Left Atrial Mitral Valve Chordae Which Disturbed the Mitral Leaflet Motion and Induced Mitral Regurgitation
Toru Kameda, Tomohiro Mizuno, Kota Kawada, Tsubasa Yoshikawa, Koichi Sugiyama, Yuzo Katayama, Takeshiro Fujii

TL;DR
A rare heart condition called left atrial mitral valve chorda can cause mitral regurgitation by restricting leaflet motion.
Contribution
This case report describes a novel presentation of LAMVC originating from a papillary muscle and causing mitral regurgitation.
Findings
LAMVC can originate from a papillary muscle and attach to the posterior mitral annulus.
The abnormal chorda restricts mitral leaflet motion, leading to mitral regurgitation.
Abstract
Left atrial mitral valve chorda (LAMVC) is a rare congenital cardiac anomaly. The abnormal tissue band, like a mitral valve chorda, is attached to the left atrial wall on one side and mostly to the mitral valve leaflet on the other side and the band sometimes disturbs the mitral leaflet motion, followed by mitral regurgitation (MR). We encountered a case with a LAMVC which originated from a papillary muscle and attached to the posterior mitral annulus over the posterior leaflet and caused MR due to restricted mitral leaflet motion.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
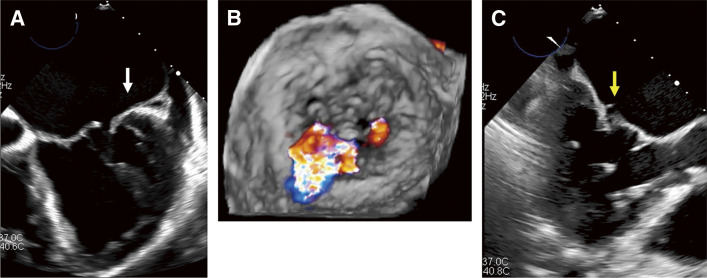 Fig. 1
Fig. 1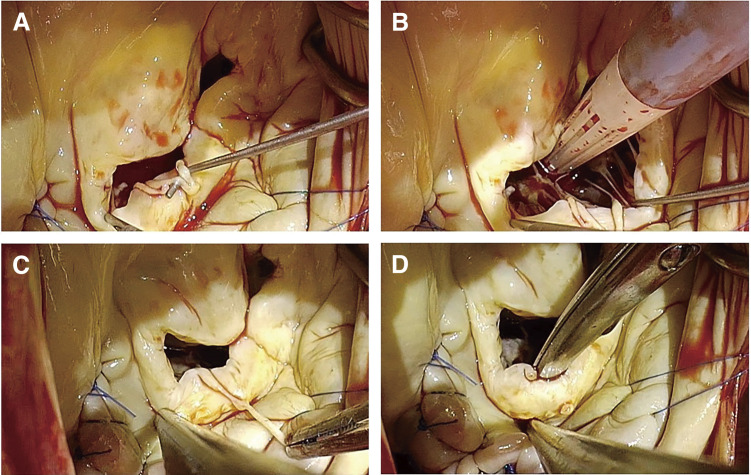 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiovascular Function and Risk Factors · Cardiac Arrhythmias and Treatments
Abbreviations
LAMVC left atrial mitral valve chorda MR mitral regurgitation TEE transesophageal echocardiography AFMR atrial functional mitral regurgitation TR tricuspid regurgitation
Introduction
Left atrial mitral valve chorda (LAMVC) is a rare congenital cardiac anomaly. The abnormal tissue band, like a mitral valve chorda, is attached to the left atrial wall on one side and mostly to the mitral valve leaflet on the other side and the band sometimes disturbs the mitral leaflet motion, followed by mitral regurgitation (MR).^1)^ Pizzuti et al.^2)^ reported an incidence of 0.02% among approximately 30000 unselected echocardiogram cases. We encountered a case with a LAMVC which caused MR due to restricted mitral leaflet motion.
Case Report
A 76-year-old woman was admitted to our hospital with progressive dyspnea. She had chronic atrial fibrillation in her history. Her transesophageal echocardiography (TEE) showed severe atrial functional MR (AFMR) and tricuspid regurgitation (TR) with restricted movement of the lateral P2 leaflets, followed by MR (Figs. 1A and 1B). We could not recognize an abnormal tissue on the mitral valve at this point.
Preoperative transesophageal echocardiographic images. (A) Movement of the posterior mitral leaflet was restricted (white arrow). (B) A surgeon’s view. The mitral regurgitant jet came from the anterolateral P2 area. (C) An abnormal tissue appeared and disappeared on the posterior mitral leaflet along with the heart beating (yellow arrow).
