From Nature to Emergency: Cardiac Complications Following the Consumption of Unwashed Fruit
Mahmoud J. Tabouni, Anas AbuRamadan, Samah Awouda

TL;DR
A man experienced severe heart issues after eating unwashed Ziziphus spina-Christi fruit, possibly due to toxicity or pesticide exposure.
Contribution
This case highlights the potential cardiotoxic effects of unwashed Z. spina-Christi fruit and pesticide exposure.
Findings
A 25-year-old male developed bradycardia and hypotension after consuming unwashed Z. spina-Christi fruit.
Cardiac evaluations ruled out ischemic or structural causes, suggesting toxicity as the likely cause.
The patient recovered with supportive care, indicating reversible cardiotoxic effects.
Abstract
Ziziphus spina-Christi (Sidr) is widely used for its medicinal and nutritional properties, with documented pharmacological effects such as antidiabetic, sedative, and antihypertensive activities. However, its consumption, especially in unregulated settings, can pose significant health risks due to potential toxicity and contamination with pesticides. We report the case of a 25-year-old male who presented with severe abdominal pain radiating to the chest, profound bradycardia (heart rate in the 20s), hypotension (systolic blood pressure in the 50s), and autonomic symptoms after ingesting unwashed Z. spina-Christi fruit. Initial investigations revealed Mobitz type I second-degree atrioventricular (AV) block, transient ST depression, and elevated troponin levels, raising suspicion of acute coronary syndrome (ACS). However, comprehensive cardiac evaluations, including CT coronary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
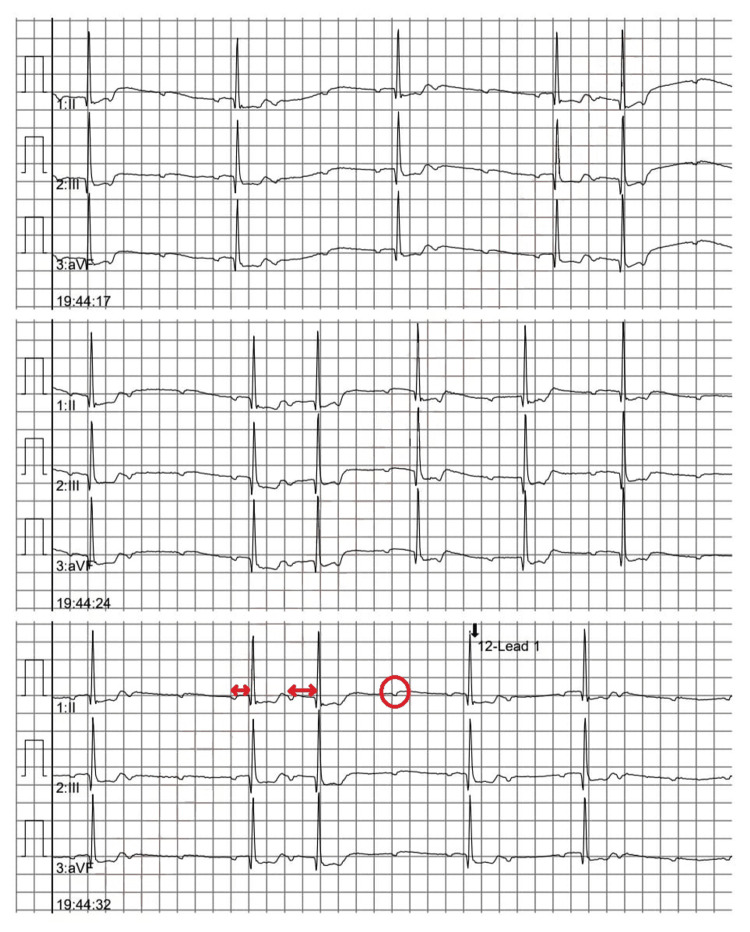 Figure 1
Figure 1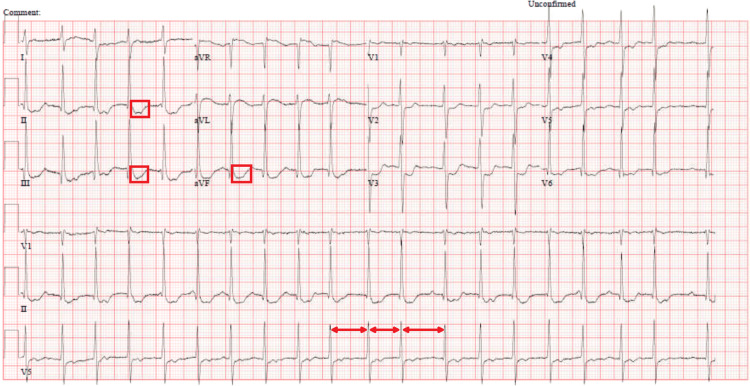 Figure 2
Figure 2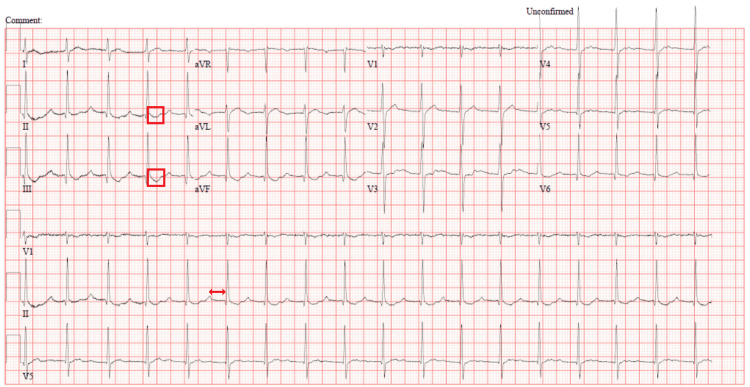 Figure 3
Figure 3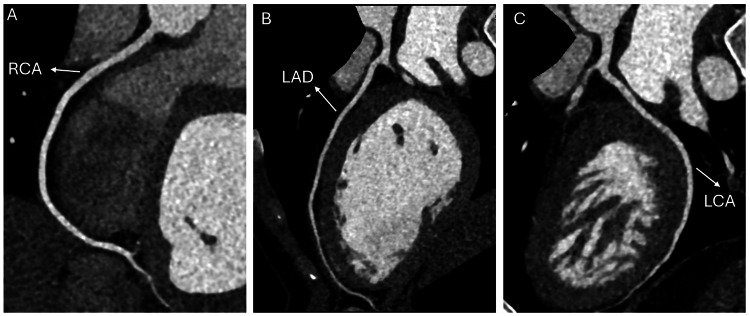 Figure 4
Figure 4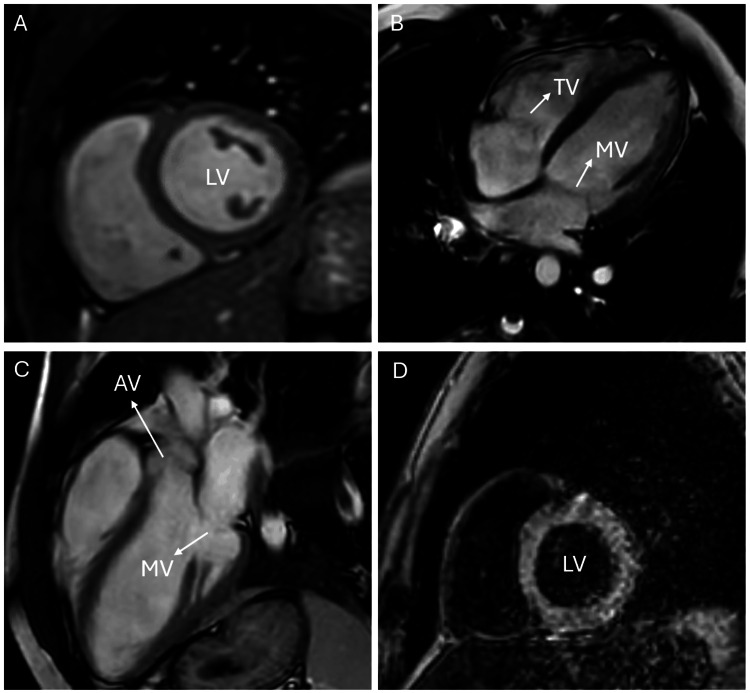 Figure 5
Figure 5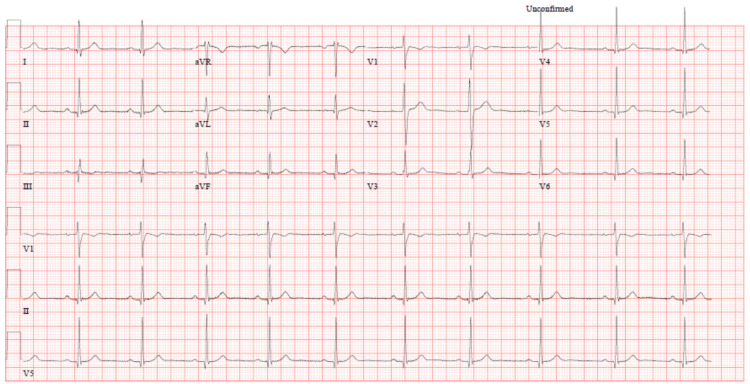 Figure 6
Figure 6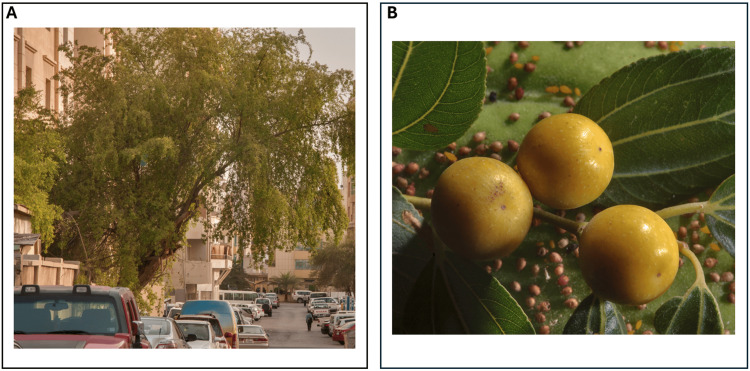 Figure 7
Figure 7| Findings: | |
