The ‘Bounce Back’ rehabilitation programme for stroke survivors in South Africa – a case report
Laeeqa Sujee, Sacha Hildebrandt, Amy Harrison, Christa Matjekane, Thabiso Mmoledi, Sonti Pilusa, Kganetso Sekome, Adedayo T. Ajidahun

TL;DR
A low-cost community-based rehabilitation program in South Africa helped stroke survivors regain function and improve their quality of life, though returning to work remained challenging.
Contribution
Presents a community-based, low-cost rehabilitation model for stroke survivors in under-resourced settings.
Findings
All participants showed improved functional independence and health-related quality of life.
One participant experienced a clinical deterioration in depressive symptoms.
Participants faced challenges in returning to work despite rehabilitation gains.
Abstract
Stroke is one of the global leading causes of disability, with a higher prevalence at a younger age in sub-Saharan Africa. Returning to functional status is a primary goal of rehabilitation for stroke survivors. However, the cost of intensive rehabilitation is often a barrier for the under-resourced in South Africa. This article describes the individualised ‘return-to-function’ approach to rehabilitation and its outcomes for five stroke survivors delivered through a non-profit public–private partnership in a low-income community in South Africa. A retrospective case series of stroke survivors who participated in the Bounce Back Journey (BBJ) programme between 2019 and 2021 was conducted. The beneficiaries’ ages ranged from 21 to 55 years; two were females and three were males. The goals and outcomes of five stroke survivors with impairments, functional limitations and participation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
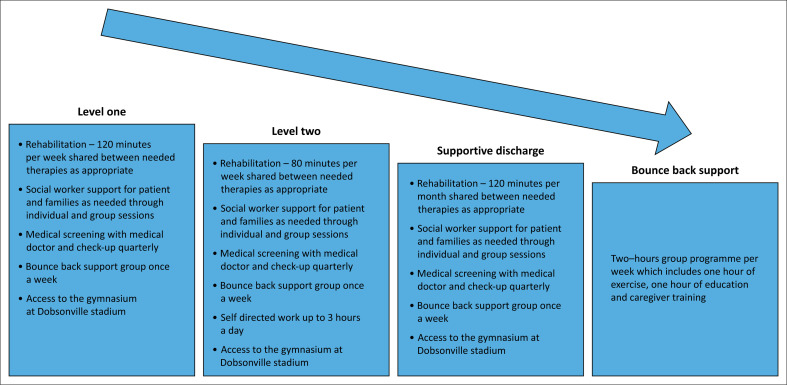 FIGURE 1
FIGURE 1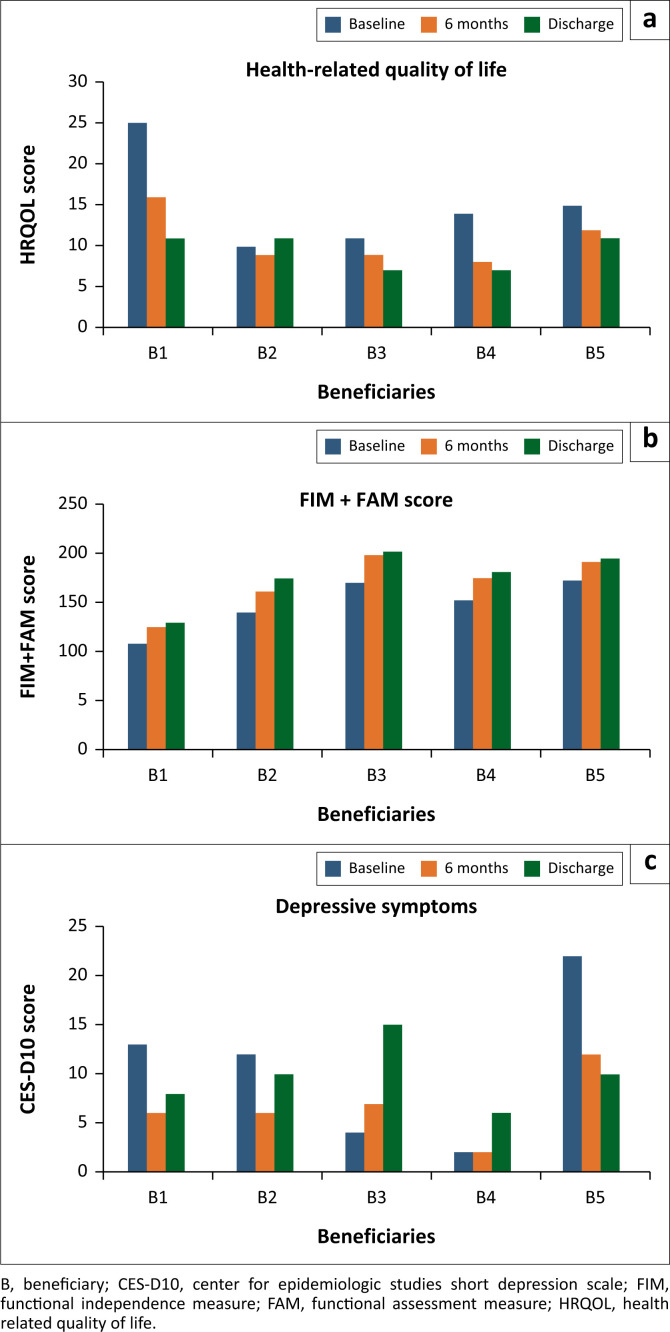 FIGURE 2
FIGURE 2| Stroke survivor | Age at stroke (years) | Gender | Post stroke started at the facility (weeks) |
|---|---|---|---|
| B1 | 55 | Male | 32 |
| B2 | 21 | Female | 78 |
| B3 | 34 | Male | 11 |
| B4 | 38 | Male | 30 |
| B5 | 41 | Female | 58 |
| Stroke survivor | Disability manifestation (at baseline) | Goals | Discharge outcomes |
|---|---|---|---|
| B1 | |||
| B2 | |||
| B3 | |||
| B4 | |||
| B5 |
| Stroke survivor | Goal set | Goal achieved (months) | |||
|---|---|---|---|---|---|
| 3 | 6 | 9 | 12 | ||
|
| |||||
| Communication | Communicate with improved speech | NA | - | - | - |
| Use the AAC system with prompting | - | A | A | - | |
| Function | Eat and drink | A | - | - | - |
| Social participation | - | - | - | - | - |
| IADL | - | - | - | - | - |
| BADL | Grooming | PA | A | A | - |
| Personal care | PA | PA | A | - | |
| Transfer | A | - | - | - | |
| Ambulate with aid or support | PA | PA | A | - | |
| Return to work | - | - | - | - | - |
| Personal | Eat normal diet | NA | - | - | - |
