Beyond urodynamics: non-invasive approaches to diagnosing detrusor underactivity in men with lower urinary tract symptoms – a systematic review
Karolina Garbas, Łukasz Zapała, Aleksander Ślusarczyk, Hanna Piekarczyk, Tomasz Piecha, Piotr Radziszewski

TL;DR
This systematic review evaluates non-invasive methods for diagnosing detrusor underactivity in men with urinary symptoms, finding varying diagnostic accuracy.
Contribution
The study systematically reviews and compares non-invasive diagnostic methods for detrusor underactivity, highlighting their feasibility and diagnostic accuracy.
Findings
The DUA-SQ questionnaire showed the highest sensitivity (95.8%) for diagnosing detrusor underactivity.
Ultrasound measurements had 100% specificity but low sensitivity (42%) for detrusor underactivity.
AI models demonstrated potential with sensitivities ranging from 65.9% to 79.7%.
Abstract
To evaluate and synthesize existing evidence on non-invasive methods for diagnosing detrusor underactivity (DU) in men presenting with lower urinary tract symptoms (LUTS), focusing on their feasibility and diagnostic accuracy. A systematic search of PubMed, Scopus, and Web of Science databases was conducted for original articles reporting on non-invasive diagnostic tests for DU in men with LUTS. Data extraction focuses on study characteristics, diagnostic methods, and accuracy. The risk of bias was assessed using the QUADAS-2 tool. Eighteen studies involving 7390 patients, of whom 3194 were diagnosed with DU, were included in our analysis. The evaluated diagnostic methods included ultrasound parameters, biomarkers, uroflowmetry results, symptom questionnaires, and clinical characteristics. Developed models, including those based on artificial intelligence (AI), and nomograms were also…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
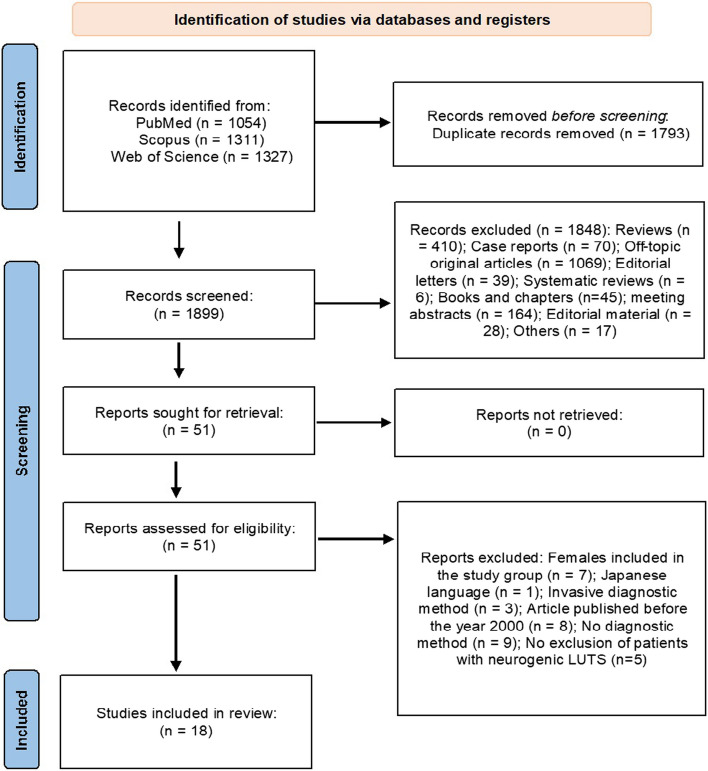 Figure 1
Figure 1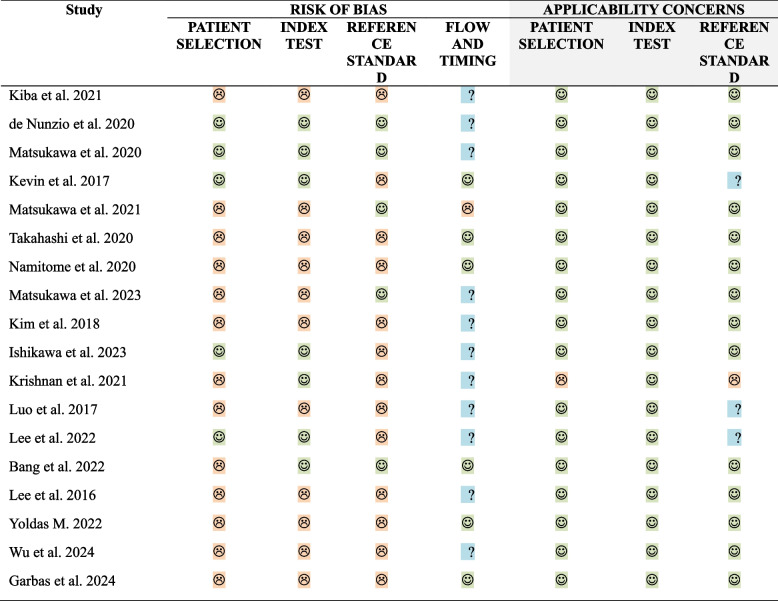 Figure 2
Figure 2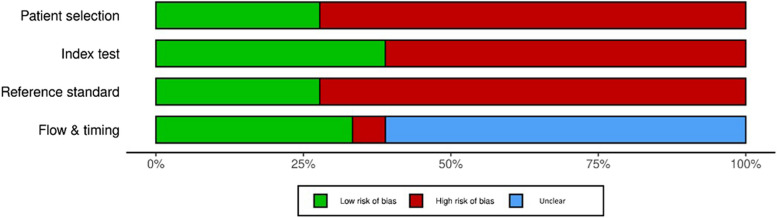 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Bladder and Prostate Research · Pelvic floor disorders treatments · Urinary and Genital Oncology Studies
Background
Detrusor underactivity (DU) has recently gained attention as a significant phenomenon among patients with lower urinary tract symptoms (LUTS). However, despite its growing recognition, the medical condition still lacks a standardized definition and universally accepted diagnostic criteria [1]. The International Continence Society (ICS) defined DU as “a contraction of reduced strength and/or duration, resulting in prolonged bladder emptying and/or failure to achieve complete bladder emptying within a normal time span” [2]. Recently, D’Ancona et al. revised this definition and described DU as “low detrusor pressure or short detrusor contraction time, usually in combination with a low urine flow rate resulting in prolonged bladder emptying and/or a failure to achieve complete bladder emptying within a normal time span” [3].
A separate term, “underactive bladder” (UAB), has been introduced to describe the symptoms associated with DU [4]. Nevertheless, defining UAB is challenging due to its lack of specific symptoms and frequent overlap with those of overactive bladder (OAB) and bladder outlet obstruction (BOO), which makes the diagnosis especially challenging [5]. DU can, thus, present as a wide array of LUTS, including urgency, frequency, and nocturia in the storage phase, as well as hesitancy, weak or interrupted stream, straining to void, and a feeling of incomplete emptying during the voiding phase [6].
The prevalence of DU is estimated to range from 9 to 23% in men under 50 years old, increasing to approximately 48% in men over 70 years old. In older women, the prevalence is estimated to be between 12 and 45% [6]. However, accurately determining prevalence remains difficult due to the absence of widely accepted non-invasive diagnostic methods [5].
The current gold-standard for diagnosing DU, proposed by the ICS, is invasive urodynamics (UDS), which includes cystometry followed by a pressure-flow study (PFS) [7]. However, for an extended period of time, the ICS did not specify exact thresholds for diagnosing DU or define a normal bladder emptying time, leading to unstandardized diagnostic criteria [8]. One of the most commonly used criteria for men in both clinical practice and research is the Bladder Contractility Index (BCI), introduced by Abrams et al. in 1999 [9]. The BCI is calculated using the formula BCI = Pdet@Qmax + 5Qmax, which in turn provides a quick and easily applicable assessment of detrusor contractility. A BCI below 100 suggests DU, a BCI between 100 and 150 is considered normal, and a BCI greater than 150 indicates the presence of strong detrusor [9].
In 2023, the ICS and the Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) recommended adopting the BCI under the new term “Detrusor Contraction Index” (ICS-DCI), retaining the same formula for use in clinical practice, scientific analyses and cohort reporting [10]. The working group replaced the terms “contractility” with “contraction” and “bladder” with “detrusor,” and advised using ICS-DCI as a continuous scale to grade detrusor voiding contraction (DVC). They suggested the clinical classes “normal DVC” and “weak DVC”, while also recognizing “strong DVC” and “very weak DVC” for specific sub-cohorts (male patients). Although the group proposed a nomogram (the ICS-PFS plot nomogram) with a recommended cutoff at DCI = 100 to differentiate normal from weak DVC, it also called for further studies on the provisional cutoffs of DCI = 50 (very weak) and DCI = 150 (strong) [10].