| Left Ventricle | Normal size left ventricle. Normal global systolic LV function. Biplane LVEF is calculated at 60%. No regional wall motion abnormality. Normal diastolic LV function. Normal left ventricular wall thickness. |
| Right Ventricle | Normal size right ventricle. Normal RV function. |
| Left Atrium | The left atrium is normal in size. |
| Right Atrium | The right atrium is normal in size. |
| IVS | Normal thickness. |
| Mitral Valve | Normal morphology and function. |
| Aortic Valve | Normal morphology and function. |
| Tricuspid Valve | Normal morphology and function. |
| Pulmonic Valve | Normal morphology and function. |
| Aorta | Normal. |
| Pericardium | No pericardial effusion. |
| Parameter | Result (Admission) | Reference Range |
| Hs-TnT | 22 ng/L | <14 ng/L |
| TSH | 0.90 mIU/L | 0.4–4.2 mIU/L |
| Lactic acid | 4.3 mmol/L | 0.5–2.2 mmol/L |
| Cr | 116 μmol/L | 44–106 μmol/L (male) |
| CK | 180 U/L | 25–200 U/L |
| Mb | 134 ng/mL | 28–72 ng/mL |
| K | 5.6 mmol/L | 3.5–5.1 mmol/L |
| Findings | |
| Origin and course of the left and right coronary circulation | Normal. |
| Dominant artery | Right coronary artery. |
| Ca score | 0. |
| LMA | Normal. |
| LAD | Normal, no evidence of stenotic lesion seen. |
| First diagonal branch | Normal. |
| LCX | Normal, no evidence of stenotic lesion seen. |
| RI | Normal, no evidence of stenotic lesion seen. |
| RCA | Normal, no evidence of stenotic lesion seen. |
| Parameter | Value | Normal Range | Additional Notes |
| Total QRS Complexes | 78,945 | - | - |
| Maximum Heart Rate (HR) | 94 bpm | 60–100 bpm | Average for 1 minute |
| Minimum Heart Rate (HR) | 45 bpm | 60–100 bpm | Average for 1 minute |
| Average Heart Rate (HR) | 61 bpm | 60–100 bpm | - |
| Ventricular Ectopic Beats | 0 (0.00%) | 0–50 beats/day | - |
| Supraventricular Ectopic Beats | 73 (0.09%) | 0–100 beats/day | - |
| Time Classified as Noise | 0.00% | <5% | - |
| Beats in Tachycardia (>100 bpm) | 28 (0.04%) | 0–50 beats/day | - |
| Beats in Bradycardia (<60 bpm) | 40,634 (51.47%) | 0–50 beats/day | - |
| AFIB Episodes | 0 | 0 | No atrial fibrillation episodes detected |
| AFIB Burden | 0.00 minutes (0.00%) | 0 minutes | - |
| Max R-R Interval | 1.64 seconds | <2 seconds | - |
| Supraventricular Ectopy | 0.09% | 0–0.1% | - |
