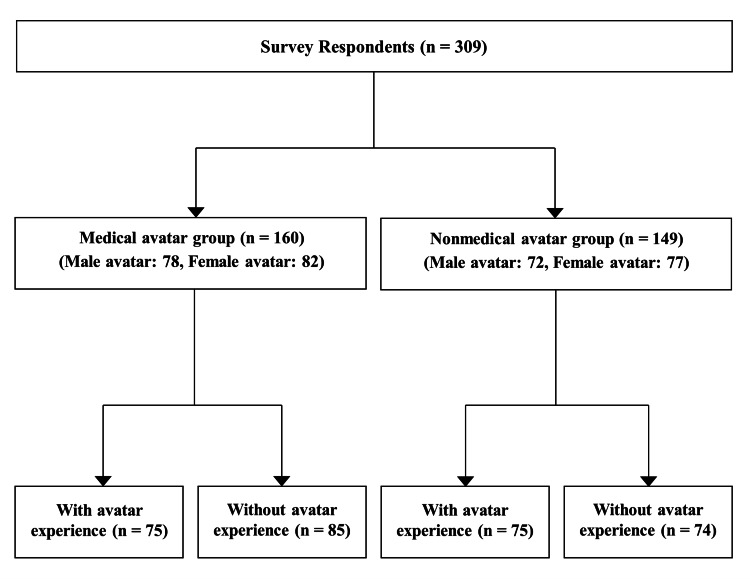 Figure 2
Figure 2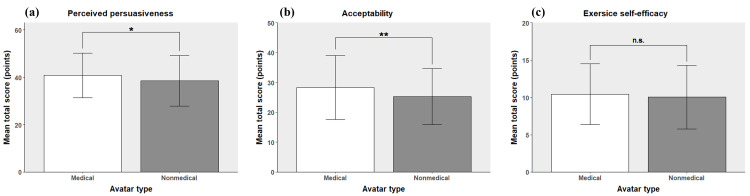 Figure 3
Figure 3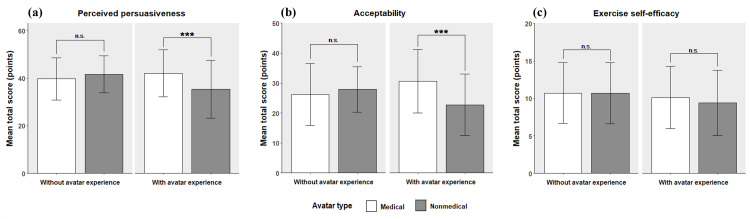 Figure 4
Figure 4| Characteristics | Medical avatar group ( | Nonmedical avatar group ( |
|
| Age (years), | 0.428 | ||
| 18-29 | 50 (31.3) | 53 (35.6) | |
| 30-39 | 60 (37.5) | 43 (28.9) | |
| 40-49 | 31 (19.4) | 35 (23.5) | |
| 50-59 | 19 (11.9) | 18 (12.1) | |
| Gender, | 0.510 | ||
| Male | 90 (56.3) | 74 (49.7) | |
| Female | 68 (42.5) | 73 (49.0) | |
| Other | 2 (1.3) | 2 (1.3) | |
| Healthcare students/professionals, | 107 (66.9) | 92 (61.7) | 0.347 |
| Educational levels, | 0.793 | ||
| <9 years | 2 (1.3) | 1 (0.7) | |
| 10-12 years | 21 (13.1) | 24 (16.1) | |
| >12 years | 135 (84.4) | 123 (82.6) | |
| Other | 2 (1.3) | 1 (0.7) | |
| Experience with avatars, | 75 (46.9) | 75 (50.3) | 0.543 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedia Influence and Health · Virtual Reality Applications and Impacts · Behavioral Health and Interventions
Introduction
Technological advancements have shifted lifestyles toward increased sedentary behavior, resulting in various health issues associated with reduced physical activity [1]. Previous studies have identified sedentary behavior and physical activity levels as independent risk factors for health and reported associations with all-cause mortality and incidence of noncommunicable diseases [2,3]. In particular, individuals with long screen time tend to have longer sedentary behavior, and a study indicated a link between sedentary time and depression [4]. Thus, measures aimed at reducing sedentary time and promoting physical activity are essential. Recently, digital technologies have gained attention as novel tools to enhance physical activity for their accessibility and potential for personalized interventions [5,6]. Educational interventions with digital technology may mitigate health risks associated with a sedentary lifestyle and promote sustainable health behaviors among a broader population.