In addition to the lack of standardized diagnostic criteria, invasive PFS are usually time-consuming, and may pose a risk of infectious complications in predisposed individuals, while at the same time are not widely accessible due to relatively high costs and the need for highly trained urodynamics specialists. Thus, patients are often reluctant to undergo these invasive procedures because of the associated discomfort and above-mentioned potential risk of infection. Consequently, there has been a growing interest in developing new non-invasive diagnostic methods, including uroflowmetry (UFL) analysis [11, 12], bladder wall thickness (BWT) or detrusor muscle thickness (DMT) measurement via ultrasound [13, 14], use of artificial intelligence (AI) [15, 16] and potential biomarkers in blood serum [17] or urine [18].
Consequently, the aim of our study was to assess the diagnostic value and feasibility of emerging non-invasive tests for diagnosing DU in men with LUTS compared to the invasive gold-standard PFS.
Methods
Search strategy
Our study protocol was registered with PROSPERO (CRD42024556425).
A systematic literature review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement to identify all scientific studies investigating a non-invasive diagnostic method for DU in men with non-neurogenic LUTS.
The Population, Intervention, Control, Outcome (PICO) framework was used to specify the review question. The following inclusion criteria were considered for evaluation:
- Type of study and study population (P): We included only full-text original studies in English language, published after the year 2000, covering a non-invasive diagnostic method for DU. Non-invasive method meant no need for performing an invasive PFS. The study population consisted of adult men (≥ 18 years old) with non-neurogenic LUTS. We excluded studies that included females in the study group or patients with neurogenic bladder or any diagnosed neurologic disease that could account for neurogenic LUTS.
- Index test (I): Index tests included any type of non-invasive tests or predictors used for the diagnosis of DU.
- Reference standard (C): In all studies, the reference standard used for the diagnosis of DU must have included PFS (conventional, video, or ambulatory urodynamics).
- Outcome (O): The accuracy of the non-invasive methods was reported using sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and overall accuracy for the diagnosis of DU.
We searched Medline (PubMed), Scopus and Web of Science databases in June 2024 for all relevant publications to date using the following terms: (“underactive bladder” OR “detrusor underactivity” OR “impaired detrusor contractility” OR “acontractile detrusor” OR “underactive detrusor” OR “detrusor failure” OR “detrusor areflexia”).
Data selection
Abstracts of all identified studies after exclusion of duplicates (n = 1899, see Fig. 1 for details) were independently reviewed and screened for eligibility by two authors (KG, ŁZ). Further selected original studies reporting on non-invasive diagnostic methods for DU were reviewed in full text (n = 51). Disagreements between individual judgements, when present, were referred to the third reviewer (TP), and the final decision was made based on the majority vote of the three reviewers. Finally, we decided to include 18 studies in our review. Studies were only included in our systematic review, if they were original studies in English language with full-text available and they covered any type of non-invasive tests used for the diagnosis of DU or DU predictors in men with non-neurogenic LUTS. Data from the eligible reports and their supplementary data files were extracted by two reviewers independently (KG, HP). Any discrepancies were resolved through consensus among the authors.Fig. 1. Flowchart for study selection process using Medline, Web of Science and Scopus databases to identify the original articles investigating a non-invasive diagnostic method for DU in men with non-neurogenic LUTS
Studies that utilized invasive methods, specifically those diagnosing DU through UDS, were excluded [19–21]. Nevertheless, we opted to include two studies [13, 14] that involved cystometry to standardize the level of bladder filling. In these studies, the DMT/BWT ratio and BWT were measured with the use of ultrasound. Our rationale for including these studies was that, despite the invasive nature of cystometry used for standardizing the measurement conditions, the method itself employed ultrasound, which could be used non-invasively in clinical practice. Patients could achieve an appropriate bladder filling by drinking a precise amount of fluids before the test. Studies in which the exclusion criteria did not precisely mention neurogenic bladder or a diagnosed neurogenic disease were excluded [22–26]. We also excluded studies performed before the year 2000, as we found the data outdated in comparison to the most up-to-date knowledge about DU.
Data display
All data extracted from the studies were systematically organized and presented using tables to ensure clarity and facilitate comparison across studies. Descriptive statistics, including means, medians, percentages, and ranges were displayed where applicable. When presenting the accuracy of the examined methods, sensitivity, specificity and prevalence were used to calculate missing NPV and PPV values, where available.
Risk of bias assessment
We used the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) Critical Appraisal Tool to evaluate the methodological quality and risk of bias in the retrieved studies [27]. Two authors (KG and HP) individually and independently assessed all the studies based on the QUADAS-2 criteria, and any potential disagreements were resolved via consensus between those two authors. In the index test domain, the risk of bias was deemed “low” when the physicians interpreting the test were blinded to the reference standard results, and when the measurement methods were consistent across all patients (e.g., all measurements were performed using abdominal ultrasound). For the reference standard domain, the risk of bias was deemed “low” if the PFS was conducted according to ICS Standards by a physician blinded to the index test results, if both DU and non-DU patients underwent the reference standard, and if the diagnosis of DU was based on BCI and BOOI values. The risk of bias in the flow and timing domain was considered “low” when patient flow was clearly documented, all patients included in the study were included in the analysis, and all received the same reference standard. Regarding applicability concerns, most studies were assessed as having “low” concerns, with some exceptions. The reference standard domain was classified as “unclear” when diagnostic criteria other than BCI/BOOI were used to diagnose DU. The QUADAS-2 template for tabular display was employed to visualize the risk of bias and applicability [28] and the Robvis tool was utilized to create a summary plot of the risk of bias of all included studies [29].
Results
Characteristics of included studies
This systematic review included 18 studies with a total of 7390 patients, of whom 3194 were diagnosed with DU.
The review comprised 18 observational studies, including cross-sectional studies (n = 17) and a case–control study (n = 1). The studies were conducted across multiple geographic regions, with a majority from Asia (n = 13), followed by Europe (n = 3), Turkey (n = 1) and India (n = 1). The publication dates ranged from 2016 to 2024 (see Table 1 for details). Table 1. Characteristics of the studies included in the systematic reviewNoStudyDOICountryStudy designDates of analysed dataInclusion criteriaExclusion criteria1Kiba et al. 2022 [ 30]10.1111/luts.12424Japanretrospective cross-sectional studyJanuary 2013—October 2020men ≥ 50 years without neurogenic disorders with DU or BOOneither DU nor BOO, surgery for BPH, conditions known to cause neurogenic bladder dysfunction (neurological disease, spinal disease, cerebrovascular infarction, or cerebral hemorrhage), PCa, BCa, incomplete data2De Nunzio et al. 2020 [14]10.1002/nau.24327Italyprospectively recruited, retrospective cross-sectional studyJanuary 1996—December 2000males, ≥ 45 years old, LUTS, informed consentneurological disorders, renal insufficiency, bladder stones, PCa, urethral stricture, previous pelvic surgery, taking α‐blockers and 5‐α reductase inhibitors3Matsukawa et al. 2020 [11]10.1111/iju.14121Japanprospectively recruited, retrospective cross-sectional study2010–2017male patients, total IPSS ≥ 8, IPSS-QOL ≥ 3, PV ≥ 20 mL in transabdominal US and age ≥ 45 yearspharmacotherapy for LUTS, bladder calculi, active UTI, suspected of conditions known to cause neurogenic bladder dysfunction (severe diabetes mellitus, neurological disease, history of pelvic