Positive Murphy's Sign of Fitz-Hugh-Curtis Syndrome
Kotaro Kunitomo, Yukinori Harada, Takahiro Tsuji, Taro Shimizu

TL;DR
A woman with right upper quadrant pain was diagnosed with Fitz-Hugh-Curtis syndrome after initial misdiagnosis, highlighting the importance of considering this condition in similar cases.
Contribution
This case emphasizes the need for thorough evaluation and history-taking to diagnose Fitz-Hugh-Curtis syndrome in patients with atypical presentations.
Findings
Right upper quadrant pain with a positive Murphy's sign can be caused by Fitz-Hugh-Curtis syndrome, not biliary disease.
A detailed patient history, including pelvic inflammatory disease symptoms, is crucial for accurate diagnosis.
Treatment with ceftriaxone and minocycline resolved the patient's symptoms within seven days.
Abstract
A Japanese woman in her 30s presented to the emergency department at midnight with right upper quadrant pain that had lasted for a week. Without a definitive diagnosis, she was prescribed acetaminophen and levofloxacin and discharged. When her pain persisted the next morning, she visited her primary care physician and reported fever and right upper quadrant pain. She was referred back to the emergency department with suspected cholecystitis. The patient's vital signs were stable, including a temperature of 36.6°C. Physical examination revealed right upper abdominal tenderness and a positive Murphy's sign, but no other abdominal tenderness. Laboratory tests showed normal white blood cell count and liver enzymes and a slightly elevated C-reactive protein concentration (2.44 mg/dL). Abdominal ultrasound showed no abnormalities. Further questioning revealed a history of unprotected sex,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
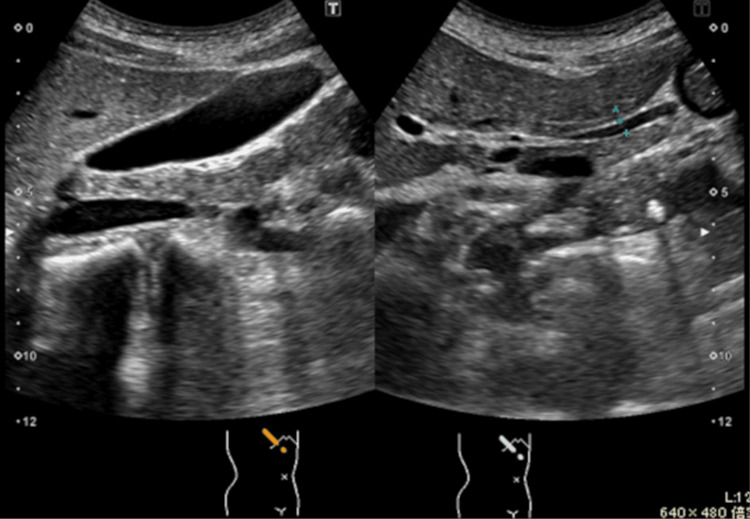 Figure 1
Figure 1| Parameter | Result (unit) | Reference range (unit) |
| White blood cell count | 8.3×10³/μL | 3.3-8.6×10³/μL |
| Aspartate aminotransferase | 11 U/L | 13-30 U/L |
| Alanine aminotransferase | 9 U/L | 7-23 U/L |
| Gamma-glutamyl transpeptidase | 20 U/L | 9-32 U/L |
| Alkaline phosphatase | 60 U/L | 38-113 U/L |
| C-reactive protein | 2.44 mg/dL | <0.14 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical Reasoning and Diagnostic Skills · Adrenal Hormones and Disorders · Empathy and Medical Education
Introduction
Murphy's sign is a clinical finding often associated with acute cholecystitis and is characterized by pain elicited during palpation of the right upper quadrant while the patient inhales deeply. While Murphy's sign has a high sensitivity (97%) for diagnosing acute cholecystitis, its low specificity (48%) necessitates careful interpretation, as a positive result does not definitively indicate acute cholecystitis [1].
Fitz-Hugh-Curtis syndrome (FHCS) is a rare complication of pelvic inflammatory disease (PID) characterized by perihepatic inflammation and adhesions between the liver capsule and the peritoneum. It has been reported to occur in 4-27% of women with PID [1]. It has been noted that the microorganisms associated with PID can spread in three ways: spontaneous ascending infection, hematogenous spread, and lymphatic spread [2]. It commonly presents with right upper quadrant pain and can mimic hepatobiliary and other abdominal diseases, as acute cholecystitis, cholelithiasis, right-sided pyelonephritis, pleurisy, and pulmonary embolism are the differential diagnoses [3-5]. Previous reports have documented cases of FHCS initially misdiagnosed as acute cholecystitis, leading to delays in appropriate treatment [6-8].
This case highlights the importance of comprehensive clinical evaluation, including a detailed history and consideration of atypical presentations, to distinguish FHCS from other causes of right upper quadrant pain. Early diagnosis is essential to prevent complications and achieve favorable outcomes in patients with FHCS.
Case presentation
A Japanese woman in her 30s visited the emergency department with right upper quadrant abdominal pain. No definitive diagnosis was made at that time. She was prescribed acetaminophen and levofloxacin and discharged home. However, she visited her primary care physician because her symptoms did not improve by the next morning. She reported right upper quadrant abdominal pain and fever and was referred to the emergency department with a suspected diagnosis of cholecystitis. She had a history of endometriosis and no history of trauma. She had no nausea, vomiting, pain during urination, or frequent urination. Her last menstrual period was 14 days ago. Her temperature was 36.6°C, and other vital signs were normal. Physical examination revealed tenderness in the right upper abdomen and a positive Murphy's sign. No tenderness was noted in other areas of the abdomen. She also complained of pain during inhalation, but other aggravating and relieving factors were unknown. Her pregnancy test was negative. The blood test results are provided in Table 1.
