High-Intensity Interval Training for Individuals With Isolated Impaired Fasting Glucose: Protocol for a Proof-of-Concept Randomized Controlled Trial
Sathish Thirunavukkarasu, Thomas R Ziegler, Mary Beth Weber, Lisa Staimez, Felipe Lobelo, Mindy L Millard-Stafford, Michael D Schmidt, Aravind Venkatachalam, Ram Bajpai, Farah El Fil, Maria Prokou, Siya Kumar, Robyn J Tapp, Jonathan E Shaw, Francisco J Pasquel, Joe R Nocera

TL;DR
This study tests if high-intensity interval training helps prevent type 2 diabetes in people with impaired fasting glucose.
Contribution
It introduces a tailored HIIT intervention for individuals with isolated impaired fasting glucose.
Findings
HIIT feasibility and acceptability will be assessed in a high-risk diabetes group.
The study will track glucose levels and clinical outcomes over an 8-week intervention.
Results may inform future trials on diabetes prevention through exercise.
Abstract
Standard lifestyle interventions have shown limited efficacy in preventing type 2 diabetes among individuals with isolated impaired fasting glucose (i-IFG). Hence, tailored intervention approaches are necessary for this high-risk group. This study aims to (1) assess the feasibility of conducting a high-intensity interval training (HIIT) study and the intervention acceptability among individuals with i-IFG, and (2) investigate the preliminary efficacy of HIIT in reducing fasting plasma glucose levels and addressing the underlying pathophysiology of i-IFG. This study is a 1:1 proof-of-concept randomized controlled trial involving 34 physically inactive individuals (aged 35-65 years) who are overweight or obese and have i-IFG. Individuals will undergo a 3-step screening procedure to determine their eligibility: step 1 involves obtaining clinical information from electronic health…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
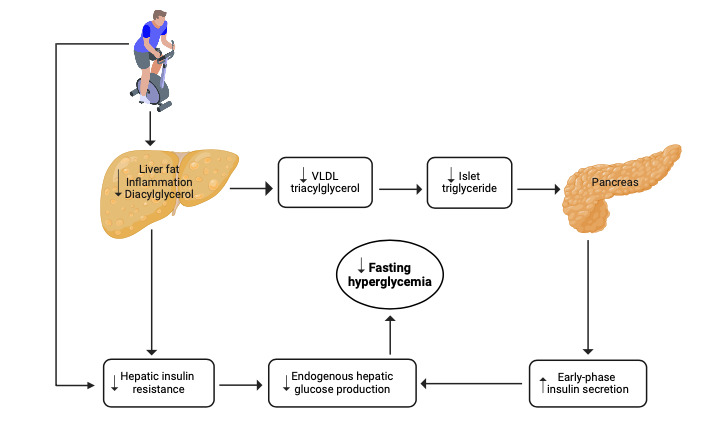 Figure 1
Figure 1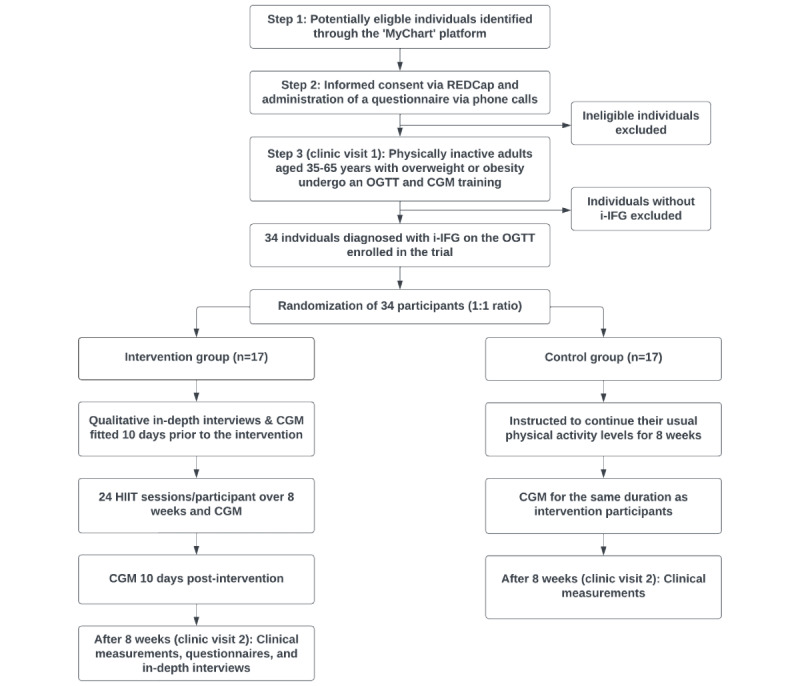 Figure 2
Figure 2| Variables | Components | Study tools | Baseline | 8 weeks | |
| Study feasibility | Response rate, screening yield, enrollment rate, time to enrollment, intervention compliance, resource use, and retention rate | REDCapa database | ✓ | ✓ | |
| Intervention feasibility | Qualitative and quantitative research | Feasibility of Intervention Measure [ | ✓ | ✓ | |
| Intervention feasibility | Qualitative and quantitative research | In-depth interviews | ✓ | ✓ | |
| Intervention acceptability | Qualitative and quantitative research | Theoretical Framework of Acceptability questionnaire [ | ✓ | ✓ | |
| Intervention acceptability | Qualitative and quantitative research | In-depth interviews | ✓ | ✓ | |
| Intervention appropriateness | Qualitative and quantitative research | Intervention Appropriate Measure [ | ✓ | ✓ | |
| Intervention appropriateness | Qualitative and quantitative research | In-depth interviews | ✓ | ✓ | |
| Participants’ expectations of and experiences with the intervention | Qualitative research | In-depth interviews | ✓ | ✓ | |
| Sociodemographics | Age, sex, marital status, education, and occupation | WHO STEPSb [ | ✓ | xc | |
| Eligibility criteria | Inclusion and exclusion criteriae | Short-form IPAQf [ | ✓ | x | |
| Behavioral measures | Dietary habits | ASA24g dietary assessment tool [ | ✓h | ✓h | |
| Behavioral measures | Physical activity | Short-form IPAQ [ | ✓i | ✓i | |
| Behavioral measures | Smoking | WHO STEPS [ | ✓ | ✓ | |
| Behavioral measures | Alcohol consumption | WHO STEPS [ | ✓ | ✓ | |
| Physical measures | Height | Stadiometer | ✓ | x | |
| Physical measures | Weight | Digital weighing scale | ✓ | ✓ | |
| Physical measures | Waist circumference | Inelastic measuring tape | ✓ | ✓ | |
| Physical measures | Hip circumference | Inelastic measuring tape | ✓ | ✓ | |
| Physical measures | BPj | DINAMAP BP apparatus | ✓ | ✓ | |