|
| |||||
| Function | Use the right hand to eat and write | NA | - | - | - |
| Social participation | Socialise with friends | NA | PA | PA | A |
| Attend church and shop | NA | PA | PA | A | |
| IADL | Assist with cooking | - | PA | PA | A |
| Assist with cleaning | NA | PA | - | - | |
| BADL | Grooming | PA | PA | PA | A |
| Personal care | - | PA | PA | A | |
| Transfer | - | - | A | - | |
| Communication | Use the AAC app to communicate | - | - | PA | A |
| Basic communication skills | - | - | - | - | |
| Return to work | Study social work or a short course | NA | - | - | - |
| Personal | Read the Bible | PA | PA | PA | A |
|
| |||||
| Communication | Improve cognitive-communication skills | A | - | - | - |
| Function | Use left UL | A | - | - | - |
| Social | Demonstrate verbal and non-verbal skills when interacting | - | - | PA | A |
| IADL | Prepare meal | - | - | A | - |
| Time management | - | - | - | ||
| BADL | Ambulate indoors and outdoors | A | - | - | - |
| Climb stairs | A | - | - | - | |
| Use public transportation | - | - | A | - | |
| Coping skills | - | A | - | - | - |
| Return to work | Return to work part time | - | - | NA | - |
| Fitness to drive assessment | - | - | NA | PA | |
|
| |||||
| Communication | Use AAC | NA | NA | NA | A |
| Establish yes or no | A | - | - | - | |
| Say 5–10 words | - | - | PA | - | |
| Function | Multitasking with carrying an object | - | - | - | A |
| Social | Shop | - | - | A | - |
| IADL | Cleaning | - | A | - | - |
| BADL | Grooming | - | A | - | - |
| Personal care | A | - | - | - | |
| Transfer | - | - | - | - | |
| Ambulate in the house | A | - | - | - | |
| Walk in public | - | A | - | - | |
| Use public transportation | NA | NA | NA | A | |
| Return to work | Start a business | - | - | - | NA |
|
| |||||
| Communication | - | - | - | - | - |
| Function | - | - | - | - | - |
| Social | Increase confidence in community engagements | - | A | - | - |
| IADL | Stabilise food during meal prep | - | A | - | - |
| Hang clothes | PA | A | - | - | |
| Clean | PA | A | - | - | |
| Carry a bucket of water | - | A | - | - | |
| BADL | - | - | - | - | - |
| Use public transportation | A | - | - | - | |
| Ambulate – change direction indoors and outdoors | A | - | - | - | |
| Carry a cup of tea independently | - | A | - | - | |
| Climb stairs | - | A | - | - | |
| Return to work | Return to work as a cleaner | - | NA | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStroke Rehabilitation and Recovery · Acute Ischemic Stroke Management
Introduction
Stroke is the third most common cause of adult physical disability and the second greatest cause of mortality in the world, accounting for more than 6 million deaths annually (Feigin et al. 2021). Most stroke-related deaths take place in low- and middle-income countries (LMICs) (Maredza, Bertram & Tollman 2015). Experiencing a stroke comes with multiple long-term health challenges that can worsen the primary disability.