| Ventricular Ectopy | 0.00% | 0–0.1% | - |
| Isolated Supraventricular Beats | 38 | 0–50 beats/day | - |
| Supraventricular Couplets | 1 | 0–10/day | - |
| Supraventricular Triplets | 0 | 0–5/day | - |
| Supraventricular Bigeminal Cycles | 2 | 0–5 cycles/day | - |
| Supraventricular Runs (≥4 beats) | 6 runs totaling 33 beats | 0–10 runs/day | 0% of total beats |
| Longest Supraventricular Run | 7 beats | <10 beats | 74 bpm |
| Fastest Supraventricular Run | 6 beats | <10 beats | 77 |
| Tachycardia Episodes (≥3 beats at ≥120 bpm) | 0 | 0 | No episodes detected |
| Tachycardia Episodes (≥4 beats at ≥80 bpm) | 0 | 0 | No episodes detected |
| Bradyarrhythmia Pauses (>2.00 seconds) | 0 | 0 | No pauses detected |
| N-N Delays (>140%) | 64 | <100 delays/day | - |
| Parameter | Finding | Normal Range | Comments |
| LV | |||
| LV (EF) | 56% | 57–77% | Slightly below normal range, not clinically significant |
| LVEDD | 5.3 cm | ≤5.6 cm | Normal |
| Wall Thickness (Max) | 8 mm | ≤10 mm | Normal |
| Regional Wall Motion | No abnormalities | No abnormalities | Normal |
| RV | |||
| RV (EF) | 50% | 47–67% | Normal |
| RVEDD | 4.2 cm | Normal for body size | Normal |
| LA | |||
| LA Area | 17.1 cm² | ≤20 cm² | Normal |
| RA | |||
| RA Area | 20.4 cm² | ≤22 cm² | Normal |
| Valves | No abnormalities | No abnormalities | Normal |
| Pericardium | Normal | No effusion | Normal |
| T2WI | No myocardial edema | None | Normal |
| Native T1 Mapping | 959 ms | 965–1055 ms | Slightly below normal, not clinically significant |
| Native T2 Mapping | 44 ms | 50–55 ms | Slightly below normal, not clinically significant |
| Post-Gadolinium Imaging | |||
| Early Phase | No LV/RV thrombus | None | Normal |
| Late Phase | No myocardial enhancement | None | No infarction or overt fibrosis |
| Left Ventricle Indexed Quantitative Parameters | |||
| LV (EDV) | 104 ml/m² | 68–112 ml/m² | Normal |
| LV (ESV) | 46 ml/m² | 16–44 ml/m² | Slightly above normal, not clinically significant |
| SI | 58 ml/m² | 44–76 ml/m² | Normal |
| Myocardial Mass (End-Diastole) | 55 g/m² | 47–87 g/m² | Normal |
| Right Ventricle Indexed Quantitative Parameters | |||
| RV (EDV) | 108 ml/m² | 74–134 ml/m² | Normal |