surgery, spinal disease, cerebrovascular infarction or cerebral hemorrhage), incomplete data4Rademakers et al. (FORCE Research Group) 2017 [31]10.1007/s00345-016–1902-7the Netherlands, Germanyprospectively recruited, retrospective cross-sectional study1 January 2000—31 December 2001treatment-naïve men ≥ 40 years with clinical BPH, LUTS, and/or PV > 25 ml and able to void without previous medical or surgical therapies for LUTSα-blockers, 5α-reductase inhibitors, urinary retention, prior LUT or pelvic surgery, evident PCa or BCa, or a neurologic deficit5Matsukawa et al. 2021 [16]10.1111/iju.14661Japanretrospective cross-sectional studyJanuary 2015 to December 2018male patients, total IPSS of ≥ 8, IPSS-QOL of ≥ 3 and age of ≥ 45 yearsprior LUTS pharmacotherapy, bladder calculi, active UTI or suspected neurogenic bladder dysfunction due to severe DM, neurological disease, history of pelvic surgery, spinal disease, cerebrovascular infarction or cerebral hemorrhage6Takahashi et al. 2021 [32]10.1002/nau.24558Japanretrospective cross-sectional studyJanuary 2010—January 2017male LUTS patients who underwent PFSpatients < 50 years, duplicates, with history of BPH surgery, neurogenic bladder, PCa, IC, BCa, bladder stones, and others affecting LUT, without full PFS data because of urinary retention or minimal VV (< 50 ml), without the data: IPSS, UFL, PVR, and PV; with DO on PFS7Namitome et al. 2020 [33]10.1097/JU.0000000000000616Japanretrospective cross-sectional studyJanuary 2010—January 2017male patients with LUTS, ≥ 50 years oldprevious BPH surgery, neurogenic bladder, PCa, IC, BCa, bladder stones, bladder neck contracture, chronic prostatitis, urethral stricture, urinary retention, < 50 ml on PFS, no full data8Matsukawa et al. 2023 [34]10.1080/13685538.2018.1481941Japanretrospective cross-sectional studySeptember 2018—December 2021men with non-neurogenic LUTS who underwent UFL and PFStotal voided and residual urine volumes in UFL < 100 mL9Kim et al. 2019 [ 35]10.1080/13685538.2018.1481941Korearetrospective cross-sectional study2000 – 2016male patients who underwent UDSDO in UDS, acute urinary retention, neurogenic problems including stroke, Parkinson’s disease, spinal cord injury, and acute UTI; low BCI and a high BOOI, suggesting simultaneous DU and BOO10Ishikawa et al. 2023 [17]10.1007/s00345-023–04341-yJapanprospective cross-sectional studyApril 2018—December 2020treatment-naïve men aged ≥ 65 years with non-neurogenic LUTSoral treatment for LUTS, neurogenic bladder dysfunction, bladder calculi, active UTI; severe cardiac disease (NYHA ≥ grade 2), hepatic dysfunction (AST and ALT levels > 2 × the normal values); renal dysfunction (serum creatinine ≥ 2.0 mg/dL); treatment for cancer at the time of study entry, receiving thiazolidinedione derivatives for DM11Krishnan et al. 2021 [18]10.1007/s00345-021–03784-5Indiaprospective case–control studyJune 2017—November 2018cases: male patients aged 18–70 years with LUTS and PVR of > 150 ml; controls: healthy age- and sex-matched volunteers without any LUTS (zero IPSS Score)cases: neurogenic bladder dysfunction, medications affecting bladder contractility such as anticholinergics, antipsychotics, opioids or beta-3 agonists; controls: serum creatinine > 2 mg/dl, prolonged use of urethral catheter, active UTI12Luo et al. 2017 [36]10.1007/s11255-017–1539-5Chinaretrospective cross-sectional studyJanuary 2013—June 2016adult men with BPH/LUTSneurogenic bladder with a confirmed etiology, such as pelvic trauma; previous medical or surgical therapies for BPH/LUTS13Lee et al. 2022 [13]10.1038/s41598-022–09302-wKoreaprospectively recruited, retrospective cross-sectional studyDecember 2017—October 2019male patients ≥ 40 years scheduled for UDS due to LUTS/BPH refractory to medical treatments for > 3 monthsmedical conditions affecting bladder function and/or structural deformation including neurological disorders of parkinsonism, stroke, MS, urethral stricture, bladder diverticulum, bladder stone, previous BPH or pelvic surgery, and PCa; patients with complications of Clavien–Dindo grading 3 or higher after prostate surgery14Bang et al. 2022 [15]10.4111/icu.20210434Korearetrospective cross-sectional studyDecember 2006—Decemer 2017males, ≥ 40 years old, who underwent PFSdiseases affecting LUT function, BCa, PCa, previous prostate, bladder, and/or urethral surgeries, indwelling catheters (or needing regular catheterization), history of cerebrovascular accident, neurologic disorders, and spinal or pelvic bone trauma, < 150 mL voided on UFL, insufficient UFL study graphs for analysis15Lee et al. 2016 [12]10.4111/icu.2016.57.6.437Korearetrospective cross-sectional study2008—2014men > 50 years old who visited outpatient department complaining of weak stream, hesitation, intermittent urination and residual urine sense, with IPPS ≥ 8 points, normal serum PSA < 3.5 ng/dL, no hematuria or pyuria and no α-blocker, anticholinergics or beta-agonists for min. 8 weeks before evaluationcentral or peripheral neurogenic disease including cerebral vascular accident and spinal cord disease, histories of urinary tract abnormalities or lithiasis, surgeries of the pelvic floor or bladder, chronic pelvic pain, cardiovascular disease, patients unable to complete UDS, other UDS criteria than: DU: BCI < 100 cmH2O with BOOI; < 20 cmH2O, and BOO: BOOI ≥ 40 cmH2O16Yoldas 2022 [37]10.4081/aiua.2022.1.51Turkeyretrospective cross-sectional studyJanuary 2007—January 2015males with min. 2 UFLs (and ≥ 150 ml on UFL) and PVR measurementsfemales, urological malignancies, calculi in the bladder and lower end of the ureter, infection and asymptomatic bacteriuria, transurethral intervention history, neurogenic disease, indwelling catheter or CIC, bedridden patients, missing data17Wu et al. 2024 [38]10.22514/jomh.2024.031Chinaretrospective cross-sectional studyJanuary 2018—October 2023BPH/LUTS patients, informed consent form, 18—100 years old; conscious, compliant, ability to express feelings and independently complete symptom questionnaire; diagnosis made through physical examinations, PV measurement by abdominal US and UDS; DU defined with the PIP < 100PV > 50 mL; history of prostate surgery, prostate biopsy, medication (antimuscarinic, beta3 agonists, α1-antagonists, 5α-reductase inhibitor, intravesical injection of Botulinum Neurotoxin A and hyaluronic acid), acute and chronic prostatitis; urethral stricture, radical pelvic surgery, neurologic disease, OAB, urinary incontinence, DM and no other periferic neurologic condition to explain DU (Tarlov cyst, severe lumbar hernia, pelvic trauma)18Garbas et al. 2024 [39]10.1007/s11255-024–04093-7Polandretrospective cross-sectional study2012 – 2022male gender, age > 18 years old, LUTS, final diagnosis of DU or BOO in PFS, UFL performed immediately prior to undergoing PFS, VV on UFL > 150 ml, informed consentneurogenic bladder (any history of neurologic disease), chronic prostatitis, IC, BCa, PCa, bladder stones, prior BPH surgery, incomplete dataBCI bladder contractility index, BCa bladder cancer, BOO bladder outlet obstruction, BOOI bladder outlet obstruction index, BPH benign prostatic hyperplasia, CIC Clean Intermittent Catheterization, DM diabetes mellitus, DO detrusor overactivity, DU detrusor underactivity, IC Interstitial cystitis, IPSS International Prostate Symptom Score, IPSS-QOL International Prostate Symptom Score Quality of Life, LUT lower urinary tract, LUTS lower urinary tract symptoms, MS multiple sclerosis, OAB overactive bladder, PCa prostate cancer, PFS pressure flow study, PIP projected isovolumetric pressure, PSA prostate specific antigen, PV prostate volume, PVR post-void residual, UDS urodynamic study, UFL uroflowmetry, US ultrasound, UTI urinary tract infection
