Lingual Bronchogenic Cyst: A Case Report and Literature Review of a Rare Pathology
Boyu Ma, Qingcong Zeng, John Le, James Wicker, Kathlyn Powell

TL;DR
A rare case of a bronchogenic cyst on the tongue in a young boy is reported, along with a literature review.
Contribution
This case report adds to the limited literature on bronchogenic cysts occurring in the tongue.
Findings
Bronchogenic cysts on the tongue are extremely rare.
The case highlights the clinical and histological features of such a rare pathology.
Abstract
Choristomas are rare, benign embryonic tumors characterized by normal tissue appearing in abnormal sites. When lined with respiratory epithelium, they are classified as bronchogenic cysts. While these cysts most commonly occur in the mediastinum or other thoracic regions, their occurrence on the tongue is exceedingly rare. Here, we present the case of a four-year-old boy diagnosed with a bronchogenic cyst of the tongue, highlighting its clinical and histological features, diagnosis, and management, along with a review of the literature.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
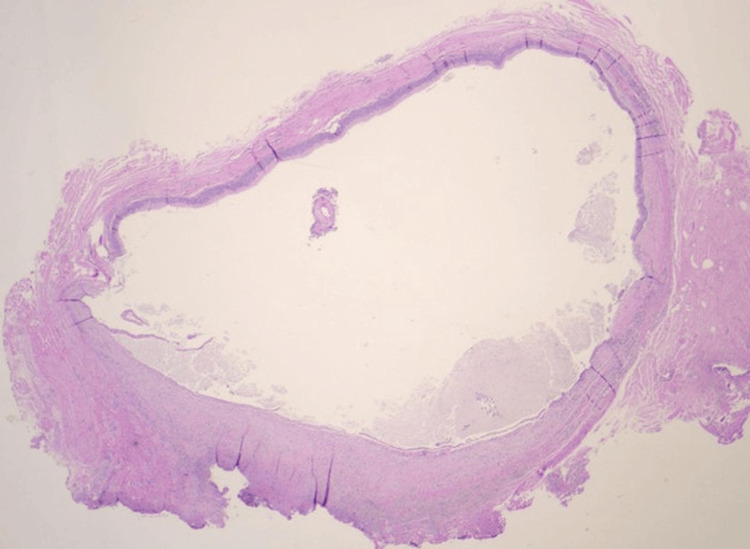 Figure 1
Figure 1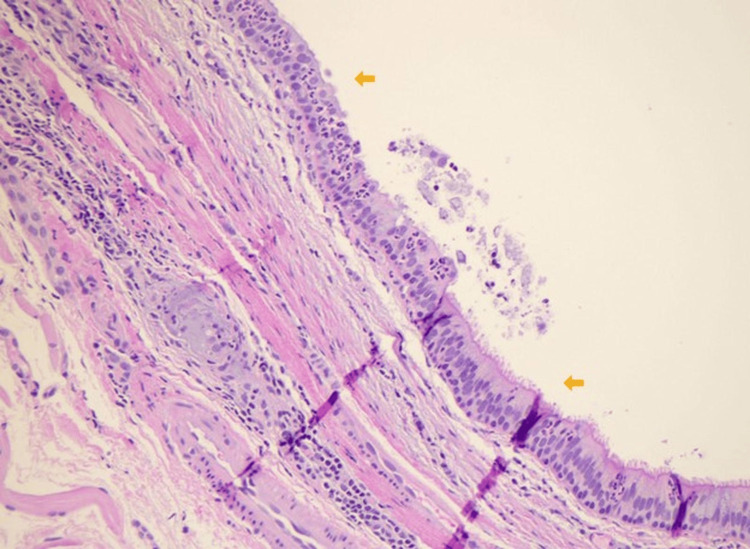 Figure 2
Figure 2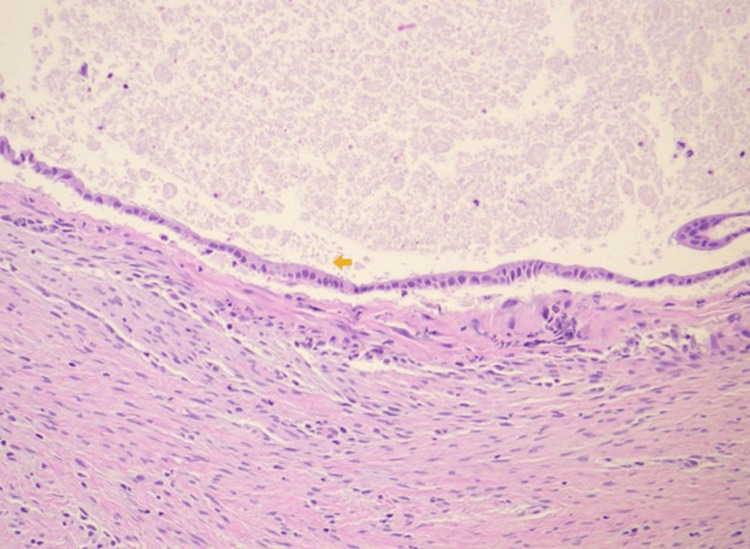 Figure 3
Figure 3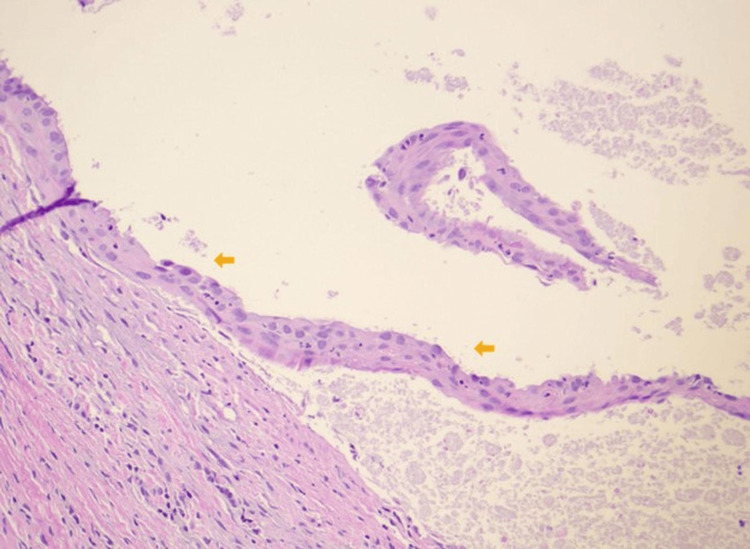 Figure 4
Figure 4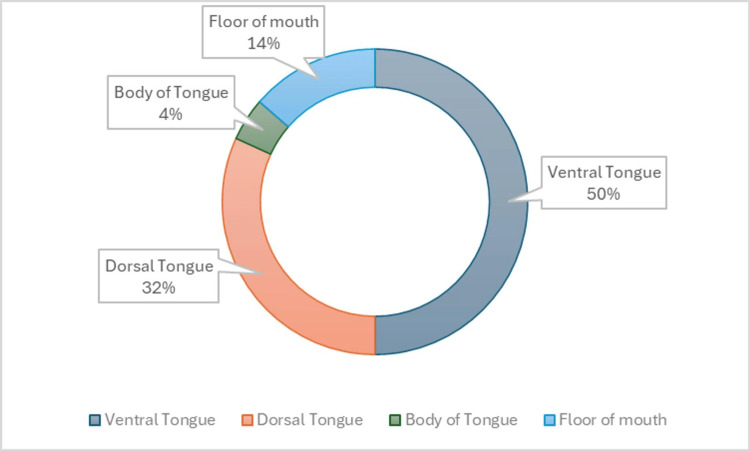 Figure 5
Figure 5| Author | Age | Sex | Site | Clinical history | Surgery |
| Gunnartodir et al. (2018) [ | 4 years old | Male | Ventral tongue | Asymptomatic | Excision |
| Bailey (1982) [ | 1 day old | Male | Ventral tongue | Present since birth, difficulty in eating | Excision |
| Aldawood et al. (2021) [ | 6 years old | Male | Ventral tongue | Asymptomatic | Excision |
| Joshi et al. (2013) [ | 6 years old | Male | Dorsal tongue | Asymptomatic | Excision |
| Kim et al. (1998) [ | 27 years old | Male | Dorsal tongue | Asymptomatic | Excision |
| Volchok et al. (2007) [ | 61 year old | Male | Ventral tongue | Transformation to adenocarcinoma | Excision |
| Fink (1963) [ | 5 years old | Male | Dorsal tongue | Painless swelling, difficulty in eating | Excision |
| Constatinides et al., (1982) [ | 9-month-old female | Female | Ventral tongue | Present since birth, difficulty in eating | Excision |
| Boue et al. (1994) [ | 4 years old | Male | Ventral tongue | Asymptomatic | Excision |
| Manor et al. (1999) [ | 11 years old | Male | Body of tongue | Macroglossia, difficulty in eating | Excision |