Disability is a biopsychosocial phenomenon, depicted by the International Classification of Functioning, Disability and Health (ICF) model which describes disability as the interaction between impairment of body functions, structures, activities and participation in the context of the person’s environmental and personal factors (World Health Organization 2002). Functional outcomes and activities of daily living (ADLs) are affected in two-thirds of stroke survivors (Rosamond et al. 2007). Some of the common impairments to body functions and structures limitations presenting post-stroke are upper and lower extremity paralysis or paresis, mental health challenges and speech problems (Silva et al. 2015). The ICF has been used to evaluate disability in people post-stroke (Perin et al. 2020).
Collaborative care comprising interdisciplinary teams is recommended in stroke rehabilitation (Alessandro et al. 2020). The Phila Sonke Wellness Initiative (PSWI) Bounce Back Journey (BBJ) rehabilitation programme, based on donor funding, is an evidence-based programme developed on the person-centred social model. It uses an interdisciplinary approach to restore functional independence (FIM) and social integration and identify the best fit for means of livelihood and income for participants to improve their overall quality of life (O’Dell 2016).
This case series presents the outcomes of the BBJ programme which is a community-based, integrated team approach to stroke survivors’ rehabilitation and return to an independent functional state.
Management
Stroke survivor selection
Participants were stroke survivors living in Dobsonville, South Africa. The stroke survivors were referred to PSWI via doctors and rehabilitation healthcare providers in the public sector as well as through word of mouth. The stroke survivor beneficiary manager who is an occupational therapist screened each potential stroke survivor to be included, in two phases. The first phase involved a non-clinical screening, during which the application and all documentation were reviewed. The inclusion criteria were individuals older than 13 years, unable to receive intensive rehabilitation in the public or private sector because of resource scarcity, long waiting lists and a lack of capacity to see patients more frequently. Participants were excluded if the stroke incident was more than 18 months prior to application, if they were unwilling to share accurate financial information about their household income, if their primary disability was mental or psychological as per medical doctor diagnosis and if there had been a recent history of drug and substance abuse. There were no other limitations based on the number of previous strokes or comorbidities.