| RV (ESV) | 54 ml/m² | 25–62 ml/m² | Normal |
| SI | 54 ml/m² | 41–77 ml/m² | Normal |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin C and Antioxidants Research
Introduction
The use of plants as food and remedies for various health conditions dates back to ancient times, yet only a limited number of these plants have been studied scientifically [1]. Although often perceived as less harmful than synthetic drugs, there is limited information on the toxicity of plants and herbal products [2]. This belief may be misguided, as many plants previously considered completely harmless have been scientifically proven to cause various adverse effects on living organisms [3]. Ziziphus spina-Christi, known as Sidr (Arabic), is thought to have originated from Sudan and grows in various regions throughout the world, especially the tropics [4]. Parts of Z. spina-Christi have been reported to have pharmacological effects such as antidiabetic, anti-nociceptive, central nervous system (CNS) modulating and antimicrobial activities [5]. The fruits of this plant have been reported for their antioxidant properties, while its seeds are recognized for their sedative effects [6, 7]. The flower, leaf and fruit of Z. spina-Christi are effective for controlling and treating hypertension [8]. Although this plant offers notable medical benefits, other studies emphasize the need for caution in its consumption due to potential adverse effects on vital organs caused by components like tannins, saponins, alkaloids, flavonoids, phenols and glycosides [9]. In this case report, we highlighted the potential cardiac effects of this fruit, exacerbated by the additional impact of pesticide exposure on the human body. After reviewing the literature, organophosphates were identified as the most commonly used pesticides in the region, and it is plausible that this type of pesticide contributed significantly to the patient’s clinical presentation [10]. Organophosphate exposure could have worsened the observed bradycardia, hypotension, and autonomic symptoms, amplifying the potentially suspected toxic effects of Z. spina-Christi. This observation underscores the importance of assessing both natural and environmental factors in toxicological cases.
