Comparison of Endovascular Interventions for the Treatment of Superficial Femoral Artery Disease: A Network Meta-analysis
Andrew W. Schwartz, Yousuf Shah, Haocheng Huang, Ashwin Nathan, Alexander C. Fanaroff, Jay S. Giri, Sahil A. Parikh, Alexandra J. Lansky, Tayyab Shah

TL;DR
This study compares various endovascular treatments for superficial femoral artery disease to determine their safety and effectiveness.
Contribution
The study provides a network meta-analysis comparing multiple endovascular interventions for SFA disease.
Findings
PTA alone is mostly inferior to other endovascular techniques for SFA disease.
CSG, BMS, and A+DCB showed superior technical success compared to PTA.
DCB, DES, and BMS improved Rutherford classification better than PTA.
Abstract
To understand the relative safety and efficacy of endovascular treatment modalities used for superficial femoral artery (SFA) disease, we performed a network meta-analysis to compare outcomes between percutaneous transluminal angioplasty (PTA), atherectomy (A), bare metal stent (BMS), brachytherapy/radiotherapy, covered stent graft (CSG), cutting balloon angioplasty (CBA), drug-coated balloon (DCB), drug-eluting stent (DES), and intravascular lithotripsy (L). We performed a systematic literature search of PubMed from January 2000 to January 2023 to identify randomized trials comparing endovascular interventions for the treatment of SFA disease. The primary end points were technical success and 12-month primary patency. In total, 57 studies (9089 patients) were included. The mean age of the included patients was 68.4 years, 41.4% had diabetes, 18.3% had critical limb ischemia, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
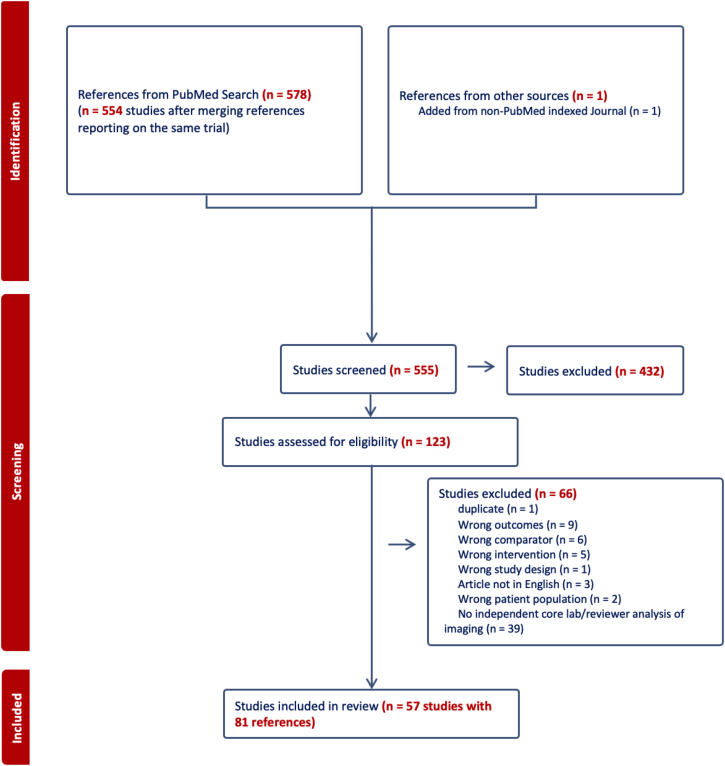 Figure 1
Figure 1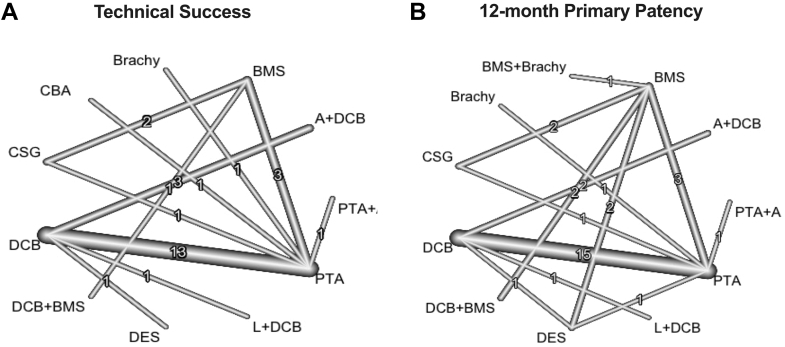 Figure 2
Figure 2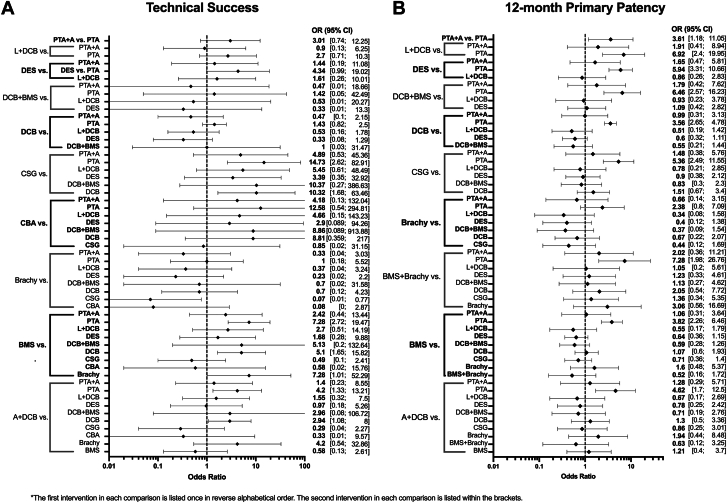 Figure 3
Figure 3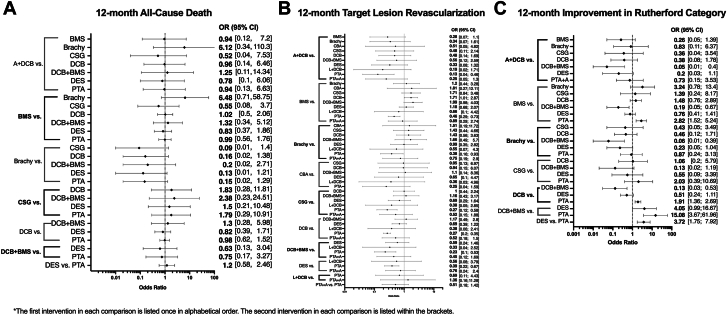 Figure 4
Figure 4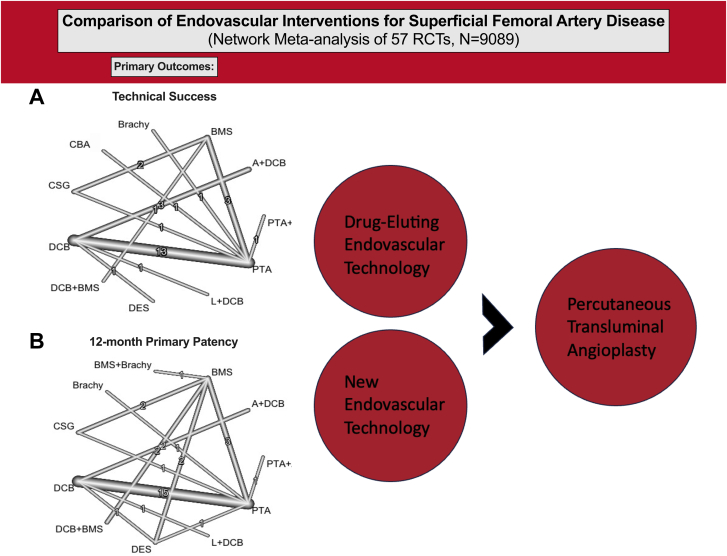 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Acute Ischemic Stroke Management · Vascular Procedures and Complications
Introduction