Sample sizes varied from 44 to 1792 participants, with a median sample size of 252. All studies exclusively involved male patients, with a mean or median age over 50 years. The studies addressed diverse populations, including study groups with pure DU (n = 17) and comparator groups consisting of individuals without DU (n = 11), DU combined with BOO (n = 1), BOO alone (n = 4), or healthy controls (n = 1). One study included two separate analyses: one compared a DU group with a DU + BOO + and BOO group, while the other compared DU + BOO + to both DU and BOO groups [16]. Baseline characteristics of patients are presented in Table 2. Table 2. Baseline characteristics of patients included in the studies. Values are presented as mean +—SD, unless indicated as median (Q1-Q3)NoStudySample size (n)DU groupComparator groupDU (n)Comparator (n)Age (DU)Age (comparator)Medication (DU)Medication (comparator)Comorbidities (DU)Comorbidities (comparator)1Kiba et al. 2022 [30]205pure DUDU + BOO + , BOO63DU + BOO + 48; pure BOO 9473.9 + -6.7DU + BOO + 71.2 ± 7.1; pure BOO 71.6 ± 6.4α-1 blocker 47 (75%); Tadalafil 17 (27%); Dutasteride 16 (25%); Anticholinergic agent or beta-3 adrenergic agonist 5 (8%)DU + BOO + : α-1 blocker 42 (86%); Tadalafil 7 (15%); Dutasteride 25 (52%); Anticholinergic agent orbeta-3 adrenergic agonist 5 (10%); BOO + : α-1 blocker 82 (87%), Tadalafil 18 (19%), Dutasteride 42 (45%), Anticholinergic agent or beta-3 adrenergic agonist 18 (19%)DM: 7 (11%)DU + BOO + : DM- 5 (10%), pure BOO: DM- 15 (16%)2De Nunzio et al. 2020 [14]448DUnon-DU19425467.6 ± 7.567.8 ± 8.1no α‐blockers and 5‐α reductase inhibitorsno α‐blockers and 5‐α reductase inhibitors3Matsukawa et al. 2020 [11]418DUBOO14527369.5 + -9.969.7 + -7.1no LUTS pharmacotherapyno LUTS pharmacotherapy4Rademakers et al. (FORCE Research Group) 2017 [31]143DUnon-DU33110median 62 (59–73)median 62 (57–68)no LUTS pharmacotherapyno LUTS pharmacotherapy5Matsukawa et al. 2021 [16]264DUBOO, DU + BOO + 8118370.1 + -8.8BOO 68.9 + -7.2; DU + BOO 71.4 + -8.3no LUTS pharmacotherapyno LUTS pharmacotherapyMatsukawa et al. 2021 [16]DU + BOO + DU, BOO6519971.4 + -8.3BOO 68.9 + -7.2; DU 70.1 + -8.8no LUTS pharmacotherapyno LUTS pharmacotherapy6Takahashi et al. 20210 [32]909DUnon-DU45445571.7 + -8.669.4 + -7.67Namitome et al. 2020 [33]909DUnon-DU454455of the whole cohort: some patients with LUTS refractory to medicationof the whole cohort: some patients with LUTS refractory to medication8Matsukawa et al. 2023 [34]266DUnon-DU (BOO group, DU + BOO group, and non-DU + non-BOO group)7019669.8 + -8.770.2 + -7.99Kim et al. 2019 [35]318pure DUpure BOO16515367 + -8.865 + -15.110Ishikawa et al. 2023 [17]118DUnon-DU3979median 76 (68–81)median 76 (68–81)no α1-blockers, phosphodiesterase type 5 inhibitors, 5α-reductase inhibitors, anticholinergic agents, β3-adrenergic receptor agonists or thiazolidinedione derivatives for DMno α1-blockers, phosphodiesterase type 5 inhibitors, 5α-reductase inhibitors, anticholinergic agents, β3-adrenergic receptor agonists or thiazolidinedione derivatives for DMHTN: 27, HL: 28, DM: 7HTN: 51, HL: 49, DM: 2111Krishnan et al. 2021 [18]44DUhealthy controls261856.7 + -16.752.3 + -14.9no medications affecting bladder contractility (anticholinergics, antipsychotics, opioids or beta-3 agonists)DM: 4, BOO: 812Luo et al. 2017 [36]704DUnon-DU11259270.3 + -8.469.6 + -7.8no LUTS pharmacotherapyno LUTS pharmacotherapyHTN: 53, DM: 11, MI: 21, stroke: 19HTN: 230, DM: 100, MI: 120, stroke: 9913Lee et al. 2022 [13]94DUnon-DU2470median 73 (70.5–75.5)median 71 (66–74)LUTS treatment > 3 monthsLUTS treatment > 3 months14Bang et al. 2022 [15]1792pure DUnon-DU89389964.9364.3915Lee et al. 2016 [12]240DUBOO11112968.01 + -9.7468.39 + -9.29no LUTS pharmacotherapy for min. 8 weeks prior to UDSno LUTS pharmacotherapy for min. 8 weeks prior to UDS16Yoldas 2022 [37]93pure DUpure BOO444978.54 + -11.664.18 + -11.1drugs affecting LUTS stopped 3 days prior to UDSdrugs affecting LUTS stopped 3 days prior to UDS17Wu et al. 2024 [38]196DUnon-DU9310370.7 ± 6.967.6 ± 7.4no antimuscarinic, beta3 agonists, α1-antagonists, 5α-reductase inhibitorno antimuscarinic, beta3 agonists, α1-antagonists, 5α-reductase inhibitorHTN: 38, DM: 12, Cardiovascular Disease: 19, Bladder stone: 10, Hyperlipidemia: 38HTN: 32, DM: 10, Cardiovascular Disease: 13, Bladder stone: 14, Hyperlipidemia: 4018Garbas et al. 2024 [39]229DUnon-DU128101median 61.5 (49–69.5)median 63 (52–70)cholinolitycs: 17, α-blockers: 36, insulin: 3, oral drugs for DM: 4, statins: 6cholinolitycs: 6, α-blockers: 52, insulin: 3, oral drugs for DM: 12, statins: 4DM: 12, hypothyroidism: 6DM: 16, hypothyroidism: 5BOO bladder outlet obstruction, DM diabetes mellitus, DU detrusor underactivity, HL hyperlipidemia, HTN hypertension, LUTS lower urinary tract symptoms, MI myocardial infarction, UDS urodynamic study
BCI data were available in 11 studies for both DU and comparator groups and in one study for the DU group only. BOOI data were available in 13 studies. Other UDS data were less commonly reported, with Pdet@Qmax available in 9 studies, Qmax in both DU and comparator groups in 8 studies, and in 1 study for the DU group only. Pdetmax data were reported in only 2 studies (see Table 3 for details). Table 3UDS characteristics of the patients included in the studies. Values are presented as mean +—SD, unless indicated as median (Q1-Q3)NoStudyUDS criteria for DU diagnosisUDS criteria for comparator group diagnosisPdet@Qmax (DU group)Pdet@Qmax (comparatorgroup)Qmax_ PFS(DU group)Qmax_PFS (comparator group)Pdetmax (DU group)Pdetmax (comparator group)BCI (DU group)BCI (comparator group)BOOI (DU group)BOOI (comparator group)1Kiba et al. 2022 [30]BCI < 100 and BOOI < 40DU + BOO group: BCI < 100 and BOOI ≥ 40; pure BOO group: BCI ≥ 100 and BOOI ≥ 4035.3 ± 12.1DU + BOO + : 66.1 ± 12.3, pure BOO: 98.3 ± 25.47.0 ± 2.7DU + BOO + 4.1 ± 1.8; pure BOO: 5.4 ± 2.570.4 ± 19.5DU + BOO + : 86.5 ± 9.7; pure BOO: 125.4 ± 22.521.2 ± 12.4DU + BOO + : 57.9 ± 14.8, pure BOO: 87.5 ± 28.12De Nunzio et al. 2020 [14]BCI < 100BCI > 10042 ± 1667 ± 316.1 ± 3.19.2 ± 5.278.8 ± 13.6130 ± 2528 ± 2043 ± 403Matsukawa et al. 2020 [11]BCI ≤ 100 and BOOI ≤ 40BCI 100 and BOOI > 4073.1 ± 19.0127.4 ± 20.626.8 ± 9.273.2 ± 25.84Rademakers et al. (FORCE Research Group) 2017 [31]by exclusion: patients with PVR > 30 ml but without BOO or dysfunctional voiding in PFSmedian 27.2 (19.8–39.8)median 58.2 (45.6–76.6)median 15.6 (5.2–27.2)median 39.2 (22.9–63.1)5Matsukawa et al. 2021 [16]BCI ≤ 100 and BOOI ≤ 40BOO: BCI > 100 and BOOI > 40DU: 68.8 ± 18.3BOO: 121 ± 22; BOO + DU: 84.9 ± 9.1DU: 27.1 ± 9.8BOO: 67.8 ± 21.5; BOO + DU: 51.6 ± 8.0Matsukawa et al. 2021 [16]BCI ≤ 100 and BOOI > 40BOO: BCI > 100 and BOOI > 40, DU: BCI ≤ 100 and BOOI ≤ 40DU + BOO + : 84.9 ± 9.1BOO: 121 ± 22; DU: 68.8 ± 18.3DU + BOO + : 51.6 ± 8.0BOO: 67.8 ± 21.5, DU: 27.1 ± 9.86Takahashi et al. 2021 [32]BCI < 100 and BOOI ≤ 40BOO: BOOI > 40 and BCI ≥ 1007Namitome et al. 2020 [33]BCI < 100BOO: BOOI > 408Matsukawa et al. 2023 [34]BCI < 100 and BOOI < 40BOO: (BCI ≥ 100, BOOI ≥ 40), DU + BOO: (BCI < 100, BOOI ≥ 40), and non-DU + non-BOO: (BCI ≥ 100, BOOI < 40)68.6 ± 19.2BOO: 128.4 ± 20.1; DU + BOO: 86.4 ± 11.0, non-DU nonBOO: 120.0 ± 16.426.0 ± 9.3BOO: 70.8 ± 23.9, DU + BOO + : 53.7 ± 9.4, non-BOOnonDU: 26.4 ± 13.59Kim et al. 2019 [35]BCI < 100BOOI > 4060.4 ± 30.7121.9 ± 32.413 ± 13.463.7 ± 34.510Ishikawa et al. 2023 [17]BCI < 100 and BOOI < 40DO: uninhibited detrusor contraction with an increasing amplitude of ≥ 10 cm H20 during the filling phasemedian 7 (4–8)median 7 (6–11)median 71 (60–78.5)median 113 (99–126.5)median 27 (24.5–32)median 51 (40–72.5)11Krishnan et al. 2021 [18]BCI < 100, no DO on UDSage and sex-matched healthy persons (no UDS)32.3 ± 21.94.0 ± 3.257.9 ± 27.612Luo et al. 2017 [36]Pdet.max < 50 cmH2O33.45 ± 14.1597.81 ± 37.313Lee et al. 2022 [13]BCI < 100, BVE < 90% and BOOI < 40BOO: BOOI > 4035.8 ± 6.767.3 ± 26.28.3 ± 4.19.1 ± 4.369.1 ± 21.0100.1 ± 29.722.7 ± 6.352.8 ± 28.314Bang et al. 2022 [15]BCI < 100BOO: BOOI > 4011 .0914.6778.38127.6626.2233.0115Lee et al. 2016 [12]BCI < 100 and BOOI < 20BOO: BOOI ≥ 4013.6 ± 0.734.7 ± 1.215.3 ± 16.556.4 ± 16.816Yoldas 2022 [37]BCI < 100 and BOOI > 40BCI > 100 and BOOI > 4034.1 ± 21.31101.1 ± 40.024.2 ± 3.966.5 ± 3.9848.8 ± 27.21132.5 ± 37.8320.0 ± 8.8288.0 ± 40.6917Wu et al. 2024 [38]PIP < 10032.7 ± 7.849.3 ± 11.64.4 ± 1.213.0 ± 3.018Garbas et al. 2024 [39]BCI < 100BOO: BOOI > 40median 37 (20–51)median 80 (70–93)median 6.6 (4.5–8.8)median 8.1 (6.6–11.1)median 46.5 (29–58.5)median 101 (84–123)median 78.5 (57.8–88)median 124.5 (112.5–141.5)median 22 (7.5–40.6)median 64.6 (52.6–80.8)BCI bladder contractility index, BOO bladder outlet obstruction, BOOI bladder outlet obstruction index, DO detrusor overactivity, DU detrusor underactivity, PFS pressure flow study, PIP projected isovolumetric pressure, PVR post-void residual, UDS urodynamic study, BVE bladder voiding efficiency
Three studies employed diagnostic criteria for DU that differed from the commonly used BCI and/or BOOI. One study defined DU by exclusion, identifying DU patients with PVR > 30 ml but without BOO or dysfunctional voiding in PFS [31]. Another study defined DU as Pdet.max < 50 cmH2O on PFS [36]. A third study used a combination of criteria: BCI < 100, BOOI < 40, and bladder voiding efficiency (BVE) < 90% [13]. Medication potentially affecting detrusor function was specified in 14 studies. Studies included patients without LUTS therapy (n = 8), LUTS therapy was stopped 8 weeks prior to UDS (n = 1) or 3 days prior to UDS (n = 1) or patients were on constant medication (n = 4). One study included patients with LUTS refractory to medication, without detailing their current medication intake, and one study included healthy controls without LUTS or medication. Comorbidities were reported in only 6 studies, with the most prevalent being hypertension (HTN) and diabetes mellitus (DM) (see Table 2 for details).