Case presentation
A 25-year-old male, a non-smoker with no significant medical or surgical history, presented to the Emergency Department (ED) at Heart Hospital in Doha, Qatar. The patient had an acute abdominal pain radiating to the chest, described as severe (9 out of 10 on a numerical rating scale) burning sensation. The patient sought help 20 minutes after the onset of pain, and emergency medical services (EMS) arrived 10 minutes later. The patient reported concurrent symptoms of sweating and shortness of breath followed by two episodes of vomiting, each consisting of a small amount of normal gastric contents, blurred vision and dizziness. The patient denied any fever, syncope, or loss of consciousness.
Upon arrival of EMS, the patient was noted to be profoundly bradycardic, with a heart rate of 23 beats per minute (bpm), and hypotensive, with a systolic blood pressure of 56 mmHg. EMS initiated resuscitation, administering an epinephrine infusion 1 microgram per minute, ketamine 200 mg, and temporary transcutaneous pacing. Initial electrocardiogram (ECG) in the ED showed a Mobitz Type I second-degree atrioventricular (AV) block (Figure 1). Shortly (15 minutes) after receiving 1 mg of atropine in ED, the patient developed atrial fibrillation with rapid ventricular response, accompanied by transient, marked ST depression in leads II and III noticed on the monitor and confirmed with ECG (Figure 2). Then ECG was repeated after 10 minutes due to a change in rhythm on the monitor and showed sinus tachycardia at 105 bpm with a first-degree AV block and nonspecific ST and T wave abnormalities (ST depression and T wave inversion) (Figure 3). He then reported a significant reduction in chest pain after it had persisted for a total duration of three hours.
Mobitz type IMobitz Type I (Wenckebach) second-degree atrioventricular (AV) block. This rhythm is characterized by a progressive prolongation of the PR interval (marked with arrows) until a QRS complex is dropped (indicated by circle). The ECG demonstrates this classic Wenckebach pattern in leads II, III, and arteriovenous fistula (aVF).