Peripheral arterial disease (PAD) remains a significant cause of morbidity and mortality worldwide, with increasing prevalence and associated health care costs.1^,^2 Chronic limb-threatening ischemia (CLTI), the most severe form of PAD, is associated with a significant risk of amputation and death.3 Disease of the superficial femoral artery (SFA) is the leading cause of both intermittent claudication (IC) and CLTI.4 Treatment of PAD often includes revascularization of the lower extremities, either by endovascular intervention or surgical bypass. Currently there is conflicting randomized evidence on whether surgical bypass or modern endovascular therapy is superior for various cohorts of CLTI patients.5^,^6 Regardless, endovascular revascularization of the lower extremities is indicated in many patients with SFA disease, including patients needing revascularization for IC resistant to medical management, those without adequate venous grafts, poor surgical candidates, or those who prefer a less invasive endovascular approach.7, 8, 9
The rapid growth of new endovascular therapies and new randomized controlled trials (RCTs) testing their effects in PAD patients has led to a significant amount of new data over the past decade10, 11, 12, 13; however, it remains unclear how each novel therapy should fit into real-world practice. Both the American and European guidelines highlight the lack of high quality and comprehensive evidence in this space and call for further data to be gathered.14^,^15 Thus, understanding the relative safety and efficacy of each intervention will help guide decision making in treating patients and may inform future guidelines. Thus, we conducted a network meta-analysis of RCTs to compare the safety and efficacy of endovascular treatment modalities for SFA disease.
Methods
Search strategy
We performed a network meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.16 The protocol was registered in PROSPERO (CRD42022377373). A systematic literature search of PubMed was completed including studies from January 2000 to January 2023 to identify RCTs comparing ≥2 endovascular interventions for the treatment of SFA disease that were published in the English language. The specific search terms used were (“femoral” or “femoropopliteal” or “peripheral artery”) AND (“endovascular” OR “angioplasty” OR “balloon” OR “stent” OR “atherectomy” OR “lithotripsy”). The bibliographies of relevant studies were also examined to identify other potentially relevant studies.
Inclusion/exclusion criteria