Intervention programme
The second phase involved the BBJ rehabilitation programme which was a graded intervention programme delivered by healthcare professionals with a special interest in neurorehabilitation. The BBJ rehabilitation programme is based on the person-centred care framework that includes the person’s well-being, context, expression, preferences and beliefs (Ekman et al. 2011). The programme involved the stroke survivor starting on a specific level based on the initial assessment, and then the intensity of therapy was weaned down as goals were achieved. This slow grading strategy aimed to support the stroke survivors and encouraged their empowerment and independence. Stroke survivors were allocated to a certain therapy intensity level approved by a case management team comprised of occupational therapists and physiotherapists, for a particular period of rehabilitation based on the assessments of the stroke survivor beneficiary manager and the recommendations of the rehabilitation team. The rehabilitation team included a physiotherapist, occupational therapist, speech therapist, social worker and medical doctor. The programme was implemented at no cost to the stroke survivor and was fully funded through the non-profit organisation PSWI. The length of stay in the levels was dependent on the patients’ outcome and level of independence. At supportive discharge, all the participants had been in the programme for at least 9 months. The content of the programme is outlined in Figure 1.
Bounce back journey rehabilitation programme.
Outcome measures
Functional independence
The FIM+FAM measure is a 30-item scale that measures dependence. The domains measured include – self-care, transfer and mobility, communication, cognition and psychosocial function (Turner-Stokes et al. 1999). The tool is validated with stroke survivors and has high internal consistency (Cronbach alpha = 0.98) (Turner-Stokes & Siegert 2013). Higher scores on the FIM+FAM measure show increased independence; the lower the score, the more dependent the patient is (UK FIM+FAM Users Group 2012). Formal permission for use is not required.
Depression
The Center for Epidemiologic Studies Short Depression Scale (CES-D10) is a 10-item questionnaire developed to measure depression symptoms among adults. The tool has been validated among the South African general population (Baron, Davies & Lund 2017) and shows high internal consistency (Cronbach’s α = 0.86). The higher the score, the higher the depressive symptoms, with a score of ≥ 10 showing substantial symptoms of depression (Andresen et al. 1994).
Health-related quality of life
The EQ-5D-5L questionnaire measures health-related quality of life. The tool has been validated in several patient groups, including patients with stroke. The EQ-5D-5L is a valid and reliable tool that measures health changes. Formal permission for digital use was obtained from the EuroQol Research Foundation. The lower the health-related quality of life scores, the fewer problems the patient faces (Oeman & Jansen 2013).
Procedure
There were two teams involved in the programme. The first team was the case management team which comprised rehabilitation professionals. It included a stroke survivor beneficiary manager, programme coordinator, research coordinator and a moderator who facilitated review meetings. The stroke survivor beneficiary manager contacted the potential stroke survivor if they met the initial inclusion and exclusion criteria based on their application, and they were then invited for an in-person clinical assessment. The assessment included baseline measurements with three outcome measures: quality of life (EQ-5D-5L), depression (CES-D10) and FIM/FAM. This assessment was to confirm the potential stroke survivor’s capabilities based on the outcome measures. In addition, the stroke survivor beneficiary manager assessed body impairments, activity limitations and participation restrictions as per the ICF framework. This assisted the case management team in making the decision regarding which level of the BBJ programme the stroke survivor should be included in. Once the case management team had allocated the stroke survivors to an appropriate programme level, they were enrolled and referred to the second team involved in the programme, the rehabilitation team which carried out interdisciplinary assessments. These included a first medical appointment, a physiotherapy assessment, an occupational therapy assessment, a speech therapy assessment and a social work assessment. These assessments were person-centred and at the discretion of each therapist. The assessments allowed the therapy team to allocate adequate time and schedule rehabilitation sessions for the stroke survivor as required.