Atrial fibrillation with rapid ventricular responseThis ECG shows irregularly irregular heart rate (marked with arrows) with no P waves and a rapid ventricular response (heart rate 120); there is also a marked ST depression in leads II and III (indicated by squares). These changes strongly indicate myocardial ischemia.
Tachycardia and first-degree atrioventricular blockSinus tachycardia (heart rate 105 beats per minute) with a first-degree atrioventricular (AV) block (indicated by arrow) and nonspecific ST and T wave abnormalities (highlighted with squares). The ECG findings correspond to transient electrical and repolarization disturbances seen in the patient during acute presentation.
Upon further review of the patient’s history, he reported no known allergies, recent travel, or toxic exposures. His family history was notable for coronary artery disease in his father, diagnosed at the age of 57. Additionally, the patient’s body mass index (BMI) was 23, indicating a normal weight range.
On examination, the patient appeared drowsy, pupils were constricted (2-3 mm) but reactive to light, with otherwise unremarkable neurological, respiratory and cardiovascular findings, except for tachycardia. Other investigations included a transthoracic echocardiogram (Table 1, Video 1), which showed normal cardiac function. Laboratory results at admission are shown in Table 2. A urine drug screen was negative for amphetamines, cannabinoids, cocaine, opiates and phencyclidine. The patient was admitted for continuous cardiac monitoring, intravenous fluids (65 mL/hour and he received total 3 liters during his admission), and serial (every 6 hours then daily) troponin measurements to rule out acute coronary syndrome (ACS).
Transthoracic EchocardiographyRA: right atrium, LA: left atrium, RV: right ventricle, LV: left ventricle.This echocardiography four-chamber view reveals normal chamber sizes and normal global systolic left ventricular (LV) function, with no evidence of regional wall motion abnormalities.
Repeated lab tests (troponin after 6 hours, and other labs after 24 hours) showed a rising trend in troponin levels (initially 22 ng/L, peaking at 176 ng/L), alongside elevated lactic acid (3 mmol/L), creatinine (83 μmol/L), and potassium (5.1 mmol/L). These findings, coupled with ECG abnormalities, raised suspicion for acute coronary syndrome (ACS) and hypoperfusion, prompting further investigations. A CT coronary angiogram (Table 3, Figure 4) and 24-hour Holter monitoring (Table 4) revealed no abnormalities, and cardiac MRI (Table 5, Figure 5) excluded myocarditis or structural heart disease. By the third day, troponin levels had normalized, and ECG findings had resolved (Figure 6).
CT Cardiac angiogram coronaryNormal origins and courses of right coronary artery (RCA) (A), left anterior descending artery (LAD) (B) and left circumflex artery (LCA) (C) with no stenosis or filling defects.
MRI Cardiac morphology functionMultiple planes in cardiac MRI showing normal appearances. (A) The short-axis view shows no (LV) left ventricular wall abnormalities (B) The four-chamber view shows normal (MV) mitral and (TV) tricuspid valves (C) The left ventricular outflow tract view shows normal (AV) aortic and (MV) mitral valves. (D) The Post contrast short-axis view shows normal enhancement pattern.
Normal ECGNormal ECG recorded on the third day of admission. No abnormalities in rhythm, conduction, or repolarization are observed, indicating resolution of the transient cardiac disturbances associated with intoxication.
During further history-taking, the patient and his friend disclosed that he had ingested multiple unwashed Sidr (Z. spina-Christi) fruits (Figure 7) from a street tree 1-2 hours before symptom onset. This history, combined with the patient’s bradycardia, hypotension, abdominal and chest pain, and significant improvement with supportive measures, strongly suggests poisoning from a Z. spina-Christi-derived substance, potentially exacerbated by pesticide exposure.
Sidr (Ziziphus spina-Christi) tree and Fruits(A) Large Sidr tree (Ziziphus spina-Christi) on Al Khattabi Street, Al Doha Al Jadeeda area, Doha, Qatar. (B) Fruits of Christ's thorn jujube (Sidr tree, Ziziphus spina-Christi) collected near Dareen Tower in West Bay, Doha, Qatar.Image source: Flora of Qatar. (n.d.). Ziziphus spina-Christi. Retrieved January 13, 2025, from https://www.floraofqatar.com/ziziphus_spina-christi.htm. Used with permission from the website administrator Alexey Sergeev.