The investigated non-invasive diagnostic methods
Diagnostic methods, their descriptions, sensitivity, and specificity were demonstrated in Table 4. Table 4. Characteristics of the non-invasive diagnostic methodsNoStudyDiagnostic methodMeasurement methodThreshold/cut-off valueSensitivitySpecificityPPVNPVAccuracy (other)Subgroup analysisFeasibility of the methodLimitations of the study1Kiba et al. 2022 [30]Smaller PVPV: 39 ml = 75%67%50.2%85.8%no1. Retrospective study. 2.Severe cases included. 3. The BCI and BOOI criteria used for DU diagnosis. 4. 13% of patients had DM2De Nunzio et al. 2020 [14]visual nomogram including: Age, PV, BWT and Qmax on UFLBWT was measured on the bladder filled to 150 mL, with suprapubic US using the 3.5 MHz convex probe, in the horizontal direction at maximum magnification. PV was measured with transrectal US using the ellipsoid formula (p/6 width height depth of prostate). Analysis of UFL (Qmax) and clinical data (age)ex. score of 14 corresponds to 70% probability of DUAUC = 0.82; net benefit in the range of probabilities between 10 and 80%;severe LUTS group: AUC = 0.841. Useful for identifying patients at high risk of DU who should undergo PFS. 2. Patients at low risk of DU could be spared of an invasive test. 3. Could be used in neurological patients (after an external validation)1. A retrospective study (data collected prospectively) 2. Applicable to males with LUTS, a small prostate nonreceiving medical treatments 3. A small percentage of patients with severe LUTS (30%)3Matsukawa et al. 2020 [11]presence of "sawtooth and interrupted" waveform on UFLWhen the flow curve showed an interrupted shape with ≥ 3 discrete peaks, as well as with a repeated decrease of urine flow to zero followed by an increase, during micturitionyes vs no80%87.2%76.8%89.2%noUseful, high-integrity factor to predict DU1. A retrospective study 2. Difficulty evaluating flow pattern 3. DU defined as BCI < 100 and BOOI < 40, however, the prevalence of DU was reported to be different according to other diagnostic criteria based on a urodynamic measurelower IPPIPP = the vertical distance from the tip of the protrusion to the circumference of the bladder at the base of the prostate gland using transabdominal US longitudinal imaging with a bladder urine volume of approximately 150–200 mL8.2 mm77%73%60.2%85.8%nolower BVE70%66%57%45.1%76.1%no4Rademakers et al. (FORCE Research Group) 2017 [31]DWT on US in combination with BCUS DWT measurements were taken at the anterior bladder wall with a 7.5 MHz US array and bladder filling ≥ 250 ml. A mean of three DWT measurements was used for the analysis. BC = [VV + PVR] on UFLDWT ≤ 1.23 mm with BC > 445 ml42%100%100%85%accuracy of 87%, a likelihood ratio of a positive test result (DU) of 42, and a likelihood ratio of a negative test result (no-DU) of 0.58noPatients with DU could be identified with the two non-invasive parameters and without urodynamic investigation1. A retrospective study. 2. Small group of patients. 3. Only applicable for male adult male patients (no females, no children with PVR)5Matsukawa et al. 2021 [16]AI based model (for DU diagnosis)Model established using tenfold stratified crossvalidation and data augmentation79.7%88.7%75.9%90.7%accuracy of 84%noThe AI system could diagnose LUTD by calculating BCI and BOOI directly from the UFL waveform and could diagnose DU + BOO1. The AI system did not learn normal patient waveforms. 2 Insufficient evaluation of reproducibility in the same person. 3. Women not analyzedAI based model(for DU + BOO + diagnosis)50.8%83.2%49.7%83.8%diagnostic predictive value = 50.8%no6Takahashi et al. 2021 [32]3-parameters nomogram composed of: 1) IPSS Q4, 2) PV 3) age; 1 point for each factorPV measured by transrectal or abdominal US; IPSS questionnaire and clinical data analysis (age) ≥ 74 years old, PV ≤ 34.8, and IPSS Q4 ≤ 1probability of DU in patients with 3 significant factors- 77%, with 2 factors- 67%, with 1 factor- 54%, with 0 factors- 24%noSelected three factors could be useful for differentiating DU from BOO1. A retrospective study 2. Excluded patients with urinary retention and those who could not void > 50 ml in a PFS 3. PV was evaluated using transrectal or abdominal ultrasonography (variability) 5. Even if all three factors are present, 34% of patients still have BOO and 23% of patients still do not have DU. 6. Among non‐DU patients with all three factors, 76% of the patients had a BCI ≤ 120 (borderline DU)7Namitome et al. 2020 [33]5-parameter scoring model, including: 1) age, 2) PV, 3) IPSSQ4, 4) IPSSQ5, 5) Qmax on UFL;PV was measured by transrectal or abdominal US; IPSS questionnaire, UFL analysis, clinical data analysis (age);1) Age 50–74- 0points, > = 75—2 points; 2) PV: < 30 ml- 5 points, > = 30 and < 50- 2 points, > = 50 ml 0 points; 3) I-PSS Q4 < = 2—1 point, 4) I-PSS Q5 > 2- 1 point; 5) Qmax on UFL- < = 5- 2points, > 5 and < = 10 0 1 point, > 10- 0 pointsc-index: 0.724; points and predicted probability of DU: 0 points- 12%; 11 points- 88%,noThe study included patients with BOO and DO, which is important as DU, BOO and DO often overlap clinically1. No external validation. 2. The effect of medications not considered. 3. Excluded patients with urinary retention or those who could not void > 50 ml in the PFS8Matsukawa et al. 2023 [34]AI-developed UFL-based parameter: 1) lower first peak flow rateThe first peak flow: the point in the voiding wave shape at which the subsequent urine flow rate decreases. Even if the gradient of the urine waveform decreased, it was not judged as the first peak flow unless the gradient was negative6.5 mL/s72%86%64.7%89.6%AUC = 0.82noThe first peak flow can be easily assessed in clinical practice1. Study required 0.1-s interval measurements of the UFL waveforms. 2. A retrospective study. 3. DU was defined as BCI < 100 and BOOI < 40. 4. The first peak flow parameters may not be useful, when VV is too low (< 50 mL). 5. Difficult to diagnose the severity of DU or exactly distinguish DU from BOO + DUAI-developed UFL-based parameter: 2) lower ratio of the first peak flow rate to QmaxCalculated as the first peak flow rate/Qmax0.876%83%61.6%90.6%AUC = 0.85no9Kim et al. 20198 [35]Higher score in DUA-SQ: 8-questions questionnaire based on symptoms8 parameters to assess; each scored 0,5,10 or 15 points45 points95.8%95.4%95.8%95.4%AUC = 0.99no1. A retrospective study 2.Difficult to detect patients who overlap with DU and BOO (designed for the differential diagnosis)10Ishikawa et al. 2023 [17]Lower total serum adiponectin levelTotal serum adiponectin levels were measured using a particle-enhanced turbidimetric immunoassay at a commercial laboratory using a latex bead-immobilized anti-adiponectin polyclonal antibody7.9 μg/mL79%90%79.6%89.7%AUC = 0.85noAdiponectin can be easily measured with good reproducibility1. Other factors associated with lifestyle-related diseases and MetS not evaluated. 2. A control group of healthy participants or a patients with different BMI and lifestyle-related diseases not included 3.Patients taking anticholinergic drugs, statins and anti-inflammatory drugs not excluded 4. DU defined as a BCI < 100 and a BOOI < 40 and most patients had 20 < BOOI < 40. 5. Some patients in the non-DU group with BOOI > 40 but BCI < 100 6. A cross-sectional study11Krishnan et al. 2021 [18]Higher NO/ATP ratio in urine samplesELISA kits were used to estimate NO and ATP levels from urine2.0688.5%88.9%92.0%84.2%accuracy of 88.6%, AUC = 0.91noSpot urinary levels of NO and ATP might help reach a diagnosis of DU for indeterminate urodynamic findings or help completely avoid UDS1. Small sample size 2. DU of different etiologies 3. Control subjects labeled as usual based on history- the UDS was not performed 4. DU defined with BCI < 10012Luo et al. 2017 [36]Smaller PV combined with higher PVRPV and PVR were measured using abdominal US. Prolate ellipsoid formula (volume = π/6 × length × width × height) was used to obtain the PVPV = 46.05 ml and PVR = 147 ml77.8%73.7%35.8%94.6%AUC = 0.77no1. Not all clinical determinants of DU assessed. 