The studies were screened by 2 independent authors (A.S. and T.S.) and were included if they were RCTs that compared ≥2 endovascular interventions for the treatment of SFA disease (IC and/or CLTI) in patients aged >18 years. Studies were excluded if they did not report any of the primary or secondary outcomes of this meta-analysis or if they did not have independent core laboratory adjudication of angiographic and/or ultrasound outcomes. Studies that reported on the same trial were included and searched for relevant data and were counted as one study in total. Any discrepancy was resolved by a third reviewer (Y.S.). Endovascular interventions and their combinations included in the study were percutaneous transluminal angioplasty (PTA), percutaneous transluminal angioplasty + atherectomy (PTA+A); drug-coated balloon (DCB), lithotripsy + drug-coated balloon (L+DCB), atherectomy + drug-coated balloon (A+DCB), drug-coated balloon + bare metal stent (DCB+BMS), drug-eluting stent (DES), bare metal stent (BMS), brachytherapy/radiation therapy (brachy), bare metal stent + brachytherapy/radiation therapy (BMS+brachy), covered stent graft (CSG), and cutting balloon angioplasty (CBA).
Data extraction
For every selected study, 2 authors (A.S., T.S, and/or Y.S.) read the text and extracted study details, sample size, patient demographics and comorbidities, lesion characteristics, and procedural characteristics. Discrepancies were reviewed by the 2 reviewers to reach consensus. Claude-3-Opus (Anthropic) was used to verify data extraction, and any discrepancies were verified and corrected.
Outcomes
The primary efficacy outcome was 12-month primary patency, defined as freedom from >50% restenosis (peak systolic velocity ratio <2.5 on duplex ultrasound) of the treated lesion and freedom from target lesion revascularization (TLR). The primary procedural outcome was technical success, defined as <30% residual stenosis on immediate postintervention angiogram.
The secondary 12-month safety outcomes were major amputation, defined as any leg amputation proximal to the ankle, all-cause death, and TLR, defined as revascularization of the treated arterial segment. The secondary efficacy outcomes included primary patency at 6 months, 12-month improvement in Rutherford category by ≥1, mean change of Walking Impairment Questionnaire score, and mean change of EuroQol-5 Dimension score, which is a standardized questionnaire to measure health-related quality of life. One-month TLR, 6-month and 12-month late lumen loss, and 1-month all-cause death were prespecified secondary end points, but they were not reported due to the limited number of studies available to include in the network.