In educational interventions, avatars are used to create digital content [7]. An avatar is a virtual object used to represent a physical entity, such as a human or an animal, which can perform relatively complex actions, including facial expressions and physical reactions [8]. Given their high level of psychological safety, avatars are increasingly used as a communication tool [9], a study examined the optimal characteristics of avatars for communication [10]. In addition, avatars are applied as marketing tools in customer service, guidance, and other business sectors [11]. Although avatar-based communication generally enhances efficiency and has a strong influence on younger generations, concerns about reliability and technical errors remain significant [11]. Ensuring the reliability of avatar use is an essential challenge.
In the medical field, the use of avatars has been explored for educational and counseling purposes. For instance, the efficacy of avatars in training and evaluating communication skills was investigated among healthcare professionals [12,13]. Previous studies have shown that avatar-based interventions are useful in the treatment of patients with mental illnesses and in education and health management for patients with chronic diseases [14-16]. These findings propose that avatar-based communication can foster a sense of security and enhance the self-efficacy, adherence, and knowledge of patients. Furthermore, in avatar-assisted counseling, the appearance of the avatar and the counseling situation have been shown to influence participants’ willingness to engage in counseling [17]. Thus, the use of avatars in healthcare for treatment and education has shown significant progress, and avatar-based health communication is expected to develop further.
However, the characteristics of avatars that are most useful for health communication remain underexplored. Specifically, which avatar features enhance communication persuasiveness to encourage healthy behavior is unclear. Previous studies have examined the association between the clothing of doctors or physical therapists and trustworthiness perceived by patients. For instance, a Japanese study assessed patient preferences and trust in various styles of doctor clothing (semiformal, white coats, surgical scrubs, and casual wear). Many patients chose white coats as the most preferred clothing for both male and female doctors, indicating that the clothing could affect the trust in medical professionals [18]. Rufa'i et al. examined the relationship between the clothing of physiotherapists and patients’ trust and comfort. The results showed that 89% of the participants reported higher trust in physiotherapists wearing white coats [19]. Therefore, wearing professional clothing, such as a white coat, is considered crucial in enhancing trustworthiness during medical or health-related communication. These findings indicate the potential applicability of video-based health communication using avatars, with the expectation that avatars resembling medical professionals could have similar positive impacts. The identification of the characteristics of avatars that are highly persuasive in health communication may contribute to the implementation of higher-quality health communication.
This study aimed to investigate the characteristics of avatars that enhance the quality of health communication through a questionnaire-based survey and hypothesized that using an avatar with a medical professional appearance could improve the quality of health communication. Participants watched videos featuring avatars, and perceived persuasiveness, acceptability, and exercise self-efficacy were assessed.
Materials and methods
Study design
This randomized observational study of Japanese participants examined the impact of medical avatars (MAs) on health communication. After providing consent, the participants viewed a video featuring an avatar and completed a questionnaire via Google Forms. Informed consent was obtained through an explanatory document attached to the Google Forms. This study was approved by the Ethics Committee of Mie University Hospital (H2024-136). As this is an observational study, clinical trial registration was not required.
Participants
This study included individuals aged 18-59 years who consented to participate in the study. Individuals unable to use the video-viewing devices were excluded from participation. Participants were recruited through posts on an account with approximately 1,800 followers on platform X. The survey was conducted from September 5 to October 6, 2024.
Sample size
The sample size was calculated using G*Power 3.1.9.7 (Heinrich Heine University, Düsseldorf, Germany), with a primary outcome comparison between the two groups using a t-test, effect size of 0.3, significance level of 5%, and power of 80%. According to Cohen’s guidelines, an effect size of 0.3 is considered small to medium [20]. This calculation resulted in an approximate sample size of 276 participants [21]. The target sample size was 300 participants aged 18-59 years.