It was paramount that the stroke survivor set SMART (specific, measurable, attainable, realistic and time-bound) goals during these initial sessions so that a plan regarding therapy could be determined between the therapist and the stroke survivor. All goal setting was carried out as a treatment strategy, where therapists spent time with the stroke survivor to help them formulate goals in their own words. This emphasised the stroke survivor-centred, stroke survivor-driven and therapist-guided approach that the initiative strove to achieve.
The stroke survivor beneficiary manager held monthly meetings with the rehabilitation team to discuss each stroke survivor’s goals and progress as well as brainstorm different treatment and management techniques and approaches. Quarterly, the stroke survivor beneficiary manager met with each stroke survivor to reassess the outcome measures of FIM, depressive symptoms and health-related quality of life. These sessions also included discussions with the stroke survivor regarding their progress, their needs and what they hoped to achieve in rehabilitation going forward. The results were then reviewed by the dedicated case management team alongside the beneficiaries’ goals, outcomes and recommendations from the rehabilitation team. These findings allowed the case management team to determine a change in programme level for the next quarter as well as address requests or concerns from the stroke survivor and rehabilitation team.
Ethical considerations
Ethical clearance to conduct this study was obtained from the University of the Witwatersrand, Human Research Ethics Committee (reference no.: M231090). Written informed consent was provided by all the beneficiaries.
Patient presentation and outcomes
Sample description
Five stroke survivors who had a stroke between 2019 and 2021 were managed under this programme. The stroke survivors’ median age was 39 (IQR:27.5-48) years. There were two females and three males (Table 1).
Disability
On admission into the programme, all stroke survivors had no finances to access private, intensive rehabilitation. They had all been to government facilities previously. Table 2 presents their baseline disability, goals and discharge outcomes.
Stroke survivor goals
As shown in Table 2, in general, goals set focussed on improving function, ADLs, social participation, communication and return to work. Most stroke survivors’ goals were achieved or partially achieved within the first 6 months of the programme. For the programme’s first 3 months, the goals were focussed mainly on function, social participation and ADLs. In the second and third quarters of the programme, the stroke survivors’ goals were geared towards returning to work. Although these return-to-work goals were mostly not achieved, the programme appeared to place them on a trajectory that introduced them and prepared them for future vocational opportunities by maximising their level of function to adapt to their current work interest or alternate work entirely. Table 3 outlines the specific goals and goals achieved over the period of the programme.
Figure 2 shows the CES-D10, FIM+FAM and EQ-5D-5L scores for all participants at baseline, 6 months and at discharge demonstrated improvements for all three outcomes. At baseline, three stroke survivors (B1, B2 and B5) had CES-D10 ≥ 10, and for these three, the CES-10 score decreased at 6 months and discharge, compared to the baseline, indicating a reduction in depressive symptoms. However, it is interesting to note that B3 presented with an increased score over the course of the programme, which indicated an increase in clinically significant depressive symptoms despite their improved FIM and quality of life (Figure 2). The FIM+FAM score compared to the baseline was higher in all the beneficiaries at 6 months and upon discharge, demonstrating improved FIM. At baseline, the FIM+FAM scores ranged from 108 to 173, and at discharge, they ranged from 130 to 202 (Figure 2). The health-related quality of life score decreased in all the beneficiaries at 6 months and discharge compared to the baseline, demonstrating improved quality of life. At baseline, the EQ-5D-5L scores ranged from 10 to 25, and at discharge, the scores ranged from 7 to 11 (Figure 2).
Baseline, 6 months and discharge outcome measures of functional independence, health-related quality of life and depressive symptoms of the stroke survivors.