The mitral valve was exposed via median sternotomy. In the operative field, an abnormal band ran over the posterior mitral leaflet (Video 1). The band was attached to the posterior mitral leaflet near the annulus on one side and split into 2 parts (Fig. 2A). One part was attached to the edge of the posterior leaflet, and the other one to a small papillary muscle on the other side (Figs. 2B–2D). It was speculated that the band pushed down the anterolateral P2 in the systolic phase and restricted leaflet movement, which might have worsened AFMR. The LAMVC was cut off and a pair of artificial chordae was placed at the anterior mitral leaflet, and a rigid ring was placed for annuloplasty. MR was reduced to trivial, and the movement of the posterior mitral leaflet improved. Postoperatively, after looking at the preoperative TEE images again, we recognized that an abnormal tissue appeared and disappeared along with the heartbeat (Fig. 1C). This was the LAMVC.
Intraoperative photographs of left atrial mitral valve chorda. (A) An abnormal band ran over the posterior mitral leaflet attached to the posterior mitral leaflet near the annulus and split into 2 parts. (B) One part was attached to the edge of the posterior mitral leaflet. (C) The other part was attached to a papillary muscle. (D) The posterior mitral leaflet after resection of the band.
Discussion
LAMVC is a rare congenital anomalous band, which looks like a mitral valve chorda. The band is attached to the left atrial wall on one side and mostly to the mitral valve leaflet on the other side.^1)^ Pizzuti et al.^2)^ reported an incidence of 0.02% among approximately 30000 unselected echocardiogram cases. The first report of LAMVC in 1947 described a band that bridged from the left atrial wall to the left atrial wall above the mitral valve and did not disturb the mitral valve function.^3)^ Reports of LAMVC have gradually increased with the progression of diagnostic technologies, and it has been recognized that the abnormal band sometimes causes MR, and surgical treatment is required.^4)^
In the case we described here, we did not recognize a LAMVC using TEE preoperatively, probably because the chorda was very slim and ran very close to the mitral valve. In addition, this case is exceedingly rare given that the chorda originated from the papillary muscle and ran over the posterior mitral leaflet to the posterior mitral annulus. The anomalous band disturbs coaptation in the systolic phase, resulting in a worsening AFMR.
Shirwaiker et al.^4)^ reported that tissue attached to the mitral leaflets is sometimes misdiagnosed as vegetation of endocarditis. If the anomaly is thoroughly understood, we can prevent misdiagnosis and unnecessary surgery.
Conclusions
We reported a case of LAMVC which was the cause of severe MR. A LAMVC is very rare, but the opportunity to detect the disease is increasing with the widespread of TEE. LAMVC should be more understood to prevent misdiagnosis and unnecessary surgery.
Declarations
Ethical approval
The Institutional Review Board approved the study protocol and publication of data on August 10, 2024 (IRB approval number: M24078).
Consent for publication
The patient provided informed written consent for the publication of the study data.
Funding
This work was not supported by any grants or funding.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author contributions
TK and TM performed clinical work, drafted the manuscript, and designed the figures. KK, KS, and TY collected data. TM, YK, and TF were involved in planning and supervising the work. All authors have read and agreed to the published version of the manuscript.
Disclosure statement
None declared.
Supporting Information
Supplementary videoIntraoperative video of the mitral valve.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bertrand PB Churchill TW Passeri JJ. A left atrial mitral valve chord. JACC Case Rep 2020; 2: 526–7.34317285 10.1016/j.jaccas.2019.11.079PMC 8298682 · doi ↗ · pubmed ↗
- 2Pizzuti A Mabritto B Casula M. Left atrial anomalous muscular band: case report, literature review, and role of three-dimensional echocardiography. J Cardiovasc Echogr 2023; 33: 51–4.37426708 10.4103/jcecho.jcecho_52_22PMC 10328128 · doi ↗ · pubmed ↗
- 3MC NAMARAWL Baker LCLA Costich K. Asymptomatic congenital anomaly of the heart: congenital muscular cord bridging walls of auricle above center of mitral valve. Am Heart J. 1947; 34: 288–90.20255274 10.1016/0002-8703(47)90299-8 · doi ↗ · pubmed ↗
- 4Shirwaiker A Goh HIS Cieslik LK Left atrial mitral valve chordae: an important congenital abnormality mimicking endocarditis on transthoracic cardiography-case report. Echocardiography 2023; 40: 1137–9.37646444 10.1111/echo.15680 · doi ↗ · pubmed ↗