2. Only Pdet. max used as the criterion for DU. 3. The threshold of Qmax might be inaccurate as a result of the low values. 4. Small sample size 5. Results based on Asian men13Lee et al. 2022 [13]Smaller ratio of DMT and BWT = (DMT/BWT × 100) %US measurements of the DMT and BWT were performed every 50 mL during filling in a cystometric study up to 500 mL or MCC. DMT and BWT were measured at the anterior wall of the bladder with the patient in the supine position < 47.5% of the thickness ratio at 20% of the MCC86.7%64.3%45.4%93.4%AUC = 0.76noThe thickness ratio remained relatively constant up to 50% of the MCC; thus, measuring the thickness ratio < 50% of the MCC would be more accurate and convenient1. Small number of DU patients 2. The age of the two control groups not matched 3. Difficult to repeat bladder filling for patients diagnosed with DU due to UDS invasiveness 4. Operator-dependent 5. Measuring DMT and BWT by US is challenging below 50% of the MCC14Bang et al. 2022 [15]Deep learning-based diagnostic platform based on UFL graphs analysisUFL graph was extracted automatically using the ABBYY Flexicapture® image capture program. A convolutional neural network (CNN) was applied. A fivefold cross-validation average value of the AUROC curve was chosen as an evaluation metric. The corresponding average precision-recall (PR) curves were provided. The average AUROC scores of DUA were measured using fivefold cross-validation and the best score was obtained with fine-tuned VGG16 network65.9%68.9%67.9%67.0%AUROC score = 73.30% (mAP = 0.70)no1. Low prediction rate (over 70%). 2. The capacity to set the basis for model predictions confined due to the absence of external data. 3. Excluded patients with both BOO and DU15Lee et al. 2016 [12]Smaller DeltaQ = (Qmax—Qmean) on UFLUFL analysis6.65 mL/s71.3%70.3%67.5%74.0%AUC = 0.81no1. A retrospective study. 2. Only patients with DU or BOO, men with mixed urodynamic problems were excluded. 3. Possibly other conditions affect DeltaQ. 5. UDS interpreted by a single urologist. 6. A single institution studySmaller Qmax on UFLUFL analysis11.05 mL/s69%68.5%65.3%71.9%AUC = 0.7616Yoldas 2022 [37]Higher BVE on UFL (for men > 80 years old)BVE = VV on UFL/pre-void BC measured on US46%93%60%67.6%90.5%AUC of max. diagnostic value for VE = 0.771yes; age > 80 years oldApplicable for men over 80 years old1. The BOOI 20–40 not examined. 2. A cut-off of 40 for AG-number used17Wu et al. 2024 [38]Older age66.5 years72%46%54.6%64.5%AUC = 0.71no1. Limited number of participants. 2. Incomplete incorporation of inflammation markers. 3. The hematological markers oversimplified and did not provide accurate representation of patient’s conditionLower PSA level2.90 ng/mL30%49%34.7%43.7%AUC = 0.3718Garbas et al. 2024 [39]10-factor model, including nocturia, intermittency, weak stream, straining points in CLSS, slow stream points in CLSS, incomplete emptying points in CLSS, PVR ratio, and fluctuating, fuctuating-intermittent and intermittent UFL curve shapesmedical history, CLSS questionnaire, interpretation of UFL, including curve shape analysis75.8%62.4%71.9%67.0%C-index: 0.783noCan be useful during the initial ambulatory visit1. A retrospective study 2. Excluded patients who could not void > 150 ml on UFL, including those with urinary retention 3. A single geographic and ethnic population study, performed on white Polish males 5. PV not evaluated 6. Some patients on medication affecting voidingAI* artificial intelligence, AUC area under the curve, AUROC area under the receiver operating characteristic curve, BC bladder capacity, BCI bladder contractility index, BMI body mass index, BOO bladder outlet obstruction, BOOI bladder outlet obstruction index, BE bladder voiding efficiency, BWT bladder wall thickness, CLSS core lower urinary tract symptom score, DM diabetes mellitus, DWT detrusor wall thickness, DO detrusor overactivity, DU detrusor underactivity, DUASQ detrusor underactivity symptom questionnaire, IPP intravesical prostatic protrusion, IPSS International Prostate Symptom Score, LUTD lower urinary tract dysfunction, LUTS lower urinary tract symptoms, MCC maximal cystometric capacity, PFS pressure flow study, PSA prostate specific antigen, PSAD prostate-specific antigen density, PV prostate volume, PVR post-void residua, UDS urodynamic study, UFL uroflowmetry, US ultrasound, VV voided volume
Nomograms and scoring models
Five studies developed and applied nomograms or scoring models for DU diagnosis, comparing patients with DU to non-DU individuals. One study introduced a visual nomogram combining age, prostate volume (PV), bladder wall thickness (BWT) measured via ultrasound, and maximum flow rate (Qmax) on UFL. This model demonstrated a 70% predictive probability of DU for patients scoring 14 points, which increased to approximately 93% when the total score reached 16 points [14]. Another study used a three-parameter nomogram composed of International Prostate Symptom Score (IPSS) question 4 (Q4), PV and age. A patient aged 74 or older, with a PV of 34.8 ml or less and an IPSS Q4 score of 1 or lower, scored 3 points in the nomogram, which corresponded to a 77% probability of DU [32]. Namitome et al. developed a five-parameter scoring model that incorporated age, PV, IPSS Q4 and Q5, and Qmax on UFL. In this model, scores of 1, 2, or 5 were assigned to each variable. For example, a 75-year-old male patient (2 points) with an IPSS Q4 score of 2 (1 point), an IPSS Q5 score of 3 (1 point), a PV of 30 ml (2 points) and a Qmax on UFL of 5 ml/sec (2 points) would have a total score of 8 points, corresponding to 72% probability of DU [33]. One study employed a nomogram based on PV and PVR, achieving 77% sensitivity and 73% specificity for DU diagnosis [36]. Another study developed a 10-factor model that incorporated symptoms, the Core Lower Urinary Tract Symptoms score (CLSS), PVR ratio (calculated as the percentage of PVR to bladder volume [voided volume + PVR]), and UFL curve shapes. The ten factors included nocturia, intermittency, weak stream, straining points in CLSS, slow stream points in CLSS, incomplete emptying points in CLSS, PVR ratio, and fluctuating, fluctuating-intermittent and intermittent UFL curve shapes. This model demonstrated sensitivity of 75.8%, similar to the abovementioned models, but had a lower specificity of 62.4% [39].
UFL analysis
Four studies utilized various UFL parameters as a diagnostic method for DU. One study investigated the presence of "sawtooth" and "interrupted" waveforms on UFL, characterized by an interrupted flow curve with three or more discrete peaks, as well as repeated decrease in urine flow to zero followed by an increase, during micturition. This method achieved a sensitivity of 80% and a specificity of 87.2%, for differentiating DU from BOO patients. Additionally, the study assessed bladder voiding efficiency (BVE), defined as the ratio between voided volume and total bladder capacity [9]. However, it performed worse, with a sensitivity of 66% and specificity of 57% [11]. Another study also evaluated the utility of BVE, showing that DU could be diagnosed with a 93% sensitivity and a 60% specificity in men over 80 years old, with UFL measurements indicating voiding efficiency higher than 46% [37]. Lee et al. tested a DeltaQ parameter, calculated as Qmax – Qmean on UFL. The area under the curve (AUC) for DeltaQ (0.806) was significantly higher than that from Qmax (0.763) and Qmean (0.574). With a cutoff value of 6.65 mL/s, it had a sensitivity of 71.3% and specificity of 70.3% [12]. Qmax was also evaluated in another study, showing a sensitivity of over 80% and specificity of 63%. However, it performed worse than the combined PV and PVR for predicting DU [36].