| Physical measures | Body composition | Bioimpedance analysis | ✓ | ✓ | |
| Biochemical measures | OGTTk (0, 30, and 120 minutes) | Enzymatic assays | ✓ | ✓ | |
| Biochemical measures | Insulin levels at 0 and 30 minutes | Immunoassays | ✓ | ✓ | |
| CGMk | Proportion of time and mean time spent in nocturnal (00:00-06:00) normoglycemia (60 to <100 mg/dl) [ | Dexcom G6 Pro (DexCom, Inc) | ✓l | ✓l | |
| Parameters | Calculations |
| Response rate |
Number of individuals responded to the invitation/number of individuals invited |
| Screening yield |
Number of individuals diagnosed with i-IFGa/number of individuals screened |
| Enrollment rate |
Number of individuals enrolled/number of individuals diagnosed with i-IFG |
| Time to enrollment |
Average time taken from sending the invitation to enrolling one participant in the trial |
| Intervention compliance |
Number of HIITb sessions attended/Total number of HIIT sessions |
| Resource use |
Program costs: Includes screening cost, cost of procedures, intervention cost, participant incentives, and other costs. Staff time: Time spent screening and recruiting participants, time spent delivering the intervention, time spent making phone calls to participants, time spent implementing the study procedures, and time spent on baseline and follow-up assessments. |
| Retention rate |
Number of participants attended follow-up visits/number of participants enrolled |
| ß cell function or IRa and components | Indices | Formula | |
|
| |||
|
| Early-phase insulin secretion: | IGIb [ | (I30c–I0d)/(G30e–G0f) |
|
| ß cell function | DIOg [ | ([ I0-30/ G0-30]×[1/I0]) I0 in µU/l G0 in mmol/l |
|
| ß cell function | HOMA-Bh [ | (20×I0)/(G0–3.5) I0 in µU/l G0 in mmol/l |
|
| |||
|
| Whole-body insulin sensitivity | Matsuda index [ | 10,000 /√((G0×I0)×(Gmeani×Imeanj)) |
|
| Insulin resistance | HOMA-IRk [ | (I0×G0)/22.5 I0 in µU/L G0 in mmol/l |
|
| Hepatic insulin resistance | HIRIl [ | (G0–G30[AUCm]×I0-30[AUC]) G0 in mg/dl I0 in µU/ml |
|
| Muscle insulin resistance | MISIn [ | (dG/dto)/Īp |
| Study stage | Challenges | Mitigation strategies |
| Identifying potential participants | Insufficient number of potentially eligible individuals |
We will use physician referrals as an additional recruitment strategy. |
| Screening | Low yield of screening |
The 3-step screening procedure was carefully designed, drawing upon insights from our previous research and existing literature, to target individuals who are likely to have i-IFGa. |
| Intervention | Low HIITb compliance |
The study coordinator will remind participants of their scheduled exercise sessions through phone calls. Additionally, the coordinator will regularly review the attendance log, providing motivation and support to participants with low attendance levels. The exercise instructor will hold weekly one-on-one meetings with participants to review their progress and provide motivation, specifically targeting those with low attendance levels. |
| Procedures | Periodic data gaps with CGMc whenever the receiver is located more than 5 feet |
The CGM data will be assessed for adequacy based on the following criteria: Data points must be present for at least 80% of the possible 288 glucose values per day for any 7 consecutive days, starting on the day after sensor insertion. |
| Follow-up | Low retention rate |
Compensation for time and parking: (1) participants will receive a US $50 gift card upon completion of the study and (2) parking fees at study sites will be covered. Building rapport: study staff will create a warm and supportive environment during study visits, fostering a sense of trust and comfort. Ongoing support: the study coordinator will provide continuous support through regular phone calls. This proactive approach ensures that participants feel connected to the study outside of scheduled visits. The study coordinator will address any concerns, answer queries, and offer encouragement, reinforcing a sense of partnership between participants and the research team. |
