Rapidly progressive mitral valve disease from non-bacterial thrombotic endocarditis to mitral stenosis in systemic lupus erythematosus: a case report
Saaya Ichikawa-Ogura, Yasuhide Mochizuki, Eiji Toyosaki, Hiroto Fukuoka, Toshiro Shinke

TL;DR
A rare case shows how heart valve disease in a lupus patient progressed from one type of valve issue to another, resembling rheumatic heart disease.
Contribution
This case report highlights an unusual progression of non-bacterial thrombotic endocarditis to mitral stenosis in a patient with SLE and APS.
Findings
Non-bacterial thrombotic endocarditis initially caused mitral regurgitation, which improved with vitamin K antagonist therapy.
The patient later developed rheumatic-like mitral stenosis requiring surgical valve replacement.
The patient suffered a fatal cerebral infarction post-surgery, likely due to antiphospholipid syndrome.
Abstract
Libman–Sacks endocarditis), a non-bacterial thrombotic endocarditis (NBTE) linked to systemic lupus erythematosus (SLE) and antiphospholipid syndrome (APS), typically causes valve regurgitation and embolism but can rarely mimic rheumatic mitral stenosis (MS). This case involves a 59-year-old woman with a history of APS and SLE who presented with worsening dyspnoea and congestive heart failure. Initially, severe mitral regurgitation (MR) due to NBTE resolved with vitamin K antagonist therapy, yet she subsequently developed significant MS with commissural fusion, a rheumatic-like feature. Despite stable SLE activity, echocardiography revealed severe MS with high pulmonary pressures, warranting surgical valve replacement. Intraoperative findings confirmed rheumatic-like degeneration, but the patient experienced a fatal cerebral infarction post-surgery, likely due to APS. This case…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1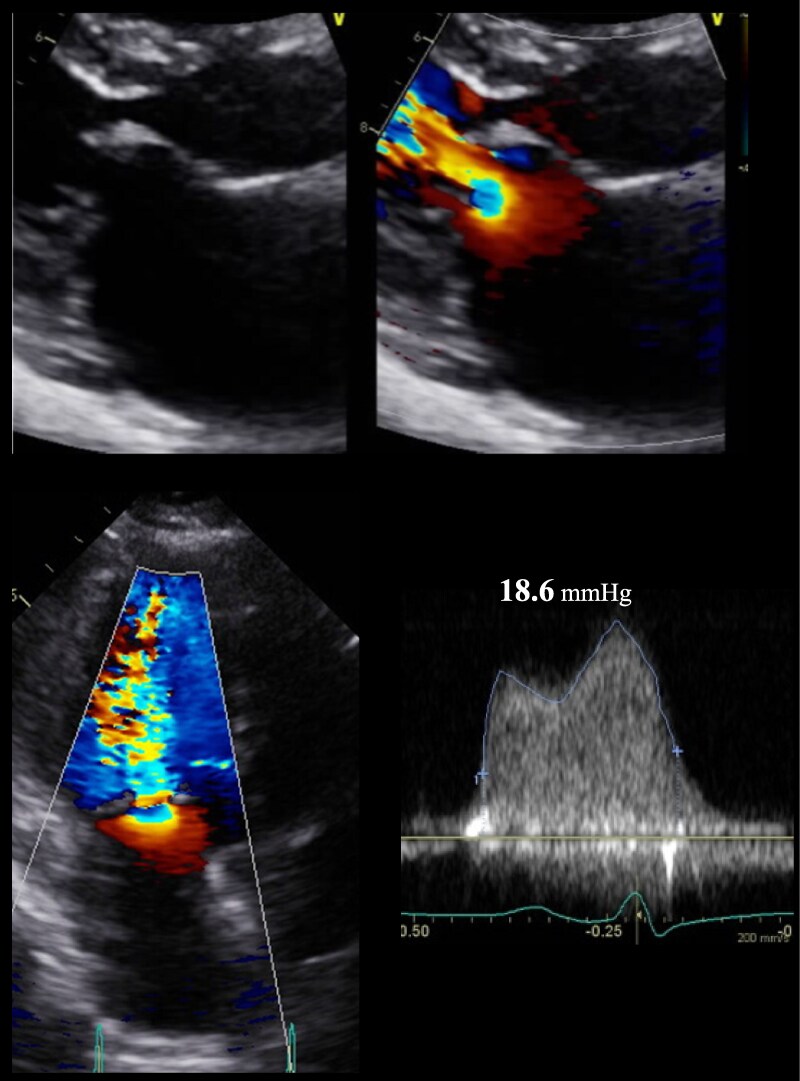 Figure 2
Figure 2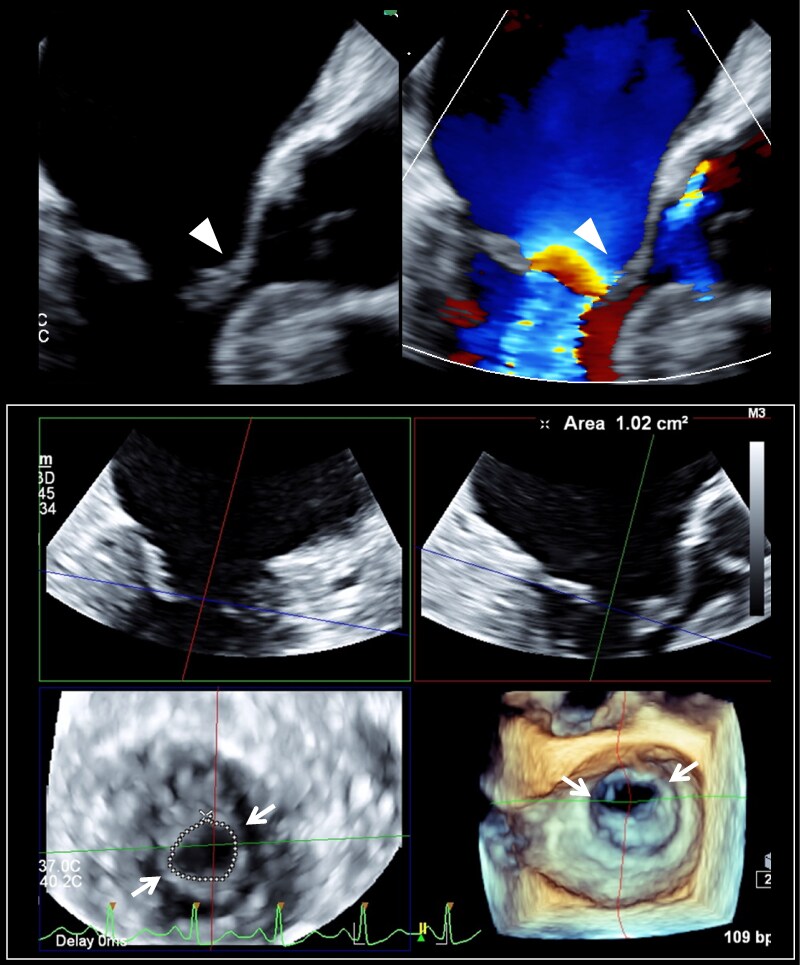 Figure 3
Figure 3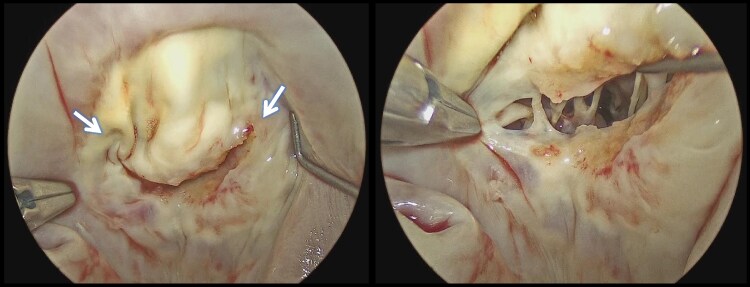 Figure 4
Figure 4| Date | Event | Figure |
|---|---|---|
| 15 years old |
Diagnosis of antiphospholipid syndrome | |
| 18 years old |
Diagnosis of systemic lupus erythematosus | |
|
Steroid therapy initiated | ||
| 55 years old (2019/2) |
Dyspnoea on exertion appeared |
|
|
Echocardiography demonstrated severe mitral regurgitation (MR) with non-bacterial thromboendocarditis (NBTE) | ||
|
Anticoagulation therapy (warfarin potassium) started | ||
| 55 years old (2019/10) |
MR improved to mild grade |
|
|
NBTE had almost disappeared | ||
| 58 years old (2022/11) |
Echocardiography revealed mild MR and newonset mitral stenosis (MS) |
|
| 59 years old (2023/11) |
Hospitalization due to congestive heart failure |
|
|
Elevated brain natriuretic peptide level of 895 pg/mL | ||
|
Echocardiography showed severe MS and pulmonary hypertension | ||
| 59 years old (2023/11) |
Surgical mitral valve replacement (27-mm MITRIS RESILIA) |