Ultrasound parameters
Three studies focused on ultrasound parameters. Two investigated detrusor wall thickness (DWT), bladder wall thickness (BWT), or their derivatives, and one assessed intravesical prostatic protrusion (IPP). The FORCE Research Group evaluated DWT in combination with bladder capacity (BC) as a method for diagnosing DU. DWT measurements were taken at the anterior bladder wall, using a 7.5 MHz ultrasound array with the bladder filled to over 250 mL. A mean of three DWT measurements was used for the analysis. BC was calculated as BC = [voided volume + PVR)] on UFL. A DWT of 1.23 mm or less, combined with BC of over 445 mL demonstrated a 100% specificity for DU diagnosis but had poor sensitivity of only 42% [31]. In contrast, Lee et al. studied the ratio of detrusor muscle thickness (DMT) to BWT, calculated as (DMT/BWT × 100) %, which showed better sensitivity but lower specificity. A thickness ratio of less than 47.5%, measured at 20% of the maximal cystometric capacity (MCC), provided a sensitivity of over 86% and a specificity of approximately 64%. In this study, ultrasound measurements of the DMT and BWT were performed every 50 mL during filling in a cystometric study up to 500 mL or MCC. Both DMT and BWT were measured at the anterior wall of the bladder with the patient in the supine position. BWT was defined as the width of the bladder wall, including the two thin hyperechoic layers of the mucosa, while DMT was specified as the width of the hypoechoic space, excluding the hyperechoic layers [13]. The third study investigated IPP, which was calculated as the vertical distance from the tip of the protrusion to the circumference of the bladder at the base of the prostate gland, using transabdominal ultrasonographic longitudinal imaging, with a bladder urine volume of approximately 150–200 mL. In this study, IPP had a significant correlation with BCI and was a useful predictor of DU, with a sensitivity of 77% and a specificity of 66% [11].
Biomarkers
Three studies investigated potential biochemical markers for DU diagnosis, focusing on those detectable in blood and urine samples. Ishikawa et al. examined total serum adiponectin levels, measured using a particle-enhanced turbidimetric immunoassay, as a potential predictor of DU. This method demonstrated a sensitivity of 79% and a specificity of 90% [17]. Krishnan assessed the NO/ATP ratio in urine samples with the use of ELISA kits, comparing DU patients to healthy controls. This marker reached both sensitivity and specificity levels exceeding 88% for DU diagnosis [18]. In contrast, the third study showed that several hematological serum markers, including Prognosis Nutrition Index (PNI), Systemic Immune Inflammation Index (SII), Neutrophil to Lymphocyte Ratio (NLR), and Platelet to Lymphocyte Ratio (PLR), were not significant predictors of DU [38].
Artificial intelligence and machine learning
Three studies incorporated AI and deep learning to diagnose DU. Matsukawa et al. developed an AI-based model established using only UFL data, tenfold stratified cross-validation, and data augmentation, which demonstrated a sensitivity of almost 80% and a specificity of over 88% for DU diagnosis and over 50% sensitivity and 83% specificity for DU + BOO + diagnosis [16]. Another study investigated parameters developed with the help of AI based on UFL, including first peak flow rate and the ratio of the first peak flow rate to Qmax. The first peak flow was defined as the point in the voiding wave shape at which the urine flow rate decreases. Even if the gradient of the urine waveform decreased, it was not judged as the first peak flow unless the gradient was negative. Both parameters showed good diagnostic performance, with sensitivities of 72% and 76%, and specificities of 86% and 83%, respectively [34]. The third study utilized a deep learning diagnostic platform based on UFL graphs analysis, achieving a sensitivity of over 65% and specificity of 68% [15].
Symptom questionnaires
One study developed a new questionnaire, the DUA Symptom Questionnaire (DUA-SQ), consisting of eight targeted questions addressing urinary symptoms. These questions included erectile dysfunction, long duration of void, nocturia, abdomen distention, sensation of void, straining, bowel dysfunction, and weak stream. Each symptom was assessed based on its severity and was assigned a score of 0, 5, 10, or 15 points. The questionnaire demonstrated a sensitivity of 95.8% and a specificity of 95.4% for predicting DU in patients who scored more than 45 points [35].
Additional parameters
Other studies evaluated various parameters, including PV, age, and PSA level. Kiba et al. found that smaller PV, older age, and less urgency may be clinical features of DU. The study identified 39 mL as the optimal cutoff value for PV for the diagnosis of pure DU, with a sensitivity of 75% and a specificity of 67% [30]. Wu et al. examined a PSA cut-off value of 2.9 ng/mL; however, the sensitivity and specificity were low, reaching 30% and 49%, respectively. Age was also considered an ancillary factor in assessing the likelihood of DU [38].
Risk of bias assessment
When assessing the risk of bias using the QUADAS-2 tool, the risk of bias in the patient selection domain was evaluated as “low” for prospectively recruited, retrospectively analyzed cross-sectional studies [11, 13, 14, 17, 31], and “high” for retrospective cross-sectional and case–control studies. In one case–control study [18], applicability concerns were rated as”high” for patient selection and the reference standard, as the control group consisted of healthy individuals without LUTS who did not undergo PFS. Overall, due to the poor quality of the studies and data heterogeneity, the meta-analysis was not performed, and only a qualitative synthesis was conducted. For a detailed risk of bias assessment, see Figs. 2 and 3.Fig. 2. Risk of bias and applicability concerns assessment of the studies included in the systematic review using QUADAS-2 toolFig. 3A summary plot of the risk of bias for main domains of the studies created with the use of the Robvis tool [29]
Discussion
In this systematic review, we conducted a comprehensive analysis of non-invasive tests for diagnosing DU in men with non-neurogenic LUTS. Our review underscores the diversity of emerging non-invasive diagnostic methods, which include ultrasound parameters, biomarkers, uroflowmetry results, symptom questionnaires, and clinical characteristics, as well as models developed with the help of AI and machine learning. Notably, the methods identified as having the highest sensitivity and specificity were the symptom questionnaire DUA-SQ and DWT measured with ultrasound in combination with BC, respectively. Furthermore, our review highlights the potential role of machine learning and AI in developing predictive models for DU. Our study also reveals the problem of significant variability in the diagnostic criteria for DU. This underscores the need for developing standardized diagnostic criteria in order to improve both the consistency and reliability of DU diagnoses. To our knowledge, this is the first systematic review that comprehensively summarizes the up-to-date data on the non-invasive tests for DU diagnosis in men with non-neurogenic LUTS, indicating their accuracy, strengths, and limitations.
UDS, currently considered the gold-standard for diagnosing DU, poses several inconveniences for patients, including embarrassment, pain, and dysuria. UDS is also not devoid of complications, such as urinary retention, macroscopic hematuria, or urinary tract infection [40], which can be dangerous for immunocompromised patients. On the contrary, non-invasive diagnostic methods, especially UFL analysis [11, 12], symptom questionnaires [35] and diagnostic nomograms [32, 33, 36, 39], offer a more convenient, non-traumatic, and safer alternative. These methods rely on easily accessible parameters (e.g., UFL, IPSS, age, PV), facilitating quicker diagnoses, even in uncooperative patients and during initial outpatient visits. Additionally, symptoms questionnaires and diagnostic nomograms are intuitive, easy to follow and integrate into daily clinical practice, unlike UDS, which requires highly trained experts for accurate interpretation and diagnosis.
The integration of AI into diagnostic methods has only recently begun but holds significant promise for the future. Matsukawa et al. were pioneers in developing an AI system capable of diagnosing lower urinary tract dysfunction (LUTD) by calculating BCI and BOOI directly from UFL waveforms. Preliminary findings indicated that the AI system diagnosed DU or BOO with high sensitivity and specificity, utilizing only limited data. When the diagnostic accuracy of the AI system was compared to that of three urologists, the AI system outperformed the clinicians, achieving a sensitivity of 80% and a specificity of 100% for DU diagnosis, whereas the urologists had a sensitivity of 46.7% and a specificity of 80% [16]. AI also contributes to the development of new diagnostic parameters derived from established tools like UFL. In another study, Matsukawa et al. proposed using the first peak flow rate and the ratio of the first peak flow rate to Qmax in UFL as diagnostic markers for DU. Both parameters were developed with AI assistance and can be easily implemented into clinical practice [34]. Additionally, deep learning diagnostic platforms, such as one developed by Bang et al., can interpret UFL results and assist clinicians in decision-making by quickly analyzing and comparing vast data sets [15].
The ongoing search for serum or urine biomarkers for DU is also promising, as they could provide more objective diagnostic tools with straightforward interpretation. Ishikawa et al. studied adiponectin, a beneficial adipokine with reported anti-inflammatory and anti-atherogenic properties [41, 42], as a potential DU predictor. Adiponectin was easy to measure and had good reproducibility, with a cutoff value of 8 μg/mL, providing high sensitivity and specificity for DU diagnosis. These findings suggest that adiponectin could serve as a useful screening marker for bladder dysfunction and may potentially predict treatment efficacy for LUTS, including surgical interventions. Nevertheless, the precise relationship between urodynamic parameters and adiponectin remains unclear and warrants further investigation [17]. Another potential biomarker is the NO/ATP ratio in urine samples. Since ATP and nitric oxide (NO) released from the urothelium have been shown to affect the afferent stimuli arising from the bladder [43], Krishnan et al. investigated the NO/ATP ratio in patients with DU, comparing it to healthy, age- and sex-matched volunteers without LUTS. Although the study found no correlation between urinary ATP and NO levels, and urodynamic parameters, the NO/ATP ratio showed excellent discrimination between DU patients and controls, with an area under the curve (AUC) of 0.91. This indicates that urinary NO and ATP levels warrant further exploration as potential DU biomarkers. If implemented, this method would be entirely non-invasive, requiring only urine samples from patients [18].