The toxicology team reviewed the case and concluded that the diagnosis could be confidently established based on the exposure history, clinical findings and ruling out other causes like structural abnormality, ischemic heart disease, arrhythmogenic syndromes or myocarditis through unremarkable CT angiogram, Holter monitoring and cardiac MRI findings support the diagnosis of transient, reversible etiology like plant toxicity. They did not recommend further diagnostic tests, given the patient’s marked improvement and the lack of specific confirmatory tests for Z. spina-Christi toxicity or organophosphate toxicity (red blood cell acetylcholinesterase activity test is not available in our facility).
The patient’s condition improved, and he was discharged home on the fourth day of hospitalization with normal ECG and troponin levels, and no residual symptoms. We advised him to avoid any future ingestion of unwashed or unfamiliar street fruit, and a follow-up appointment was scheduled for the patient; however, unfortunately, he did not turn up for the appointment. This case underscores the pivotal role of detailed history-taking in identifying toxic ingestions. Poisoning should be considered in cases presenting with cardiovascular and gastrointestinal symptoms resembling acute coronary syndrome, especially when there is a history of possible exposure. Prompt recognition and treatment can lead to significant clinical improvement and saving life.
Discussion
This case highlights the diagnostic challenges in a young, otherwise healthy patient with a combination of gastrointestinal, cardiac, and autonomic symptoms. Initially, the focus was on ACS due to elevated troponin levels and ECG abnormalities, a common diagnostic approach in emergency settings [11]. However, further investigation revealed an atypical toxicological etiology.
The patient presented with severe bradycardia (heart rate in the 20s) and hypotension (systolic blood pressure in the 50s), prompting urgent interventions, including adrenaline infusion, transcutaneous pacing, and atropine administration for stabilization [12]. Such profound bradycardia typically suggests serious underlying conditions, such as myocarditis, cardiovascular pathology, or the effects of pharmacologic agents [13].
ECG findings showed Mobitz Type I second-degree AV block, which later evolved into atrial fibrillation with transient ST depression in the inferior leads, can be related to the treatment that patient received, especially atropine [14]. Elevated troponin-T levels (initially 22 ng/L, rising to 176 ng/L) suggested myocardial injury; as a result, ACS was initially suspected. However, both coronary CT angiography and 24-hour Holter monitoring were unremarkable, effectively ruling out ischemic causes and persistent arrhythmias. Additionally, transthoracic echocardiography and cardiac MRI revealed no myocarditis, stress-induced cardiomyopathy (Takotsubo cardiomyopathy) or structural abnormalities, leading clinicians to consideration of alternative explanations [12, 13, 15].
A critical clue emerged when the patient reported ingesting unwashed Sidr (Z. spina-Christi) from a street tree two hours prior to symptom onset. This history, combined with the signs and symptoms of bradycardia, hypotension, abdominal pain, miosis, a positive response to supportive treatment, and the rapid resolution of symptoms, strongly suggested toxicity as a likely cause. By reviewing the literature, we found that Z. spina-Christi fruit is well established to be toxic at higher doses, causing significant alterations in liver and renal function tests, as well as histological changes in the liver [16, 17]. Research conducted on frogs has shown that cardiac effects due to Z. spina-Christi can range from bradycardia to cardiac arrest, depending on the ingested dose of the plant [18]. The ingestion of unwashed fruit raises the possibility of pesticide exposure as a contributing factor that may have amplified the patient's clinical presentation including the elevated troponin [19]. Pesticide toxicity, including organophosphate poisoning, is unlikely to be the sole cause of this patient's presentation, although some cholinergic effects such as bradycardia, abdominal pain and miosis were observed. Key features of severe organophosphate toxicity - such as unresponsiveness, muscle fasciculations, diarrhea, excessive salivation, lacrimation, and urinary incontinence - were absent, and the patient's heart rate improved significantly with a single dose of atropine, while severe organophosphate poisoning typically requires pralidoxime and multiple doses of atropine for stabilization [20].