|
| Parameter | Result | Normal range (for an adult woman) |
|---|---|---|
| White blood cell count, /μL | 12 700 | 4000–11 000 |
| Haemoglobin, g/dL | 7.5 | 12.1–15.1 |
| C-reactive protein, mg/dL | 3.1 | <0.1 |
| BNP, pg/mL | 895 | ≤18.4 |
| Serum creatinine, mg/dL | 1.74 | 0.5–0.9 |
| Creatinine clearance, mL/min | 33.5 | 80–130 |
| Lupus anticoagulant test | Positive | Negative |
| Haemolytic complement activity, U/mL | 55 | 30–50 |
| Anti-dsDNA antibody levels, IU/mL | 0.6 | <30 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Systemic Lupus Erythematosus Research · Infective Endocarditis Diagnosis and Management
Introduction
Libman–Sacks endocarditis (LSE), described in 1924 by Emanuel Libman and Benjamin Sacks, is a cardiac manifestation of systemic lupus erythematosus (SLE). It presents as sterile vegetation on mitral and aortic valves and is a type of non-bacterial thrombotic endocarditis (NBTE) linked to SLE and antiphospholipid syndrome (APS). Key complications include systemic embolism and regurgitation from incomplete valvular coaptation. Rarely, LSE mimics rheumatic valvular disease, causing stenosis through inflammatory commissural fusion.^1–4^ We present a case where anticoagulation effectively treated NBTE-associated mitral regurgitation (MR), but rheumatic-like mitral stenosis (MS) developed over four years, necessitating surgical valve replacement.
Summary figure
**: **
Case presentation
A 59-year-old woman was diagnosed with APS at age 15 and SLE at age 18. She later developed central nervous system lupus, recurrent miscarriage, thrombocytopaenia-related irregular vaginal bleeding, and lupus nephritis. Her history included steroid-induced diabetes, bronchial asthma, and avascular necrosis of the femoral head. At age 55, she presented with exertional dyspnoea. Transthoracic echocardiography (TTE) and transoesophageal echocardiography (TOE) revealed severe MR and a 5 mm mass on the left atrial side of both mitral valve leaflets (Figure 1). Transthoracic echocardiography revealed left ventricular ejection fraction (LVEF) of 62%, left atrial volume of 40 mL/m^2^. The mean pressure gradient (MPG) through the mitral valve was 5.3 mmHg, and the mitral valve area (MVA) calculated using the pressure half-time (PHT) method was 2.3 cm², suggesting mild MS. Two sets of blood cultures were negative, and she was diagnosed with NBTE associated with LSE. Oral anticoagulation therapy with vitamin K antagonist (VKA) was initiated via heparin bridging therapy, and prothrombin time and international normalized ratio was stably maintained at around 2.0 with 2 mg. After 8 months of sustained therapy, the NBTE resolved completely, and MR improved to a mild grade (see Supplementary material online, Movie S1). At age 58, TTE revealed progression to moderate MS with MPG of 7.5 mmHg, MVA of 1.1 cm² by PHT, and 1.4 cm² by planimetry, along with bilateral