Intervention content
Four types of avatars were created: male MA, female MA, male nonmedical avatar (NA), and female NA. To account for potential differences in how male and female participants might perceive avatars of the same or opposite sex, both male and female avatars were created for each avatar type (MA and NA). This design was implemented to control for any underlying sex-related biases or preferences in participants’ responses. The MA wore white coats, whereas the NA wore casual hoodies, with no other differences aside from appearance and gendered voices (Figure 1).
Visual representation of the videos.(a) Avatars used in the videos. (b) Screenshot of the video content as viewed, showing the text: “Choose high-intensity activities. For instance, take the stairs, ride a bicycle, and avoid sitting on the train."Screenshot of the video taken by co-author Ryo Momosaki.
Participants were randomly assigned to view one of these avatars. The assignment was conducted using the shuffle feature of Google Forms, which randomized the order in which the videos were displayed, although the specific algorithm behind the shuffle is not publicly disclosed. Participants were instructed to watch only the video that appeared at the top of the randomized list and report the corresponding video number. This method ensured random group allocation, minimizing allocation bias and maintaining equality across groups.
The videos were approximately 2 minutes long and highlighted the importance of exercise while introducing practical ways to increase physical activity levels. Participants were not provided with specific instructions regarding viewing conditions such as viewing time or device type.
Outcomes
The primary outcome was the total score for the perceived persuasiveness of the video to evaluate the overall impact of the avatar. Perceived persuasiveness was measured using the validated questionnaire of Thomas et al., comprising nine items across three factors: effectiveness, quality, and capability, rated on a 7-point scale from strongly disagree to strongly agree [22]. The secondary outcomes were the total scores for each of the following: acceptability of the avatar and exercise self-efficacy. Acceptability of the avatar was assessed using a 10-point scale questionnaire based on five items (knowledge, trust, care, approachability, and comfort), adapted from a systematic review investigating the impact of physicians’ clothing on patient preference and satisfaction [23]. In this study, a questionnaire on the acceptability of avatars was developed based on the study by Petrilli et al. [24]. Exercise self-efficacy was measured using a validated scale by Oka, assessing confidence in exercising under five conditions that could hinder physical activity: physical fatigue, mental stress, lack of time, non-routine life, and bad weather [25]. Responses were recorded on a 5-point scale from not at all confident to very confident. Scores were summed across all items, except for the non-routine life condition, which was an irrelevant item. All outcomes were measured immediately after viewing the video.
The extracted background information included age, gender, educational level, healthcare student or professional status, and experience with avatars. Avatar experience was defined based on whether the individual regularly watched avatar-based streams or videos, such as VTuber content, or frequently used avatars in games.
Statistical analysis
Participants were classified into the MA and NA groups based on the avatar type viewed, and the background characteristics and outcomes were compared. Because this study aimed to evaluate the impact of MAs on health communication, a gender-based analysis of the avatars was not performed. Categorical data were presented as absolute numbers and percentages and compared between the groups using the χ² test. Continuous data were presented as means ± standard deviations and compared using t-tests. Subgroup analysis based on avatar experience was also performed. Statistical analysis was conducted using SPSS version 29.0 (IBM Corp., Armonk, NY), with significance defined as two-sided (P < 0.05).
Results
In total, 309 participants completed the survey, with 160 viewing a video for MA and 149 viewing a video for NA (Figure 2). Participant characteristics are presented in Table 1. No significant differences were observed in gender, age, or other background characteristics between the MA and NA groups.
Overview of the study design.
Table 1: Baseline characteristics of the participants (n = 309).Note: Categorical data were analyzed using χ2 tests, and continuous data were analyzed using t-tests. Significance was set at P < 0.05.
Outcome comparisons between the groups are shown in Figure 3. The MA group had significantly higher scores for avatar perceived persuasiveness (40.79 ± 9.39 vs. 38.48 ± 10.65, P = 0.044) and acceptability (28.29 ± 10.67 vs. 25.30 ± 9.38, P = 0.009) than the NA group. No significant difference was found in exercise self-efficacy between the two groups (10.43 ± 4.09 vs. 10.04 ± 4.25, P = 0.419). The comparative results for all items are provided in Appendix A.