Discussion
The BBJ project, using a community-based, interdisciplinary approach, was conceptualised to restore FIM, social participation and quality of life to stroke survivors. Between 2019 and 2021, five stroke survivors consecutively participated in the programme. The outcomes showed that via engagement with this programme, these five stroke survivors achieved most of their goals regarding FIM, cognitive functioning, social participation and improved daily living activities.
Functional independence and quality of life had improved at discharge in all stroke survivors. This is not surprising as evidence has shown that rehabilitation interventions improve quality of life, cognitive functioning and FIM post-stroke (Gao et al. 2024). However, the evaluation of depressive symptoms at baseline and discharge did not show similar outcomes. Only one stroke survivor (B1) reported a clinically significant reduction in depressive symptoms (from CESD10 ≥ 10 to CESD10 < 10). An interesting finding was the increase in clinically significant depressive symptoms (from CESD10 < 10 to CESD10 ≥ 10) in B3 at discharge compared to baseline. The presence and persistence of depressive symptoms and anxiety post-stroke are common whether or not the stroke survivors have access to rehabilitation programmes (Hartley, Burger & Inglis-Jassiem 2022; Mahadevan et al. 2021), and it has been reported that depressive symptoms and anxiety are more common in younger adults compared to older people (> 50 years) (Kapoor et al. 2019). In our study, the only stroke survivor (B1) who had a clinically significant reduction in depressive symptoms was also the oldest (mid-fifties), while the others were within the younger adult age group.
Some dynamics of living with stroke as a younger person are different from those of an older adult, as the impact of stroke on the life of a younger person is sometimes invisible and could impact other outcomes (Lawrence 2010). Disorientation, life (social and psychological) disruption and change in roles and relationships are three main themes identified in a qualitative systematic review of experiences of young adults post-stroke (Lawrence 2010). Other themes identified from the literature include – loss of valued activities (recreation and employment) (Kuluski et al. 2014) and loss of pre-stroke life construct and relationships (Shipley et al. 2018). Navigating life as a young adult post-stroke can be challenging, and the burden could increase in a community with a high potential to stigmatise people living with disability (Trani et al. 2020). An understanding of the contextualised burden of living with stroke as a young person in a low-income community in South Africa could help in mapping out potential strategies to mitigate the challenges associated with living with stroke as a young person, which could improve psychological outcomes.
No stroke survivor fully achieved the return-to-work goal at discharge. South Africa is grappling with high unemployment rates (Stats SA 2023), which presents a challenge for people living with disabilities to get jobs as available work opportunities are dwindling. The rate of return to work among stroke survivors ranges from 12%–64% in various populations (Baldwin & Brusco 2011; Olaoye, Soeker & Anthea 2021). In a randomised controlled trial conducted in South Africa, after a workplace intervention programme, 60% (n = 24) of stroke survivors in the intervention group returned to work compared to 20% (n = 8) in the control group. In this case series, the stroke survivors who did not return to work, unwillingness by old employers to employ them, as well as cognitive, psychological and functional challenges, were the primary reasons (Ntsiea et al. 2015). All the stroke survivors of our programme found that returning to their previous jobs was challenging because of their disabilities, and therefore, they would require skill adaptation to seek employment.
Furthermore, the individual and community understanding of the dynamics of disability and ability was a challenge. There was a sense of incapacitation associated with living with a disability at the individual level and a community approach to people with disabilities, which hindered their ability and desire to return to work. Despite participants’ willingness to return to work, their family members sometimes did not encourage it, and the wider community questioned their cognitive and physical capacity to work. Additionally, previous employers are not willing to accommodate people with disabilities. A study conducted in a similar community in Soweto as our study showed that there is stigmatisation of people living with disabilities which can be seen in the higher levels of unemployment, which increases the risk of depression and low self-esteem (Trani et al. 2020). In people living with disabilities, being unemployed and having no education increase the risk of depression (Trani et al. 2020). Trani et al. (2020) recommend community engagement with people living with disabilities while providing psychosocial support and enacting anti-stigma policies.