C-reactive protein was mildly elevated, but there were no other abnormalities. Abdominal ultrasonography showed no gallstones, gallbladder wall thickening, gallbladder enlargement, or bile duct dilatation (Figure 1).
Abdominal ultrasound findings not suggestive of biliary disease
At this time, we reevaluated the medical history of the patient. She reported unprotected sexual intercourse, lower abdominal pain that preceded the onset of pain in the right hypochondrium about a week earlier, and increased vaginal discharge. She noted that she had not reported the lower abdominal pain as it had resolved within a few days. Due to the increased likelihood of PID and FHCS, a polymerase chain reaction test of the urine for Chlamydia trachomatis was performed, yielding a positive result. Tests for syphilis, gonorrhea, and human immunodeficiency virus were negative. The patient was diagnosed with FHCS and treated with seven days of antimicrobial therapy (ceftriaxone 2 g/day and minocycline hydrochloride 200 mg/day). After completing treatment, her symptoms improved. We also recommended that her partner undergo testing and receive appropriate treatment.
Discussion
In this case, the presence of a positive Murphy's sign initially led to the suspicion of biliary disease, especially acute cholecystitis. This illustrates the availability bias, a type of cognitive bias, where the physician, influenced by the prominent finding, linked Murphy's sign directly to acute cholecystitis. In addition, as the patient did not initially report lower abdominal pain, FHCS was not considered in the differential diagnosis.
FHCS is a rare complication of PID characterized by perihepatic adhesions between the liver capsule and the abdominal wall. These adhesions cause right upper quadrant pain, which is often exacerbated by respiration due to movement of the liver against the inflamed peritoneum [4]. This pain can mimic what is associated with biliary disease and result in a positive Murphy's sign, increasing the likelihood of misdiagnosis. Cases of FHCS with positive Murphy's sign have been reported, and FHCS can be misdiagnosed as acute cholecystitis in clinical practice [1,3]. In the absence of imaging findings suggestive of biliary disease despite a positive Murphy's sign, inflammation of the peritoneum on the surface of the liver should be considered. Recognizing the potential for FHCS to mimic biliary disease is essential to prevent delays in diagnosis and ensure timely, effective management. Early treatment of FHCS is important to minimize the risk of infertility [2].
Approximately half of patients with FHCS present with isolated right upper quadrant pain without lower abdominal pain [6,9], making the differentiation of biliary diseases challenging. However, lower abdominal pain, which is often associated with PID, is critical in diagnosing FHCS. Thus, despite transient symptoms suggestive of PID, such as lower abdominal pain and tenderness, obtaining a detailed patient history is essential [10]. In this case, the absence of findings indicative of biliary disease, such as abnormal imaging findings, created a discrepancy that prompted a reassessment of the initial diagnosis, ultimately leading to the diagnosis of FHCS.
While the differentiation between FHCS and cholecystitis can be difficult, imaging findings such as the presence of small, avascular peritoneal masses at the upper dome of the liver on ultrasound have been reported as a useful diagnostic feature for FHCS [11]. Although such findings were not observed in this case, the potential of non-invasive imaging modalities to aid in distinguishing FHCS from biliary disease is noteworthy.
Conclusions
In a young woman with a positive Murphy's sign but no imaging findings suggestive of biliary disease, the diagnosis should be reconsidered to include inflammation of the peritoneum on the liver surface. Furthermore, for female patients with right upper quadrant abdominal pain, reevaluating the detailed history for signs of PID is crucial, as lower abdominal pain and tenderness may resolve during the clinical course. These approaches can help reduce diagnostic errors associated with FHCS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fitz-Hugh-Curtis syndrome: a diagnosis to consider in a woman with right upper quadrant abdominal pain without gallstones Eur J Case Rep Intern Med FaréPB Allio I Monotti R Foieni F 7435201810.12890/2017_000743 PMC 634693230756005 · doi ↗ · pubmed ↗
- 2Fitz-Hugh-Curtis syndrome Stat Pearls [Internet] Basit H Pop A Malik A Sharma S Treasure Island (FL)Stat Pearls Publishing 2023 https://pubmed.ncbi.nlm.nih.gov/29763125/29763125 · pubmed ↗
- 3Right upper quadrant pain with positive Murphy's sign in a 19-year-old woman Gastroenterology Matsuura H Kishida M Shimizu W 04158202010.1053/j.gastro.2019.10.04631738915 · doi ↗ · pubmed ↗
- 4Fitz-Hugh-Curtis syndrome Gynecol Surg Theofanakis CP Kyriakidis AV 12913482011
- 5Fitz-Hugh-Curtis syndrome: a cause of right upper quadrant abdominal pain Med Clin (Barc) Sánchez-Oro R Jara-Díaz AM Martínez-Sanz G 44745215420203214598810.1016/j.medcli.2020.01.022 · doi ↗ · pubmed ↗
- 6Clinical outcome of Fitz-Hugh-Curtis syndrome mimicking acute biliary disease World J Gastroenterol Woo SY Kim JI Cheung DY Cho SH Park SH Han JY Kim JK 697569801420081905833410.3748/wjg.14.6975 PMC 2773862 · doi ↗ · pubmed ↗
- 7Two cases of Fitz-Hugh-Curtis syndrome in acute phase [Article in Korean]Korean J Gastroenterol Lee SC Nah BG Kim HS 137142452005 https://pubmed.ncbi.nlm.nih.gov/15725719/15725719 · pubmed ↗
- 8A case of Fitz Hugh Curtis syndrome mimicking an acute abdomen Med Pharm Rep Mihetiu A Bratu D Popescu O Catana A 5215259420213610549210.15386/mpr-1890 PMC 9389874 · doi ↗ · pubmed ↗