Despite the strengths of the studies included in this review, several limitations and concerns about the methods, their quality, and reliability remain. Most studies were retrospective, single-center, and conducted in Asia, which introduces selection bias. Moreover, none of the studies published after 2023 applied the newly introduced ICS-SUFU standards on PFS analysis [10], likely because their research began before the updated guidelines took effect. Future studies that avoid relying on a strict DCI < 100 threshold are needed to more precisely assess the detrusor function. Given the limited utility of a single cutoff at 100 for defining a weak detrusor, using DCI as a continuous variable or introducing an additional “very weak” threshold (DCI < 50) may provide greater clinical relevance and utility in daily practice. Additionally, none of the diagnostic methods have undergone external validation, further limiting their applicability. Although Krishnan et al. conducted a case–control study, the control group consisted of healthy, age- and sex-matched volunteers without any LUTS (indicated by a zero IPSS score), who did not undergo UDS. This may have led to overly optimistic findings [18]. Several studies did not account for patient medications [15, 32, 34, 35], included patients on drugs affecting detrusor function [13, 30, 33, 39] or only ceased medication three days prior to UDS [37]. Overlooking the impact of medications on bladder function might have affected the studies’ results. Additionally, some researchers excluded patients who could not void over 150 mL during UFL [15, 37, 39] or whose total voided and residual urine volumes in UFL were under 100 mL [34]. These exclusions limit applicability, as patients with the most severe LUTS were omitted from the study cohort. It is important to note that some diagnostic tools were restricted to specific patient subgroups. For example, Yoldas developed a diagnostic tool solely for men over 80 years old [37], while de Nunzio et al. created a method applicable to males with LUTS, a small prostate (median 30 g) not receiving medical treatment for LUTS [14]. This suggests that a universal tool applicable to all patients may not exist. Instead, various non-invasive diagnostic methods tailored for specific subgroups might be necessary.
Moreover, even though some methods seem quick and easy to follow, such as the newly developed DUA-SQ, proposed by Kim et al. [35], they are highly subjective. Its results depend on a patient’s understanding of symptoms, current well-being, and patient-clinician dialogue, which can lead to significant variability.
Some methods rely on ultrasound to measure BWT [14, 31] or DMT/BWT ratio [13]. To standardize measurement conditions, BWT was assessed in a bladder prefilled with a calculated volume of fluid via catheterization. This approach is suboptimal, as each catheterization increases the risk of urinary tract infection, especially in patients with neutropenia or renal diseases [44]. Moreover, ultrasound diagnoses are operator-dependent, and require consistent training to ensure reproducibility of results.
Other methods are based on UFL analysis, which has already demonstrated diagnostic utility in various urological conditions. Despite the quick and easy implementation of UFL, recent data suggest that several factors, including diurnal, postural, locational, and operator variability, may introduce variability in test results, affecting its overall diagnostic value [45]. Matsukawa et al. faced challenges in precisely evaluating UFL flow patterns, particularly "sawtooth" and "interrupted" waveforms, noting that interpretations could vary between clinicians [11]. A study by Lee et al. identified DeltaQ as the most specific and sensitive UFL parameter, however, it exclusively included patients with DU or BOO, excluding men with mixed urodynamic issues. Limited data on other conditions that may also affect DeltaQ highlights the need for further prospective trials [12].
Regarding DU biomarkers, Ishikawa et al. introduced adiponectin as a possible DU predictor. However, this study did not evaluate other major pathological factors associated with lifestyle-related diseases and metabolic syndrome, such as leptin, TNF-α, or interleukin-6. Furthermore, the study did not include patients with lifestyle-related diseases or varying BMI—the median BMI of 23.0 appeared low compared to Western populations. Lastly, it remains unclear whether serum adiponectin levels increase following LUTS treatment or whether elevated adiponectin levels improve bladder function [17]. Wu et al. aimed to analyze the potential of systemic inflammatory markers in predicting DU in BPH patients with LUTS and low PV [38]. The study posited that inflammatory markers in the bloodstream might correlate with chronic bladder ischemia, contributing to DU. However, their role as potential markers was not confirmed. It is essential to recognize that identifying new biomarkers and incorporating them into clinical practice can be costly and time-consuming. Additionally, the pathogenesis of DU is multifactorial, involving a complex interplay of aging, neurogenic, myogenic, and iatrogenic factors [46], making it unlikely to find a single universal biomarker for DU.
Recent advancements in AI have also impacted DU diagnostic methods. The initial study by Matsukawa et al. in 2021, which developed an AI-based model, encountered several limitations. The AI system did not learn normal patient waveforms, and the evaluation of reproducibility within the same patient was insufficient. Diagnosing coexisting pathological conditions, such as concurrent DU and BOO, also proved challenging [16]. In 2023, Matsukawa et al. utilized AI to develop new specific parameters derived from available UFL data to aid in DU diagnosis. However, this study also had limitations, including an analysis restricted to only 266 cases due to the requirement for precise 0.1-s interval measurements of urinary flow waveforms. Additionally, when the voided volume is too low, the UFL waveform often appears monophasic, regardless of LUTS pathophysiology, which may render parameters related to the first peak flow ineffective for differentiating DU [34]. Bang et al., on the other hand, used deep learning in order to create a diagnostic platform based on UFL graphs analysis. However, the prediction rate was only slightly over 70%, and the capacity to set the basis for model predictions confined due to the absence of external data [15].
Future research on diagnostic methods should not only focus on identifying non-invasive markers for diagnosing DU but also on evaluating the degree of detrusor weakness by considering the DCI as a continuous variable. A key question is whether these methods can determine a patient’s candidacy for surgical intervention and accurately predict likely benefit. In the recent UPSTREAM trial, patients with LUTS who had BCI greater than 123.0 showed more favorable outcomes following surgery [47], underscoring the need to develop non-invasive tools that can reliably identify those most likely to benefit from surgical treatment.
Several non-invasive methods included in this analysis, particularly those that are straightforward to use in clinical practice and have high sensitivity – such as the DUA-SQ questionnaire [35] or the "sawtooth and interrupted" waveform on UFL [11] – could serve to preselect patients for invasive UDS, after external validation of these methods. This approach would improve the diagnostic process and reduce costs. Moreover, combining multiple existing techniques into a single diagnostic algorithm and evaluating its overall accuracy could further enhance clinical decision-making for DU.
Conclusions
Non-invasive diagnostic methods, including ultrasound parameters, biomarkers, UFL analysis, symptom questionnaires, clinical characteristics, and AI integration, show promise in diagnosing DU and offer safer, more convenient alternatives to invasive UDS. However, many methods face limitations such as a lack of accuracy and external validation, as well as variability in test conditions, which affect their reliability and applicability. Our work provides a valuable resource for clinicians seeking to optimize diagnostic strategies for DU by consolidating evidence on the efficacy and limitations of these non-invasive tests. Furthermore, our analysis highlights important areas that require further investigation to refine existing methods, examine their applicability, and create diagnostic tools customized for specific patient subgroups.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ICS Standards 2024. Retrieved from: https://www.ics.org/Publications/ICS%20Standards%202024.pdf Accessed 20 Oct 2024
- 2Szmydki D, Burzyński B, Sołtysiak-Gibała Z, Przymuszała P, Trzewik M, Chudek J, Owczarek AJ. Prediction of detrusor underactivity based on non-invasive functional tests and clinical data in patients with symptoms of bladder outlet obstruction. Eur Rev Med Pharmacol Sci. 2020;24(21):10992–8.10.26355/eurrev_202011_2358333215413 · doi ↗ · pubmed ↗
- 3QUADAS-2 Template for tabular display. Retrieved from: https://www.bristol.ac.uk/population-health-sciences/projects/quadas/resources/ Accessed 10 Aug 2024
- 4Mc Guinness LA, Higgins JPT. Risk-of-bias VI Sualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods. n/a(n/a). Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/jrsm.1411. Accessed 10 Aug 2024.10.1002/jrsm.141132336025 · doi ↗ · pubmed ↗
- 5Garbas K, Zapała Ł, Ślusarczyk A, Piecha T, Gwara P, Żuk-Łapan A, et al. (A)voiding misdiagnosis: prediction of detrusor underactivity vs. bladder outlet obstruction using pre-urodynamic nomogram in male patients with LUTS. Int Urol Nephrol. 2024. [cited 2024 Sep 16]; Available from: https://link.springer.com/10.1007/s 11255-024-04093-710.1007/s 11255-024-04093-7PMC 1146461038819576 · doi ↗ · pubmed ↗