|
| 2023 | 2024 | 2025 | ||||||||
|
| May | July-December | January-March | April-June | July-September | October-December | January-March | April-June | July-September | October-December | |
| Received funding | ✓ |
|
|
|
|
|
|
|
|
| |
| Finalizing the study protocol and study tools |
| ✓ |
|
|
|
|
|
|
|
| |
| Clinical trial registration |
| ✓ |
|
|
|
|
|
|
|
| |
| Obtaining approvals: NIHb, NCATSc, and IRBd |
|
| ✓ | ✓ | ✓ |
|
|
|
|
| |
| REDCap database setup |
|
|
|
|
| ✓ |
|
|
|
| |
| Screening and recruitment |
|
|
|
|
|
| ✓ | ✓ |
|
| |
| Baseline assessments |
|
|
|
|
|
| ✓ | ✓ |
|
| |
| Baseline in-depth interviews |
|
|
|
|
|
| ✓ | ✓ |
|
| |
| HIITe intervention |
|
|
|
|
|
| ✓ | ✓ |
|
| |
| 8-week assessments |
|
|
|
|
|
|
|
| ✓ |
| |
| In-depth interviews at 8 weeks |
|
|
|
|
|
|
|
| ✓ |
| |
| Data entry |
|
|
|
|
|
| ✓ | ✓ | ✓ |
| |
| Data analysis |
|
|
|
|
|
|
|
| ✓ | ✓ | |
| Study report and publications |
|
|
|
|
|
|
|
|
| ✓ | |
| Conferences and scientific meetings |
|
|
|
|
|
|
|
|
| ✓ | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Management and Research · Hyperglycemia and glycemic control in critically ill and hospitalized patients · Diabetes, Cardiovascular Risks, and Lipoproteins
Introduction
The prevalence of type 2 diabetes is increasing globally [1-3], driven predominantly by a rising number of individuals with prediabetes [2]. Globally, an estimated 860 million (8.4%) adults are living with prediabetes, a condition that increases the risk of developing type 2 diabetes [2], micro- and macrovascular complications, and mortality [4].
Prediabetes is not a singular entity but rather a heterogeneous group of metabolic defects that often precede type 2 diabetes [5-7]. Prediabetes phenotypes include isolated impaired fasting glucose (i-IFG), isolated impaired glucose tolerance (i-IGT), and IFG + IGT. Each prediabetes phenotype exhibits distinct pathophysiological abnormalities [5-7]. i-IFG is marked by impaired early-phase insulin secretion and hepatic insulin resistance. Conversely, i-IGT involves impairments in both early- and late-phase insulin secretion and skeletal muscle insulin resistance [5,7]. IFG + IGT presents a combination of defects observed in both i-IFG and i-IGT [5,7]. i-IFG accounts for a substantial portion of the global prediabetes population, ranging from 43.9% to 58% among Caucasian individuals and 29.2% to 48.1% among Asian individuals, depending on the diagnostic criteria [8]. Individuals with i-IFG exhibit a 4 to 5.5 times higher rate of progression to type 2 diabetes, depending on the diagnostic criteria, compared to those with normoglycemia [9].
Individuals with prediabetes are typically advised to adopt standard lifestyle interventions that emphasize improving diet quality with a modest calorie restriction and increasing moderate-intensity physical activity to reduce the risk of developing type 2 diabetes [10,11]. However, recent research highlights the varied effectiveness of these interventions among different prediabetes phenotypes. While these approaches prove highly effective for individuals with i-IGT and IFG plus IGT, their efficacy is notably limited for those with i-IFG [6,12,13]. Thus, there arises a necessity for alternative lifestyle intervention strategies tailored specifically to individuals with i-IFG.
One of the promising approaches is high-intensity interval training (HIIT), recognized as a time-efficient exercise option with significant benefits for metabolic health [14]. HIIT entails alternating short bursts of high-intensity exercise with periods of less active or passive recovery [15]. It is noteworthy that HIIT represents a more intensive exercise regimen compared to the current physical activity recommendations for individuals with prediabetes [10,11].