*Main results of the analysis.(a) Mean total score for perceived persuasiveness, (b) mean total score for acceptability, and (c) mean total score for exercise self-efficacy.Note: The significance of the results was determined using t-tests, with significance defined as P < 0.05. Bars represent the mean total scores for each measure, and error bars indicate ± standard deviation (SD). Significance is indicated as follows:*P < 0.05.**P < 0.01.**P < 0.001.Results with n.s. indicate no significant difference. The score ranges for each outcome were as follows: perceived persuasiveness (9-63), acceptability (5-50), and exercise self-efficacy (4-20).
The subgroup analysis based on avatar experience is shown in Figure 4. Among participants with avatar experience, the MA group scored significantly higher on perceived persuasiveness (42.03 ± 9.89 vs. 35.40 ± 12.19, P < 0.001) and acceptability (30.67 ± 10.58 vs. 22.76 ± 10.29, P < 0.001) than the NA group. In contrast, no significant differences were observed in perceived persuasiveness (39.71 ± 8.84 vs. 41.59 ± 7.75, P = 0.153), acceptability (26.20 ± 10.37 vs. 27.88 ± 7.60, P = 0.243), and exercise self-efficacy (10.69 ± 4.04 vs. 10.68 ± 4.08, P = 0.977) among participants without avatar experience. The comparative results for all items are provided in Appendix B.
*Results of the subgroup analysis.(a) Mean total score for perceived persuasiveness, (b) mean total score for acceptability, and (c) mean total score for exercise self-efficacy.Note: The significance of the results was determined using t-tests, with significance defined as P < 0.05. Bars represent the mean total scores for each measure, and error bars indicate ± standard deviation (SD). Significance is indicated as follows:*P < 0.05.**P < 0.01.**P < 0.001.Results with n.s. indicate no significant difference. The score ranges for each outcome were as follows: perceived persuasiveness (9-63), acceptability (5-50), and exercise self-efficacy (4-20).
Discussion
In this study, a questionnaire survey was conducted to examine the impact of MAs on health communication. The results indicated that avatars wearing white coats received higher ratings for perceived persuasiveness and acceptability than avatars wearing hoodies.
The MA group rated the persuasiveness and acceptability of the videos higher than the NA group; thus, these outcomes may be impacted by avatar appearance. In face-to-face communication, studies have shown that healthcare providers wearing professional clothing can enhance patients’ trust and sense of security [18,19,24,26]. Similarly, avatars dressed in professional clothing may increase perceived persuasiveness and acceptability in video-based health communication.
Despite similarities between the results of the previous study and the present study, the effect sizes were larger in the former. Specifically, in the previous study, the mean acceptability scores for doctors wearing white coats were all above 8 [24], whereas in the present study, the mean acceptability scores for avatars wearing white coats remained in the 5-point range. This difference may be explained by variations in the target population and the attributes of the speakers. The previous study focused on patients, whereas the present study included individuals aged 18-59. Patients may have been more strongly influenced by the acceptability of a physician’s clothing. Another factor to consider is the difference in speaker attributes. Although the previous study examined the acceptability of individuals explicitly identified as “doctors,” the present study did not specify the identity of the avatar. As a result, the lack of clarity regarding the title and expertise of the avatar may have reduced acceptability. These differences in target population and speaker attributes may have contributed to the differences in effect sizes.
The effect of avatar appearance on exercise self-efficacy was also investigated. However, no significant difference in self-efficacy was found between the MA and NA groups. This may reflect differences in participants’ stages of behavior change as per the transtheoretical model [27], indicating that the content may not have been optimal for enhancing exercise self-efficacy for all participants. Furthermore, the avatar video used in this study was only approximately 2 minutes long, which may not have been enough to positively impact self-efficacy. Thus, identifying avatar characteristics that are useful in improving self-efficacy will require intervention studies with adequately timed, personalized video content.