Statistical analysis
Categorical variables, such as patient demographics, are reported as percentages whereas continuous variables are reported as mean ± SD. A network meta-analysis was conducted through simultaneous analysis of direct comparisons of interventions within RCTs and indirect comparison across trials using common comparators. Heterogeneity between studies was assessed using I^2^. Random effect models were used, given the intermediate heterogeneity across trials. When available, PTA was used as a control comparator. The effect estimate for each of the outcomes is presented as an odds ratio (OR) with 95% CI. Prediction intervals were also calculated for each primary outcome. P-scores, which measure the certainty that a treatment is better than other treatments, were calculated based on meta-analytic point estimates and standard errors and used to rank order different interventions.17
Meta-regression was used to identify if effect sizes of various interventions varied by proportion of various subgroups included in the trials. Subgroups tested included age, female sex, diabetes, current smoking status, chronic kidney disease, end-stage renal disease, CLTI, total occlusions, severe calcification, and de novo lesions. Only results of DCB vs PTA meta-regressions are shown, given the limited number of studies available for other comparisons to conduct meta-regression. We did not account for multiple testing in the primary analysis because the comparisons were only hypothesis-generating and we did not expect to find significant results for most tested subgroups. As a sensitivity analysis we used the Bonferroni method to account for multiple testing.
Risk of bias
A risk of bias assessment was completed using the Cochrane Risk of Bias 2 tool.18 Each study was evaluated in 5 different categories to determine an overall risk of bias, including randomization process, deviation from the intended intervention, missing outcome data, measurement of the outcome, and selection of reported results. Publication bias was assessed by funnel plots and asymmetry tests (Egger’s test).
Results
Study selection
The search identified 555 total studies with 81 references encompassing 57 studies (9089 total patients) included in the final analysis (Figure 1).10^,^13^,^19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73 Details of all included studies are presented in Supplemental Table S1. Four of the included studies reported only on secondary outcomes for which there was not enough data to develop a network.19^,^34^,^44^,^45 The studies were found to generally be at low risk of bias (Supplemental Table S2) and there was no evidence of publication bias (Supplemental Figures S1 and S2).Figure 1PRISMA flow diagram of the network****meta-analysis.
Cohort characteristics
The baseline characteristics of the population are outlined in Table 1. Briefly, the mean age was 68.4 years, 66.7% were male, and 84.4% were White. A total of 41.4% had diabetes mellitus, 41.2% were current smokers, 68.1% had dyslipidemia, 79.3% had hypertension, and 12.8% had renal insufficiency. The mean target leg ankle–brachial index was 0.6, most patients had Rutherford Class 3 (63.1%), and 18.3% had CLTI before intervention. A mean of 1.2 lesions were treated per patient with 81.3% being de novo lesions (Table 2). There was popliteal involvement in 16.6% of lesions treated, and 35.7% of patients had chronic total occlusions. Patient characteristics by each tested endovascular intervention is available in Supplemental Table S3.Table 1. Baseline characteristics.N = 7271Age, y68.4 ± 9.0Male sex66.7%Body mass index, kg/m^2^27.3 ± 4.5Hypertension79.3%Dyslipidemia68.1%Diabetes mellitus41.4%Current smoking41.2%Heart failure5.9%Coronary artery disease42.9%Prior myocardial infarction18.5%Carotid artery disease23.0%Prior CVA (stroke/TIA)13.2%Renal insufficiency12.8%End-stage renal disease6.6%Target leg ankle–brachial index0.6 ± 0.2Rutherford class 14.8% 225.0% 363.1% 49.0% 58.3% 61.1%Chronic limb-threatening ischemia (Rutherford 4-6)18.3%Prior interventions46.6% Percutaneous transluminal angioplasty16.8% Drug-coated balloon1.6% Stent39.4% Atherectomy2.8%N = average number of patients with data available from total of 9089. Values are mean ± SD or %.CVA, cerebrovascular accident; TIA, transient ischemic attack.Table 2. Lesion and procedural characteristics.Lesion characteristicsN = 7480 No. of lesions treated1.2 ± 0.9 De novo lesions81.3% In-stent restenosis18.0% No. of patient runoff vessels 08.6% 121.2% 237.3% 340.1% Popliteal involvement16.6% Lesion length, cm9.3 ± 5.3 Total occlusion35.7% Diameter stenosis at baseline, %81.7 ± 13.6 Calcification None33.8% Mild/moderate46.4% Severe21.3%Procedural characteristicsN = 6526 Procedure time, min64.7 ± 32.7 No. of treatment balloons1.3 ± 0.4 Procedural complication Any dissection38.6% Flow-limiting dissection (≥ type D)5.2% Thrombus3.0% Aneurysm/pseudoaneurysm1.9% Perforation0.8% Distal embolus1.6% Diameter stenosis after intervention, %22.4 ± 11.0N = average number of lesions or patients with relevant data available from total of 9089. Values are mean ± SD or %.