HIIT has been shown to effectively reduce hepatic insulin resistance and improve early-phase insulin secretion in individuals with type 2 diabetes [16-20], leading to significant reductions in fasting plasma glucose (FPG) levels [17,21-25]. Given that i-IFG shares these same pathophysiological defects [5-7], it is reasonable to hypothesize that HIIT could also be effective in individuals with i-IFG, as depicted in Figure 1. However, this hypothesis has yet to be tested in a randomized controlled trial (RCT). This is a critical investigation, as reducing fasting hyperglycemia is key to preventing the progression of type 2 diabetes in those with i-IFG [6,26]. To inform the design and implementation of this RCT, we propose conducting a proof-of-concept study among individuals with i-IFG, with the following objectives.
Primary objectives (feasibility and acceptability): (1) assess the feasibility of recruiting and retaining participants and executing study procedures; (2) examine the feasibility, acceptability, and appropriateness of the HIIT intervention for participants; and (3) investigate participants’ experiences, perceptions, and satisfaction with the HIIT intervention, and identify facilitators and barriers to participation.Secondary objective (preliminary efficacy): Investigate the preliminary efficacy of HIIT in reducing FPG levels and addressing the underlying pathophysiology of i-IFG.
Potential pathways through which high-intensity interval training sessions may address the pathophysiological abnormalities and fasting hyperglycemia in individuals with isolated impaired fasting glucose. VLDL: very low-density lipoprotein.
Methods
Study Design, Study Setting, and Participants
The study will be reported in accordance with the CONSORT (Consolidated Standards of Reporting Trials) guidelines for randomized pilot and feasibility trials [27]. This is a “proof-of-concept” 1:1 parallel-group RCT involving 34 physically inactive individuals aged 35-65 years who are overweight or obese and have i-IFG. Figure 2 presents the study’s CONSORT diagram. The Georgia Clinical Research Center (GCRC) at Emory University Hospital will serve as the site for participant recruitment and conducting study procedures. A highly trained and experienced study coordinator will recruit participants through a comprehensive 3-step screening procedure.
CONSORT (Consolidated Standards of Reporting Trials) flow diagram. CGM: continuous glucose monitoring; HIIT: high-intensity interval training; i-IFG: isolated impaired fasting glucose; OGTT: oral glucose tolerance test; REDCap: Research Electronic Data Capture.
Step 1: Screening (via Electronic Health Records)
Potential participants will be identified using Emory’s electronic health care records system, known as “MyChart.” Queries within this database will target individuals aged 35-65 years with a BMI≥25 kg/m^2^ (≥23 kg/m^2^ if Asian descent) [28], who have been diagnosed with prediabetes (hemoglobin A_1c_ [HbA_1c_] 5.7%-6.4%) [29] within the last 12 months, have no diagnosis of diabetes (FPG≥126 mg/dL or 2-hour plasma glucose ≥200 mg/dL or HbA_1c_≥6.5% or currently taking antidiabetic drugs) [29], not currently taking weight-loss medications, not currently taking drugs known to influence glucose tolerance (steroids and antipsychotics), not currently taking beta-blockers and calcium channel blockers (individuals taking these drugs will not reach heart rate (HR) targets for the HIIT sessions), did not undergo bariatric surgery, no anemia (anemia may limit the exercising capacity), and have no chronic illnesses (cardiovascular disease, stroke, cancers, chronic respiratory diseases, and mental health disorders). Individuals meeting these criteria will receive an invitation through the MyChart platform to participate in the second screening step.
Step 2: Screening (via Phone Calls)
Those expressing interest in participating in the study through MyChart will be contacted via phone. During these calls, individuals will receive a comprehensive explanation of the study and have any questions addressed. They will then be asked to sign an electronic consent form via Emory’s REDCap (Research Electronic Data Capture; Vanderbilt University) platform [30]. Following consent, potential participants will complete a questionnaire to assess their eligibility for step 3 screening based on the following criteria.
Physically inactive (less than 150 minutes per week of moderate-intensity physical activity, less than 75 minutes per week of vigorous-intensity physical activity, and <600 metabolic equivalent task–minutes per week) [31] assessed by the International Physical Activity Questionnaire (IPAQ) [32].Available to participate in the HIIT group sessions.No history of smoking (smoking is associated with reduced insulin secretion and increased insulin resistance) [33].Not enrolled in weight loss programs in the past 6 months.Not enrolled in any regular exercise programs in the past 6 months.Not currently following a specific diet (eg, ketogenic and Mediterranean).No plans to undergo bariatric surgery during the study period.No plans to relocate outside the study area during the study period.Not pregnant.Not breastfeeding.