A subgroup analysis based on avatar experience was conducted. Among participants with avatar experience, the MA group rated the perceived persuasiveness and avatar acceptability higher than the NA group. However, among participants without avatar experience, no difference was found between the two avatar types across any of the items. This indicates that among individuals with avatar experience, the appearance of avatars may influence the trustworthiness of the video and acceptability, whereas individuals without avatar experience are less impacted by the appearance of the avatar. Although this is currently a hypothesis, the results may be due to the higher attention to avatars among experienced users, making them more receptive to the avatar appearance. Future studies should investigate the association between avatar experience and attention to avatars.
To the best of our knowledge, this is the first study that examined the impact of MAs on health communication. Four types of avatar videos were used in this study: male MA, female MA, male NA and female NA. The inclusion of both male and female avatars enabled us to control for the impacts of avatar gender, which is often cited as a limitation in avatar and YouTuber research [28], thus allowing a clearer comparison of the impact of avatar appearance.
However, this study has several limitations. First, the generalizability of the results is limited because participants were recruited through social media, excluding those who do not use such platforms. Second, our study focused on health communication, which may have attracted individuals with a particular interest in the topic, potentially introducing selection bias. Third, environmental factors such as viewing time, location, and device were not controlled, which might have influenced participants’ psychological responses. Finally, this study evaluated perceived persuasiveness and acceptability immediately after video viewing and therefore could not assess long-term impacts such as behavior change.
Conclusions
In this study, avatar appearance was found to influence the perceived trustworthiness and acceptability of videos in health communication. Avatars wearing white coats were associated with higher trustworthiness and acceptability. These findings indicate that tailoring avatar appearance may enhance the quality of health communication.
Future research should investigate the long-term effects of avatar appearance on behavior change and health outcomes. In addition, examining how not only avatar attire but also other customization factors, such as voice, personality traits, and speaking style-affect the effectiveness of avatar-based interventions is important. Identifying optimal methods for video-based health communication may improve patient education and contribute to better health outcomes on a population level.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sedentarism and chronic health problems Korean J Fam Med Goyal J Rakhra G 2392574520243932709410.4082/kjfm.24.0099 PMC 11427223 · doi ↗ · pubmed ↗
- 2Sedentary behavior patterns and the risk of non-communicable diseases and all-cause mortality: a systematic review and meta-analysis Int J Nurs Stud Wu J Fu Y Chen D 10456314620233752395210.1016/j.ijnurstu.2023.104563 · doi ↗ · pubmed ↗
- 3The physiological benefits of sitting less and moving more: opportunities for future research Prog Cardiovasc Dis Hwang CL Chen SH Chou CH 61667320223345328510.1016/j.pcad.2020.12.010PMC 8628304 · doi ↗ · pubmed ↗
- 4The associations between screen time-based sedentary behavior and depression: a systematic review and meta-analysis BMC Public Health Wang X Li Y Fan H 15241920193172705210.1186/s 12889-019-7904-9PMC 6857327 · doi ↗ · pubmed ↗
- 5Effectiveness of workplace interventions with digital elements to reduce sedentary behaviours in office employees: a systematic review and meta-analysis Int J Behav Nutr Phys Act Parés-Salomón I Señé-Mir AM Martín-Bozas F 412120243864181610.1186/s 12966-024-01595-6PMC 11031993 · doi ↗ · pubmed ↗
- 6Behavior change techniques and the effects associated with digital behavior change interventions in sedentary behavior in the clinical population: a systematic review Front Digit Health Martín-Martín J Roldán-Jiménez C De-Torres I 620383320213471309710.3389/fdgth.2021.620383 PMC 8521816 · doi ↗ · pubmed ↗
- 7Assessment of interest in a virtual avatar-based nutrition education program among youth-serving community partners J Nutr Educ Behav Enahora B Tripicchio GL Kopper R 7197275620243903345810.1016/j.jneb.2024.06.005 · doi ↗ · pubmed ↗
- 8Agency for Healthcare Research and Quality: Healthcare Simulation Dictionary 10 2024 2020 https://www.ahrq.gov/patient-safety/resources/simulation/terms.html