Primary end points
Network plots are shown in Figure 2. There were 37 total studies including 5765 patients that assessed technical success among 11 endovascular treatments (Figure 3A).10^,^12^,^13^,^21, 22, 23, 24^,^28, 29, 30, 31^,^33^,^36^,^38^,^40^,^43^,^46, 47, 48, 49, 50, 51, 52, 53^,^58, 59, 60, 61, 62, 63, 64^,^66^,^68, 69, 70^,^72^,^73 There was no significant heterogeneity across trials (I^2^ = 35.9%; 95% CI, 0.0%-63.1%). Technical success was superior for CSG (OR, 14.73), BMS (OR, 7.28), and A+DCB (OR, 4.2) compared with PTA, whereas A+DCB (OR, 2.94) and CSG (OR, 10.32) were superior to DCB, and BMS (OR, 7.28) was superior to brachy. Technical success ranked highest for CSG (0.88) based on P-scores; the remaining rankings are detailed in Table 3.Figure 2Network plots for primary outcomes. Line thickness is weight by amount of randomized controlled trials used to compare the 2 groups by outcome. (A) Technical success; (B) primary patency.Figure 3Primary outcomes of the network meta-analysis. (A) Technical success; (B) primary patency at 12 months. Endovascular interventions with their comparators are on the left of the y-axis, with corresponding odds ratio (OR) with 95% CI displayed on the right. A, atherectomy; BMS, bare metal stent; brachy, brachytherapy; CBA, cutting balloon angioplasty; CSG, covered stent graft; DCB, drug-coated balloon; DES, drug-eluting stent; L, lithotripsy; PTA, percutaneous transluminal angioplasty.Table 3. Ranked P-scores for primary and secondary outcomes.Endovascular interventionPrimary patency 12 moTechnical successTarget lesion revascularization 12 moRutherford improvement 12 moMajor amputation 12 moAll-cause death 12 moWIQ score change 12 moEQ-5D score change 12 moBMS+brachy0.75–––––––L+DCB0.740.470.27–––––DCB+BMS0.730.340.740.990.20.59––DES0.710.610.440.780.620.33––CSG0.630.880.660.51–0.25––A+DCB0.540.610.890.17–0.48–0.55PTA+A0.420.500.33––0.46––BMS0.390.760.330.660.590.47––DCB0.350.250.680.490.530.490.930.65Brachy0.240.190.460.2––––PTA0.010.120.050.20.550.460.060.29CBA–0.740.63–––––Ranked P-scores for primary and secondary outcomes. P-scores indicate the certainty an intervention is superior than other interventions for the outcome.A, atherectomy; BMS, bare metal stent; brachy, brachytherapy; CBA, cutting balloon angioplasty; CSG, covered stent graft; DCB, drug-coated balloon; DES, drug-eluting stent; EQ-5D, EuroQol 5-Dimension; L, lithotripsy; PTA, percutaneous transluminal angioplasty; WIQ, Walking Impairment Questionnaire.