Step 3: Screening (via In-Person Clinic Visits)
Individuals meeting the step 2 criteria will be invited to visit the GCRC at Emory University Hospital after fasting overnight for a minimum of 8 hours [29]. During the visit, participants will complete standard questionnaires to collect sociodemographic information (education, occupation, and marital status) [34,35] and details on alcohol consumption [34,35] and dietary intake [36]. Additionally, physical measurements will be conducted using standardized instruments in accordance with the World Health Organization’s STEPwise approach to noncommunicable disease risk factor surveillance (STEPS) protocol [37]. Following these assessments, individuals will undergo an oral glucose tolerance test (OGTT) and provide blood samples for insulin. Individuals diagnosed with i-IFG, defined by the American Diabetes Association criteria as FPG between 100-125 mg/dL and 2-hour plasma glucose<140 mg/dL [29], will be deemed eligible to participate in the study. Individuals without i-IFG will be excluded from further participation in the study. They will receive a summary report of their test results and general healthy lifestyle advice and will be referred to their general practitioner if they have IGT or undiagnosed diabetes for further management.
Randomization and Blinding
Participants will be equally randomized into either the intervention or control group after completing baseline assessments and being found eligible, using a computer-generated randomization sequence by a statistician not involved in the trial. Given the nature of the study, only specific personnel such as nursing staff, laboratory personnel, and the data analyst will be blinded to participant allocation to the study groups. Participants, the study coordinator, the HIIT intervention instructor, and the principal investigator will not be blinded to participation allocation.
Intervention
Following the recommendation of the American College of Sports Medicine [38], participants in the intervention group will be required to obtain medical clearance from their general practitioner before starting the HIIT sessions. These sessions, led by a qualified exercise physiologist (the instructor) and adhering to standard protocols [39,40], will take place in the Aerobic Exercise Laboratory at Emory University's Rehabilitation Hospital. Using “spin cycle ergometers” (Schwinn), sessions will be conducted in small groups of 5 or fewer participants at specified times on Mondays, Wednesdays, and Fridays, spanning 8 weeks. Each participant will undergo a maximum of 24 HIIT sessions. Each session will consist of a 5-minute warm-up, followed by an interval-based workout phase with steady up-tempo cadences, sprints, climbs, and interspersed recovery periods. A 5-minute cooldown will conclude each session. The workout sessions will initially last 20 minutes and will progressively increase in time based on participants’ tolerance and instructor recommendations. Each session will include “active rest” periods where resistance is reduced to lower HR, alternating with high-intensity intervals featuring sprints or climbs to elevate HR. The duration of active rest versus high-intensity intervals will be adjusted according to individual responses and target HR. To monitor and maintain intensity within the target HR range, participants will wear Polar H10 chest strap HR sensors [41]. The target HR will be calculated using the Karvonen method [42]. Exercise intensity will begin at 75% of the estimated maximum HR reserve (HRR) and will increase by 5% every week, as tolerated or deemed necessary by the instructor, over the 8-week intervention period. During the workout phase, the target HRR reserve will be maintained by averaging increases and decreases in intensity or HR with a target to maintain within a 10% offset from the HRR goal [39,40]. Participants will need to adhere to within-session HR targets at an 80% rate (or greater) for a session to be counted as attended and participants will need to attend 19 out of 24 sessions to be included as a “completer” in the final data analysis. To date, our interventions have yielded a within-session adherence rate to the prescribed intervention of 91% (as measured by HR) and a retention rate of 85% [40,43-45]. Participants’ weight and body composition will be measured weekly.
To ensure high compliance in session attendance, the instructor will hold weekly one-on-one meetings with participants to provide personalized feedback and encouragement. Participants’ HR data will also be reviewed during these meetings. Additionally, the study coordinator will remind participants of their scheduled sessions 1 day in advance through phone calls or texts. Attendance in sessions will be closely monitored, and records of attended exercise sessions will be maintained. Participants who miss sessions will be contacted via phone calls to encourage attendance.
Any adverse events occurring during or after HIIT sessions will be documented, with medical advice sought if necessary. Both intervention and control participants will receive instructions to maintain a eucaloric diet throughout the study. Dietary adherence will be monitored biweekly by a registered dietitian using the Automated Self-Administered 24-Hour Dietary Assessment Tool (National Cancer Institute) [36]. This tool will be administered via phone calls 3 times a week, covering 2 weekdays and 1 weekend day. Additionally, control participants will be instructed to refrain from engaging in intense physical activities during the study period. Physical activity adherence will be assessed biweekly using the short form of IPAQ, also administered via phone calls [32].
Procedures
The details about the measurements, study tools, and timelines are outlined in Table 1.
Study Feasibility
Table 2 shows the study feasibility metrics. Continuous data collection on feasibility parameters, such as response rate, screening yield, enrollment rate, time to enrollment, intervention compliance, resource use (cost and staff time), and retention rate, will be conducted throughout the study.