Conclusions
This case highlights the importance of detailed history-taking and a high index of suspicion when evaluating patients presenting with a combination of cardiovascular, gastrointestinal, and autonomic symptoms. The ingestion of unwashed Z. spina-Christi fruit, likely contaminated with pesticides, was the probable cause of the patient's profound bradycardia, hypotension, and elevated troponin levels, which initially mimicked acute coronary syndrome. The patient's symptoms resolved with supportive care, including atropine administration and cardiac monitoring, emphasizing the importance of prompt recognition and management of plant poisoning.
The future implications of this study are as follows: (1) Further research is needed to identify the specific compounds in Z. spina-Christi responsible for its toxic effects on the heart and to understand the mechanisms of action, particularly in combination with contaminants like pesticides. (2) Educational campaigns should emphasize proper cleaning techniques for fruits and vegetables, such as rinsing under running water, scrubbing tough skins, and soaking delicate produce. These efforts can reduce the risk of toxin or pesticide exposure. (3) Stronger policies on pesticide regulation, residue testing, and farmer education are critical to minimize contamination risks. Authorities should monitor pesticide use and promote safer agricultural practices. (4) Hospitals should equip themselves with tools like plant toxin assays and red blood cell cholinesterase testing to better diagnose and manage plant and pesticide-related toxicities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Status of conservation of the indigenous leaf vegetables and fruits of Africa African Journal of Biotechnology Adebooye OC Opabode JT 70070532004 https://www.ajol.info/index.php/ajb/article/view/15041
- 2Current uses and knowledge of medicinal plants in the autonomous Community of Madrid (Spain): a descriptive cross-sectional study BMC Complement Med Ther Sánchez M González-Burgos E Iglesias I Lozano R Gómez-Serranillos MP 3062020203305474010.1186/s 12906-020-03089-x PMC 7557077 · doi ↗ · pubmed ↗
- 3Comparison of medicinally important natural products versus synthetic drugs - a short commentary Nat Prod Chem Res Nisar B Sultan A Rubab SL 100030862017
- 4Studies on in-vitro antioxidant and free radical scavenging potential and phytochemical screening of leaves of Ziziphus mauritiana L. and Ziziphus spinachristi L. compared with Ascorbic acid J Med Genet Genomics Abalaka ME Mann A Adeyemo SO 283432011 https://www.researchgate.net/publication/285777021_Studies_on_in_vitro_antioxidant_and_free_radicals_scavenging_potential_and_phytochemical_screening_of_leaves_of_Ziziphusmauritiana_L_and_Ziziphusspinachristi_L_compared_with_ascorbic_acid
- 5Anti-diabetic activity and stability study of the formulated leaf extract of Zizyphus spina-christi (L.) Willd with the influence of seasonal variation J Ethnopharmacol Michel CG Nesseem DI Ismail MF 536213320112083323610.1016/j.jep.2010.09.001 · doi ↗ · pubmed ↗
- 6In vitro antioxidant activities of Ziziphus spina-christi fruits (red date) grown in Oman Biotechnology Singh V Guizani N Essa MM Rahman MS Selvaraju S 209216112012
- 7Analysis of phenolic compounds in extracts of Ziziphus spina-christi using RPHPLC method J Chem Pharm Res Ghafoor AO Qadir HK Fakhri NA 3158316342012 https://www.jocpr.com/articles/analysis-of-phenolic-compounds-in-extracts-of-ziziphus-spinachristi-using-rphplc-method-1579.html
- 8A mini-review on the most important effective medicinal plants to treat hypertension in ethnobotanical evidence of Iran J Nephropharmacol Baharvand-Ahmadi B Asadi-Samani M 3862016 https://pmc.ncbi.nlm.nih.gov/articles/PMC 5295656/pdf/npj-6-3.pdf 28197520 PMC 5295656 · pubmed ↗