A total of 33 studies including 5907 patients that evaluated 11 different endovascular treatments assessed 12-month primary patency (Figure 3B).10^,^13^,^20, 21, 22, 23^,^25^,^26^,^28^,^30^,^31^,^33^,^36^,^38^,^43^,^47^,^48^,^50^,^51^,^56, 57, 58, 59, 60^,^62, 63, 64, 65, 66^,^68^,^71, 72, 73 There was significant heterogeneity across trials (I^2^ = 57.6%; 95% CI, 33.2%-73.0%). Primary patency was superior for L+DCB (OR, 6.92), DES (OR, 5.94), DCB+BMS (OR, 6.46), DCB (OR, 3.65), CSG (OR, 5.36), BMS+brachy (OR, 7.28), BMS (OR, 3.82), and A+DCB (OR, 4.62) compared with PTA. BMS+brachy (0.75), L+DCB (0.74), DCB+BMS (0.73), and DES (0.71) ranked highest by P-scores (Table 3). Results were similar for 6-month primary patency (Supplemental Figure S3A). Prediction intervals for primary end points, using PTA as a common comparator, showed similar trends to CIs and are available in Supplemental Table S4.
Secondary end points
Network plots are shown in Supplemental Figure S4. A total of 37 studies including 6556 patients assessed 12-month mortality for 9 endovascular interventions.12^,^23, 24, 25, 26^,^28, 29, 30, 31, 32, 33^,^35, 36, 37^,^42^,^47, 48, 49, 50, 51, 52^,^56^,^57^,^59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71^,^73 Mortality (Figure 4A) and 12-month major amputation (Supplementary Figure S3B) were not different across treatments.Figure 4Secondary outcomes of the network meta-analysis. (A) All-cause death at 12 months; (B) target lesion revascularization at 12 months; (C) improvement in Rutherford category at 12 months. Endovascular interventions with their comparators are on the left of the y-axis, with corresponding odds ratio (OR) with 95% CI displayed on the right. A, atherectomy; BMS, bare metal stent; Brachy, brachytherapy; CBA, cutting balloon angioplasty; CSG, covered stent graft; DCB, drug-coated balloon; DES, drug-eluting stent; L, lithotripsy; PTA, percutaneous transluminal angioplasty.
A total of 49 total studies including 7801 patients assessed 12-month TLR for 11 endovascular interventions.10^,^12^,^13^,^21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31^,^33^,^35, 36, 37, 38^,^41, 42, 43^,^46, 47, 48, 49, 50, 51, 52^,^54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73 There was significant heterogeneity across trials (I^2^ = 44.5%; 95% CI, 18.9%-62.0%). A+DCB (OR, 0.13), BMS (OR, 0.46), brachy (OR, 0.38), CSG (OR, 0.27), DCB (OR, 0.27), DCB+BMS (OR, 0.23), and DES (OR, 0.39) were superior to PTA. BMS (OR, 1.71) was inferior to DCB (Figure 4B). When ranked, A+DCB had the highest P-score (0.89) (Table 3).
A total of 18 studies including 2885 patients assessed improvement in Rutherford classification at 12 months for 7 endovascular interventions.25^,^26^,^30^,^31^,^35^,^36^,^40^,^47^,^49^,^50^,^57^,^58^,^60^,^61^,^63^,^65^,^67^,^70 There was no significant heterogeneity across trials (I^2^ = 26.2%; 95% CI, 0.0%-62.6%). BMS (OR, 2.82), DCB (OR, 1.91), DCB+BMS (OR, 15.08), and DES (OR, 3.72) all significantly improved Rutherford classification compared with PTA. DCB+BMS was superior to A+DCB (OR, 0.05), BMS (OR, 0.19), brachy (OR, 0.06), and DCB (OR, 0.13) (Figure 4C). When ranked, DCB+BMS had the highest P-score (0.99) (Table 3).
A limited number of trials assessed 12-month changes in EuroQol-5 Dimension and Walking Impairment Questionnaire scores. Although point estimates favored DCB over PTA, they were not significant.