Intervention, Feasibility, Acceptability, and Appropriateness
The Feasibility of Intervention Measure (FIM) will evaluate the feasibility of the intervention, encompassing questions regarding its implementability, possibility, doability, and ease of use [46]. The acceptability of the intervention will be assessed through the Theoretical Framework of Acceptability (TFA) questionnaire, which explores affective attitude, burden, ethicality, perceived effectiveness, intervention coherence, self-efficacy, opportunity costs, and general acceptability [47]. The Intervention Appropriate Measure (IAM) will evaluate the appropriateness of the intervention, including questions about its fittingness, suitability, applicability, and alignment with participants’ needs [46]. Responses to the questions in all 3 questionnaires will be recorded on a Likert scale of 1 to 5. The mean total score for each of these scales will be calculated by combining the individual Likert points of each scale. Higher scores on the FIM, TFA, and IAM scales indicate greater feasibility, acceptability, and appropriateness, respectively, among participants.
Continuous Glucose Monitoring
By providing 288 glucose measurements per day throughout the 8-week intervention and 10-day follow-up, continuous glucose monitoring (CGM) can track the dynamic changes in fasting glucose levels induced by HIIT [48]. This can help identify when the effects of HIIT on fasting glucose levels become evident and whether these effects are sustained after the intervention, which may not be captured by a single blood glucose measurement taken after 8 weeks. All participants, regardless of their assigned treatment, will be fitted with a CGM device on their abdominal area upon enrollment. The CGM device, Dexcom G6 Pro CGM system (DexCom, Inc), will be used in blinded mode to minimize bias and ensure that it does not influence the study outcomes. Participants will be instructed to eat their last meal by 10 PM daily after the CGM fitting. They will wear CGM devices for approximately 80 days, including 10 days prior to the intervention, the 8-week intervention period, and 10 days following the intervention. Participants will be trained on how to replace the device every 10 days, using the instructions provided in the manual [49], during the first study visit. The adequacy of CGM data will be evaluated using the following criteria: a minimum of 80% of the potential 288 glucose values per day should be present for any 7 consecutive days, commencing from the day following sensor insertion [50].
Clinical Measures
Data on health behaviors, physical measurements, and biochemical measurements will be collected at both baseline and 8 weeks.
Health Behaviors
Physical activity levels will be assessed using the short form of IPAQ [32] and dietary intake with the Automated Self-Administered 24-Hour Dietary Assessment Tool questionnaire [36]. Data on smoking and alcohol use will be obtained using questions adapted from the WHO STEPS [34] and the National Health and Nutrition Examination Survey questionnaires [35].
Physical Measures
Physical measurements will be taken following standard protocols [37,51]. Height will be measured using a stadiometer (Welch Ally—Scale-Tronix) with an accuracy of 0.1 cm. Weight will be assessed using a digital weighing scale (Welch Ally—Scale-Tronix) with precision to the nearest 0.1 kg. Waist and hip circumferences will be measured using an inelastic measuring tape (BaumGartens) with a precision of 0.1 cm. Blood pressure will be measured using the DINAMAP automatic blood pressure apparatus (GE HealthCare). Body composition measures, including fat mass, muscle mass, fat-free mass, visceral adipose tissue mass, and fat percent, will be obtained using the bioimpedance analysis.
Biochemical Measures
Participants will undergo an OGTT following standard protocols [52,53]. The test will be conducted after an overnight fast of at least 10 hours, with the session scheduled between 7 and 9 AM. Venous blood samples will be collected at 0, 30, and 120 minutes after ingesting a 75-g oral glucose load dissolved in 250-300 mL of water, consumed over 5 minutes. Additionally, blood samples for insulin will be obtained at 0 and 30 minutes after glucose load ingestion. Blood samples will be processed and analyzed at the Emory Medical Laboratory (EML). EML is a fully accredited and licensed clinical laboratory, actively participating in the College of American Pathologists Laboratory Accreditation Program. Additionally, it holds Clinical Laboratory Improvement Amendments certification through the Centers for Medicare and Medicaid Services. EML is also duly licensed by the state of Georgia. Glucose levels will be assessed through enzymatic assays and insulin levels via immunoassays based on the EML protocol [53]. All these analyses will use kits provided by Beckman Coulter Inc and will be performed on a Beckman Coulter analyzer.
Indices of ß Cell Function and Insulin Resistance
Table 3 provides details on the indices of ß Cell function and insulin resistance derived from glucose and insulin levels. Early-phase insulin secretion will be assessed using the insulinogenic index [54], while total ß cell function with be evaluated with the oral disposition index [55] and homeostatic model assessment of ß cell function [56]. Whole-body insulin resistance will be determined using the Matsuda index [57] and homeostatic model assessment of insulin resistance [56], while tissue-specific insulin resistance will be assessed with the hepatic insulin resistance index [58] and muscle insulin sensitivity index [58].