commissural fusion, while MR remained mild. Brain natriuretic peptide (BNP) levels remained relatively low at ∼30 pg/mL, and SLE disease activity was well-controlled. At age 59, she presented with a 1-month history of persistent dyspnoea and was admitted for congestive heart failure (HF). Physical examination revealed bilateral lower limb oedema, and auscultation detected wheezing. Electrocardiography revealed sinus rhythm with a heart rate of 105 beats/min. Chest radiography demonstrated pulmonary congestion and bilateral pleural effusions. As shown in Table 1, the laboratory data revealed elevated inflammatory markers and a marked increase in BNP levels. The patient had been prescribed daily oral medications in the outpatient setting, including 2 mg warfarin potassium, low-dose aspirin, 16 mg prednisolone, and 1250 mg mycophenolate mofetil daily, which were continued after admission. After approximately one week of treatment for congestive HF with intravenous furosemide 20 mg/day and oral tolvaptan 3.75 mg, the congestion improved. On admission, TTE showed a preserved LVEF of 60% and a left atrial volume index of 42 mL/m². The MVA with bilateral commissural fusion was 0.86 cm² (calculated by continuity equation), and the MPG was markedly elevated at 18.6 mmHg, confirming severe MS (Figure 2, Supplementary material online, Movie S2). Transoesophageal echocardiography performed after HF treatment confirmed thickened mitral leaflets, complete resolution of the NBTE, bilateral commissural fusion, and diastolic doming (Figure 3 and Supplementary material online, Movie S3). The mitral valve area was calculated as 1.02 cm² using three-dimensional multiplanar reconstruction analysis. No significant valvular disease other than MS, thrombi, or vegetation was detected. Cardiac catheterization revealed an elevated pressure gradient of 25 mmHg between the pulmonary artery wedge pressure and the left ventricle, suggesting increased left atrial pressure. The mean pulmonary arterial pressure was 30 mmHg, indicating post-capillary pulmonary hypertension. These findings confirmed that MS was clinically significant. Given the high surgical risk with an STS score of 27.5 for mitral valve replacement, percutaneous transvenous mitral commissurotomy was considered a less invasive alternative. However, the severe commissural fusion and the history of NBTE raised concerns about procedural embolism. After a heart team conference, surgical valve replacement was chosen. The operation was performed two months after the HF hospitalization. Vitamin K antagonist was discontinued three days before surgery, and strict anticoagulation management was achieved during the perioperative period using intravenous heparin, monitored with the HMS PLUS heparin concentration measurement system (Medtronic). A 27-mm MITRIS RESILIA bioprosthetic valve was implanted. Intraoperative findings were consistent with TOE results, revealing rheumatic degeneration characterized by bilateral commissural fusion and leaflet thickening (Figure 4). Despite rigorous perioperative management, including intravenous heparin and HF control, the patient developed a left middle cerebral artery infarction, presumably due to APS, and died on postoperative Day 180.