| Azanero et al. (2009) [ | 4 years old, 21 years, old | Male | Ventral tongue, Dorsal tongue | Present since birth, difficulty in breastfeeding, difficulty in eating | Excision |
| Boffano et al. (2009) [ | 35 years old | Female | Floor of mouth | Asymptomatic | Excision |
| Soares et al. (2011) [ | 12 years old | Female | Ventral tongue | Present since 6 years old, slow growth, difficulty in eating | Excision |
| Chai et al. (2011) [ | 6 months old | Female | Ventral tongue | Difficulty in eating | Excision |
| Juneja et al. (2011) [ | 1 year old | Female | Dorsal tongue | Present since birth, difficulty in eating | Excision |
| Fortier et al. (2013) [ | 17 years old | Female | Dorsal tongue | Asymptomatic | Excision |
| Kwak et al. (2014) [ | 2 years old | Female | Ventral tongue | Asymptomatic | Excision |
| Kün-Darbois et al. (2015) [ | 9 days old, 12 months old | Male and female | Dorsal tongue | Asymptomatic | Excision |
| Peters et al. (2018) [ | 10 years old, 27 years old | Male and female | Floor of mouth | Asymptomatic | Excision |
| Cialente et al. (2020) [ | 44 years old | Male | Floor of mouth | Present since 9 months old, swelling on the body of the tongue | Excision |
| Current case (2023) | 4 years old | Male | Ventral tongue | Present since birth | Excision |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTumors and Oncological Cases · Teratomas and Epidermoid Cysts · Tracheal and airway disorders
Introduction
Bronchogenic cysts are benign congenital lesions with normal tissue occurring in abnormal sites. They are part of a group of tumors called choristomas, heterotopic cysts, or foregut duplication cysts [1]. Choristomas can be histologically characterized based on their derivative tissue. Bronchogenic cysts are derived from the abnormal budding or branching of epithelial cells during the development of the tracheobronchial tree or associated vasculature. The majority of cases (>99%) occur in the mediastinum and lung, while extrathoracic sites are exceedingly rare [2,3]. Here, we describe a case of a lingual bronchogenic cyst arising in the ventral tongue of a four-year-old male. The cyst was completely excised, and no recurrence was seen at follow-up.
Case presentation