Qualitative Research
Participants assigned to the intervention group will be invited to take part in in-depth interviews both before and after the HIIT intervention. Trained interviewers will administer these interviews either in person during scheduled study visits or via Zoom within 1 week of the visits if participants are unable to attend in person. The interviews will be guided by interview guides specifically developed for the study and piloted with members of the study team. Preintervention interviews will delve into participants’ prediabetes history, physical activity and dietary habits, perceptions of body size and image, as well as their comfort levels, perceived difficulty, confidence, and expectations regarding the HIIT intervention. Post-intervention interviews will focus on participants' experiences with the intervention. Every effort will be made to interview both dropouts and active participants to ensure a comprehensive understanding of program acceptability and to identify barriers and facilitators to adherence. All interviews will be audio recorded, transcribed verbatim, and deidentified for analysis.
Outcomes
Primary Outcomes
Quantitative measures: (1) feasibility metrics and (2) mean FIM, TFA, and IAM scores.
Qualitative measures: participants’ experiences, perceptions, and satisfaction with the HIIT intervention, and facilitators and barriers to participation.
Secondary Outcomes
Between-group differences in changes in the following parameters from baseline to 8 weeks: (1) mean FPG and insulin levels, (2) indices of β cell function and insulin resistance, and (3) weight, body composition, waist and hip circumferences, and blood pressure.CGM metrics: (1) between-group differences in the proportion of time and mean time spent in nocturnal (12 to 6 AM) [50] normoglycemia (60 to <100 mg/dL) during the 8-week intervention period and the 10 days following the intervention, and (2) within-participant differences in the proportion of time and mean time spent in nocturnal (12 and 6 AM) normoglycemia (60 to <100 mg/dL) between exercise and non-exercise days during the 8-week intervention period.
Data Management
The study coordinator will enter questionnaire data, as well as physical and biochemical measurements directly into Emory University’s REDCap database [30]. This database will feature validation checks to ensure data accuracy, along with skip patterns facilitated by branching logic functions. The principal investigator (ST) will constantly review the data for any errors, promptly flagging any errors for correction by the study coordinator. Upon completion of data entry and cleaning, a master copy of the data set will be generated and securely stored within the REDCap database. CGM raw data (in CSV file format per participant) will be downloaded from the DexCom Clarity software and uploaded to REDCap. Access to these datasets will be limited to the study coordinator and the principal investigator for confidentiality and data security purposes.
Sample Size Calculation
Assuming a Cohen d of 0.3 to <0.7 (medium standardized effect size) [25,59] for FPG in the planned main trial, with an alpha of 5% and a power of 90%, a sample size of 15 participants per treatment group is deemed necessary for this pilot study. Factoring in a 10% loss to follow-up in each group, the total sample size was estimated to be 34 participants (17 per group).
Statistical Analysis
Quantitative Research
Objective 1
Continuous variables will be summarized using either mean (SD) or median (IQR), depending on their distribution, which will be visually assessed through histograms. Categorical variables will be presented as counts (n) and percentages (%).
Objective 2
The analyses will adhere to the “intention-to-treat” principle. Between-group differences in changes in continuous variables from baseline to 8 weeks will be analyzed using mixed-effects linear regression models, while categorical variables will be assessed with log-binomial models. Skewed variables will be log-transformed prior to analysis. Fixed effects will include the study group (intervention vs control), timepoint (follow-up vs baseline), and the interaction between the study group and timepoint. Random effects will be specified for participants to account for the correlation between repeated measurements on the same individual. The P value for the study group-by-timepoint interaction will be used to evaluate the difference in changes between the study groups. The correlation between changes in fasting glucose levels and the indices from baseline to 8 weeks will be assessed using either Pearson or Spearman correlation coefficients, depending on the nature of the data distribution. Mixed-effects linear regression models will be used to compare CGM metrics between study groups, adjusting for baseline values. These models will also examine within-participant differences in CGM metrics between exercise and non-exercise days. Statistical significance will be considered with a 2-sided P value<.05 with no adjustments for the multiplicity of comparisons. All analyses will be conducted using Stata (version 18.0; StataCorp LLC).
Qualitative Research
In-depth interviews will be conducted with intervention group participants and dropouts. All interviews will be audio recorded and transcribed verbatim for analysis. The qualitative analysis plan involves 2 main components: a framework-driven analysis of intervention acceptability data and a thematic analysis focusing on participant expectations, experiences, barriers, and facilitators in undergoing the HIIT intervention. For the framework-driven analysis, a deductive codebook containing the TFA dimensions will be applied to both baseline and postintervention interview data. This approach aims to provide a comprehensive and longitudinal understanding of HIIT acceptability among program users, comparing results across timepoints and between those who remained in the program and study dropouts. Additionally, an inductive approach will be used to create a codebook of inductive codes around other aspects of acceptability, program barriers, facilitators, experiences, and sustainability through a close reading of the transcripts. Once the data is coded, thick descriptions of individual codes will be developed, including structured comparisons such as between baseline and postintervention interviews, program adherents and dropouts, men and women, and older and younger participants. These comparisons will guide data reporting and program adaptation for further trials, providing insights into the diverse experiences and perspectives of participants.