Transthoracic (A) and transoesophageal (B) echocardiography in February 2019 showing non-bacterial thrombotic endocarditis (white arrow) and severe mitral regurgitation.
Transthoracic echocardiography at admission for congestive heart failure revealed severe mitral valve stenosis, with a mean transvalvular pressure gradient of 18.6 mmHg across the mitral valve.
Transoesophageal echocardiography during hospitalization for congestive heart failure in November 2023 demonstrated severe mitral valve stenosis. The mitral valve leaflets showed marked thickening with doming of the anterior leaflet (arrowhead), and commissural fusion (white arrow) with severe restriction of valve opening was evident. The mitral valve area was calculated as 1.02 cm² using three-dimensional multiplanar reconstruction analysis.
Intraoperative view showing bilateral commissural fusion (arrow), with marked thickening of both mitral valve leaflets and chordae tendineae.
Discussion
This report highlights an atypical clinical course of LSE. The patient initially presented with MR due to NBTE, which resolved completely with VKA therapy but later progressed unexpectedly to rheumatic-like MS, culminating in congestive HF (see Supplementary material online, Movie S4).
Non-bacterial thrombotic endocarditis presents as sterile fibrin-platelet thrombi mainly affecting mitral and aortic valves, occurring in autoimmune diseases, malignancies, and disseminated intravascular coagulation. In SLE/APS, it’s called LSE and can develop regardless of disease activity. Patients with antiphospholipid antibodies are prone to valve disease, with immune complex deposits suggesting immune-mediated inflammation.^3,5,6^ As shown by TOE in this case, NBTE features no valve destruction, with symmetrically aligned mass echoes on the mitral atrial rough zone, differing from infective endocarditis. Negative blood cultures and resolution of mass echoes with anticoagulation alone further distinguished it from infective endocarditis. Management of NBTE typically involves intravenous unfractionated or low-molecular-weight heparin to prevent embolic events. While VKA is not superior to heparin, preventing thromboembolism in APS requires high-intensity warfarin therapy.^7^ Approximately 70% of NBTE cases resolve after VKA therapy,^8^ and surgical intervention is reserved for refractory cases.^9,10^ In one reported instance, NBTE due to APS resolved, and MR severity improved following VKA therapy.^11^ In this patient, bridging intravenous heparin to VKA improved MR while mitigating procedural risk.