Recommendations
The ongoing promotion and facilitation of independence of the stroke survivors as they progress through their rehabilitation journey needs to be reinforced from admission and not just as FIM goals are achieved. As such, it is recommended to have follow-up sessions and check-ins post-discharge. In addition, all stroke survivors are encouraged to continue the support groups post-discharge from the formal programme. In future, meetings with the stroke survivor beneficiary manager and rehabilitation team should include the stroke survivor to ensure that the process is as person-centred as possible. An important learning point of our study was the stroke survivors’ return-to-work journey and the factors that negatively influenced their return to work. Return-to-work options should be considered by therapists and stroke survivors on admission and not only towards the end of the programme as this would allow more time to consider re-employment and reskilling opportunities before discharge. Partnering with business-oriented organisations that could assist with self-employment and business support would better support stroke survivors’ return-to-work goals.
Conclusion
The individualised PSWI BBJ rehabilitation programme, which uses public–private partnerships to rehabilitate people with disabilities, has shown positive functional outcomes in an economically marginalised community. However, to further strengthen the programme, partnerships with business-oriented organisations to improve the return-to-work outcome would benefit the stroke survivors’ quality of life.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alessandro, L., Olmos, L.E., Bonamico, L., Muzio, D.M., Ahumada, M.H., Russo, M.J. et al., 2020. [Multidisciplinary rehabilitation for adult patients with stroke]. Medicina (B Aires) 80, 54–68.32044742 · pubmed ↗
- 2Andresen, E.M., Malmgren, J.A., Carter, W.B. & Patrick, D.L., 1994, ‘Screening for depression in well older adults: Evaluation of a short form of the CES-D’, American Journal of Preventive Medicine 10(2), 77–84. 10.1016/S 0749-3797(18)30622-68037935 · doi ↗ · pubmed ↗
- 3Baldwin, C. & Brusco, N.K., 2011, ‘The effect of vocational rehabilitation on return-to-work rates post stroke: A systematic review’, Topics in Stroke Rehabilitation 18(5), 562–572. 10.1310/tsr 1805-56222082705 · doi ↗ · pubmed ↗
- 4Baron, E.C., Davies, T. & Lund, C., 2017, ‘Validation of the 10-item centre for epidemiological studies depression scale (CES-D-10) in Zulu, Xhosa and Afrikaans populations in South Africa’, BMC Psychiatry 17, 1–14. 10.1186/s 12888-016-1178-x 28068955 PMC 5223549 · doi ↗ · pubmed ↗
- 5Ekman, I., Swedberg, K., Taft, C., Lindseth, A., Norberg, A., Brink, E. et al., 2011, ‘Person-centered care—Ready for prime time’, European Journal of Cardiovascular Nursing 10(4), 248–251. 10.1016/j.ejcnurse.2011.06.00821764386 · doi ↗ · pubmed ↗
- 6Feigin, V.L., Stark, B.A., Johnson, C.O., Roth, G.A., Bisignano, C., Abady, G.G., Abbasifard, M. et al., 2021, ‘Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019’, The Lancet Neurology 20(10), 795–820. 10.1016/S 1474-4422(21)00252-034487721 PMC 8443449 · doi ↗ · pubmed ↗
- 7Gao, C., Li, X., Li, F., Li, J. & Zhang, J., 2024, ‘Non-pharmacological interventions on quality of life in stroke survivors: A systematic review and meta-analysis’, Worldviews on Evidence-Based Nursing 21(2), 158–182. 10.1111/wvn.1271438429872 · doi ↗ · pubmed ↗
- 8Hartley, T., Burger, M. & Inglis-Jassiem, G., 2022, ‘Post stroke health-related quality of life, stroke severity and function: A longitudinal cohort study’, African Journal of Disability (Online) 11, 1–10. 10.4102/ajod.v 11i 0.947PMC 883192235169551 · doi ↗ · pubmed ↗