Challenges and Mitigation Strategies
The potential challenges that could be encountered at various stages of the study and the corresponding mitigation strategies are outlined in Table 4.
Ethical Considerations
The study protocol was approved by the institutional review board of Emory University, Atlanta, USA (MOD001-STUDY00005855). All participants will provide written informed consent prior to study participation. Participant identifiers will be kept strictly confidential in a secure REDCap database, accessible only by the principal investigator and study coordinator. Data will be deidentified before analysis. Participants will receive a US $50 gift card as compensation for their participation.
Results
Table 5 shows the study timeline. Recruitment for the study is scheduled to begin in February 2025, with follow-up expected to be completed by the end of September 2025. We plan to publish the study findings by the end of 2025.
Discussion
Expected Findings
This proof-of-concept study will generate data on the feasibility and acceptability of the HIIT intervention, as well as participants’ experiences and satisfaction levels. Additionally, the study will offer preliminary estimates on the efficacy of HIIT in reducing FPG levels and addressing the pathophysiology of i-IFG.
Strengths and Limitations
To our knowledge, this study will be the first to assess the feasibility and acceptability of a HIIT intervention exclusively among individuals with i-IFG. Additionally, we adhered to the PRISMA-P (Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols) statement [60] when reporting the details of this study protocol. However, there are some limitations. We will assess the pathophysiological abnormalities in i-IFG using indices derived from the OGTT and fasting insulin levels instead of gold-standard methods like the intravenous glucose tolerance test and glycemic clamps [61-63]. However, these indices have demonstrated strong correlations with estimates obtained from the gold-standard methods [61-63]. Additionally, our reliance on a single OGTT may be subject to day-to-day variability in glucose tolerance status. Nevertheless, strict adherence to standardized protocols for conducting the OGTT [52,53] should help minimize this variability to a significant extent.
Conclusions
The results of this study are expected to guide the design and implementation of an RCT to assess the efficacy of HIIT intervention in reducing diabetes incidence and achieving remission in individuals with i-IFG.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2019 Diabetes in the Americas Collaborators Burden of diabetes and hyperglycaemia in adults in the Americas, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet Diabetes Endocrinol 2022109655667 10.1016/S 2213-8587(22)00186-335850129 S 2213-8587(22)00186-335850129 PMC 9399220 · doi ↗ · pubmed ↗
- 2Magliano D Boyko EJIDF Diabetes Atlas 2021 Brussels, Belgium International Diabetes Federation 35914061 · pubmed ↗
- 3GBD 2019 Diabetes Air Pollution Collaborators Estimates, trends, and drivers of the global burden of type 2 diabetes attributable to PM air pollution, 1990-2019: an analysis of data from the Global Burden of Disease Study 2019 Lancet Planet Health 202267 e 586e 600 10.1016/S 2542-5196(22)00122-X 35809588 S 2542-5196(22)00122-X 35809588 PMC 9278144 · doi ↗ · pubmed ↗
- 4Cai X Zhang Y Li M Wu JH Mai L Li J Yang Y Hu Y Huang Y Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis BMJ 2020370 m 2297 10.1136/bmj.m 22973266928232669282 PMC 7362233 · doi ↗ · pubmed ↗
- 5Abdul-Ghani MA Tripathy D De Fronzo RA Contributions of beta-cell dysfunction and insulin resistance to the pathogenesis of impaired glucose tolerance and impaired fasting glucose Diabetes Care 20062951130113910.2337/diacare.29511301664465429/5/113016644654 · doi ↗ · pubmed ↗
- 6Campbell MD Sathish T Zimmet PZ Thankappan KR Oldenburg B Owens DR Shaw JE Tapp RJ Benefit of lifestyle-based T 2DM prevention is influenced by prediabetes phenotype Nat Rev Endocrinol 202016739540010.1038/s 41574-019-0316-13206041610.1038/s 41574-019-0316-132060416 · doi ↗ · pubmed ↗
- 7Nathan DM Davidson MB De Fronzo RA Heine RJ Henry RR Pratley R Zinman B Impaired fasting glucose and impaired glucose tolerance: implications for care Diabetes Care 200730375375910.2337/dc 07-99201732735530/3/75317327355 · doi ↗ · pubmed ↗
- 8Yip WCY Sequeira IR Plank LD Poppitt SD Prevalence of pre-diabetes across ethnicities: a review of impaired fasting glucose (IFG) and impaired glucose tolerance (IGT) for classification of dysglycaemia Nutrients 20179111273 10.3390/nu 911127329165385 nu 911127329165385 PMC 5707745 · doi ↗ · pubmed ↗