Meta-regression analysis
Based on meta-regression, trials comparing DCB vs PTA with a higher proportion of de novo lesions (P < .0001), female patients (P = .04), and severely calcified lesions (P = .03) had greater effect size for DCBs improving Rutherford category. Trials with a higher proportion of de novo lesions (P = .014) had greater effect size favoring DCBs for 12-month TLR. Trials with a higher proportion of chronic total occlusions (P = .008) had greater 12-month mortality in the DCB arms (Supplementary Table S5). When accounting for multiple testing, only effect modification of de novo lesions remained significant.
Discussion
This network meta-analysis, based on rigorously conducted contemporary RCTs with independent and core laboratory adjudication of end points, provides up to date, comprehensive and clinically relevant insights into the relative safety and efficacy of the numerous endovascular devices available to treat SFA disease in primarily IC patients. Technical success was highest for CSG, BMS, and A+DCB, and 12-month primary patency was superior for virtually all newer endovascular interventions compared with PTA (Central Illustration). Therapies with improved primary patency compared to PTA were also associated with more frequent improvement in symptoms, with DCB+BMS being particularly highly ranked for 12-month improvement in Rutherford classification. The 12-month mortality and major amputation rates were similar between treatments, although these comparisons were limited by the small number of studies included and low event rates (considering most were IC patients who generally have lower rates of these events than CLTI patients). Comparisons of changes in Walking Impairment Questionnaire and EuroQol-5 Dimension were also limited by number of studies, although their point estimates favored DCB over PTA.Central IllustrationPrimary end points network plots of (A) technical success and (B) 12-month primary patency. A, atherectomy; BMS, bare metal stent; brachy, brachytherapy; CBA, cutting balloon angioplasty; CSG, covered stent graft; DCB, drug-coated balloon; DES, drug-eluting stent; L, lithotripsy; PTA, percutaneous transluminal angioplasty; RCT, randomized controlled trial.
Our results are consistent with findings of previous meta-analyses that demonstrate that PTA alone for SFA lesions is inferior to other endovascular options in primary patency and technical success.74^,^75 Our meta-analysis also confirmed that these findings were consistent among trials including patients with in-stent restenosis, which was not previously evaluated. It also showed that PTA was inferior to other interventions, including DCBs, in symptom improvement. This is not surprising because negative remodeling and neointimal hyperplasia following PTA are mitigated by therapies such as stents and DCBs.76, 77, 78 This adds to the growing evidence that a PTA-alone strategy for SFA disease is insufficient79 for most lesions despite it being used in up to 30% of cases.5^,^80 Although PTA alone may have been overused in the past due to the now discredited link between paclitaxel and increased mortality,81, 82, 83 these results highlight the benefit of drug-eluting therapy.
This study addresses, in part, the gap in knowledge regarding device selection in femoropopliteal disease identified by previous guidelines.9^,^15 Both documents give relatively little guidance on device selection and only give weak recommendations for newer therapies relative to PTA and only when PTA gives a suboptimal result. Our study shows that technical success is superior with the use of newer endovascular therapies as a first-line strategy. Additionally, 12-month primary patency and even more importantly, patient symptoms, are also improved when newer endovascular therapies are used as a first-line strategy. As drug-eluting therapies including DCBs continue to become standard of care for these patients, the comparisons presented here using DCB as the comparator will provide valuable insight for device selection in modern practice.
Highly calcified SFA lesions are difficult to treat due to decreased vessel compliance, increased risk of dissection with balloon expansion, and decreased delivery of drug therapy.84 Currently, the mainstay therapy for highly calcified lesions includes vessel preparation strategies with intravascular L and A, often followed by PTA or DCB.30^,^85^,^86 Our analysis suggests both are viable options, particularly when paired with DCBs, given that L+DCB and A+DCB were highly ranked for 12-month primary patency. However, given the limited number of studies including these interventions, this result should be interpreted with caution.