In SLE, MR is common, while MS is rare. Roldan et al.^12^ reported stenotic valvular disease in 4% of SLE patients using TOE, with no new cases or progression during follow-up exams. Similarly, Moyssakis et al.^4^ noted mild to moderate MS in (2.6%) of patients with SLE, with progression to severe MS during the follow-up period. A case report showed SLE/APS-associated mild MR progressing to severe MS and regurgitation after a 5-year interruption in treatment.^13^ While our case differs, showing MS progression despite optimal therapy, both cases suggest valvular disease can progress independently of SLE/APS activity and may rapidly worsen at any disease stage.
The development of rheumatic-like MS in patients with SLE remains unclear but may involve chronic inflammation leading to progressive valvular thickening, fibrosis, and scarring. Cross-reactivity in antibody specificity between rheumatic fever and APS^14^ may contribute to similar valvular degeneration, mimicking the pathology of MS.
Finally, there are no reports of successful long-term outcomes of percutaneous transvenous commissurotomy in SLE patients with APS. With risks of recurrence and perioperative thrombosis, it may be an option but is unlikely to be curative.
Conclusion
This case presents a rare NBTE in SLE/APS, featuring MR improvement with VKA treatment, yet rapid progression to rheumatic-like MS despite controlled SLE, leading to fatal surgical intervention. This highlights the necessity of regular echocardiographic monitoring with careful attention to mitral valve morphology.
Supplementary Material
ytaf098_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Asopa S, Patel A, Khan OA, Sharma R, Ohri SK. Non-bacterial thrombotic endocarditis. Eur J Cardiothorac Surg 2007;32:696–701.17881239 10.1016/j.ejcts.2007.07.029 · doi ↗ · pubmed ↗
- 2Lee JL, Naguwa SM, Cheema GS, Gershwin ME. Revisiting Libman–Sacks endocarditis: a historical review and update. Clin Rev Allergy Immunol 2009;36:126–130.19089657 10.1007/s 12016-008-8113-y · doi ↗ · pubmed ↗
- 3Hurrell H, Roberts-Thomson R, Prendergast BD. Non-infective endocarditis. Heart 2020;106:1023–1029.32376608 10.1136/heartjnl-2019-315204 · doi ↗ · pubmed ↗
- 4Moyssakis I, Tektonidou MG, Vasilliou VA, Samarkos M, Votteas V, Moutsopoulos HM. Libman–Sacks endocarditis in systemic lupus erythematosus: prevalence, associations, and evolution. Am J Med 2007;120:636–642.17602939 10.1016/j.amjmed.2007.01.024 · doi ↗ · pubmed ↗
- 5Hojnik M, George J, Ziporen L, Shoenfeld Y. Heart valve involvement (Libman–Sacks endocarditis) in the antiphospholipid syndrome. Circulation 1996;93:1579–1587.8608627 10.1161/01.cir.93.8.1579 · doi ↗ · pubmed ↗
- 6Ziporen L, Goldberg I, Arad M, Hojnik M, Ordi-Ros J, Afek A, et al Libman–Sacks endocarditis in the antiphospholipid syndrome: immunopathologic findings in deformed heart valves. Lupus 1996;5:196–205.8803890 10.1177/096120339600500306 · doi ↗ · pubmed ↗
- 7Khamashta MA, Cuadrado MJ, Mujic F, Taub NA, Hunt BJ, Hughes GR. The management of thrombosis in the antiphospholipid-antibody syndrome. N Engl J Med 1995;332:993–997.7885428 10.1056/NEJM 199504133321504 · doi ↗ · pubmed ↗
- 8Slivka AP, Agriesti JE, Orsinelli DA. Natural history of nonbacterial thrombotic endocarditis treated with warfarin. Int J Stroke 2021;16:519–525.33040698 10.1177/1747493020961744 · doi ↗ · pubmed ↗