Subgroup analyses by meta-regression suggested that patients with de novo lesions had greater benefit from DCB for symptom improvement and TLR compared with those with in-stent restenosis. It is well established that DCBs are superior to PTA alone in patients with in-stent restenosis49^,^50^,^52; however, this study demonstrates that the benefit is less strong than in de novo lesions. There is abundant evidence that DCBs are superior for heavily calcified lesions59^,^87 and for women,88 which are both supported by our meta-regression analysis as well. Although our meta-regression analysis suggested there may be increased mortality with DCBs in trials that enrolled more patients with total occlusions, this does not have a physiologic basis and, as mentioned above, this association has been repeatedly debunked. More likely this finding was the result of type I error from multiple testing as evidenced by all meta-regressions, besides those looking at de novo lesions, no longer being significant after adjusting P values for multiple testing.
Limitations
This study has several limitations. First, this is a post hoc analysis of trial-level data; therefore, these results are only hypothesis-generating. For many comparisons there was significant heterogeneity across trials, likely reflecting the varying patient/lesion selection in the trials for different devices, which may affect the interpretability of the results, particularly for interventions used in vastly different patient populations. However, in most cases, heterogeneity was at most moderate89 and was explained by differences in baseline characteristics identified by meta-regression including lesion calcification and in-stent restenosis lesions. Additionally, many outcomes and interventions had few, if any, studies contributing to the network, limiting many comparisons and making the results susceptible to selection bias based on which studies reported which outcomes. Finally, the cohort had a male predominance, which limits the generalizability of the results to the broader population, although this is a limitation in trial enrollment and not one specifically of this meta-analysis.
Conclusion
This network meta-analysis supports the benefit of new endovascular therapies, including drug-eluting therapy, for the treatment of SFA disease compared with PTA alone. Future studies focused on device selection in SFA disease are warranted.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nehler M.R.Duval S.Diao L.Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population J Vasc Surg 6032014686695.e 22482090010.1016/j.jvs.2014.03.290 · doi ↗ · pubmed ↗
- 2Mahoney E.M.Wang K.Keo H.H.Vascular hospitalization rates and costs in patients with peripheral artery disease in the United States Circ Cardiovasc Qual Outcomes 3620106426512094024910.1161/CIRCOUTCOMES.109.930735 · doi ↗ · pubmed ↗
- 3Conte M.S.Bradbury A.W.Kolh P.Global vascular guidelines on the management of chronic limb-threatening ischemia Eur J Vasc Endovasc Surg 581S 2019 S 1S 109.e 333118233410.1016/j.ejvs.2019.05.006PMC 8369495 · doi ↗ · pubmed ↗
- 4Poredos P.Cevc M.Blinc A.Characteristics of atherosclerosis in femoropopliteal artery and its clinical relevance Atherosclerosis 335202131403454758810.1016/j.atherosclerosis.2021.09.012 · doi ↗ · pubmed ↗
- 5Farber A.Menard M.T.Conte M.S.Surgery or endovascular therapy for chronic limb-threatening ischemia N Engl J Med 387252022230523163634217310.1056/NEJ Moa 2207899 · doi ↗ · pubmed ↗
- 6Bradbury A.W.Moakes C.A.Popplewell M.A vein bypass first versus a best endovascular treatment first revascularisation strategy for patients with chronic limb threatening ischaemia who required an infra-popliteal, with or without an additional more proximal infra-inguinal revascularisation procedure to restore limb perfusion (BASIL-2): an open-label, randomised, multicentre, phase 3 trial Lancet 401103902023179818093711652410.1016/S 0140-6736(23)00462-2 · doi ↗ · pubmed ↗
- 7Primary Panel Abramson B.L.Al-Omran M.Canadian Cardiovascular Society 2022 guidelines for peripheral arterial disease Can J Cardiol 38520225605873553781310.1016/j.cjca.2022.02.029 · doi ↗ · pubmed ↗
- 8Foley K.M.Kennedy K.F.Lima F.V.Treatment variability among patients hospitalized for chronic limb-threatening ischemia: an analysis of the 2016 to 2018 US National Inpatient Sample J Am Heart Assoc 1332024 e 03089910.1161/JAHA.123.030899 PMC 1105616838240207 · doi ↗ · pubmed ↗