A healthy four-year-old male, with no prior medical history, presented with a two-week history of an enlarging tongue nodule on the ventral surface of his tongue. The nodule initially presented at birth without symptoms, but became enlarged and painful. On examination, a well-circumscribed, firm nodule was palpated at the midline ventral tongue with tenderness. The overlying mucosa had a purple tinge, but no other abnormalities were noted intraorally. The remaining oral and head and neck examination was without any remarks. No imaging modalities were utilized. Based on the clinical examination, the differential diagnosis included a branchial cyst, thyroglossal duct cyst, dermoid cyst, lipoma, and ranula. A total excisional biopsy of the mass was performed one week later under general anesthesia.
Intraoperative findings showed a cystic mass that was successfully dissected circumferentially and removed in its entirety from the underlying tongue musculature. Primary closure was achieved following the removal of the mass. The patient had an uneventful recovery and was discharged home on the same day as the surgery.
The gross specimen was gray-pink, 0.7 cm x 0.6 cm x 0.6 cm in size, and contained a tan-brown purulent fluid. Histological examination showed a cystic lesion predominantly lined by pseudostratified ciliated columnar epithelium with patchy mixed inflammation noted (Figures 1, 2). There were foci of low cuboidal epithelium and squamous metaplasia, consistent with bronchogenic cysts (Figures 3, 4) [2]. A pathologic diagnosis of a bronchogenic cyst was made.
Low-power (20x) histopathology of the bronchogenic cyst showing a cystic structure with patchy mixed inflammation. (Hematoxylin and Eosin stain)
High-power (40x) histopathology of the bronchogenic cyst wall.The arrows indicate a pseudostratified ciliated columnar epithelium (hematoxylin and eosin stain).
High-power (40x) histopathology of the bronchogenic cyst wall.The arrow indicates foci of the low cuboidal epithelium (hematoxylin and eosin stain).
High-power (40x) histopathology of the bronchogenic cyst wall.The arrows indicate foci of squamous metaplasia (hematoxylin and eosin stain).
The patient returned for an examination two weeks postoperatively. The ventral tongue was well healed, and the patient reported no sensorineural or functional deficits. Since the recurrence rate for bronchogenic cysts is low and the oral tongue can easily be surveilled, a one-year follow-up appointment was scheduled for the patient.
Discussion
The exact etiology of bronchogenic cyst development remains unknown. During the third week of embryogenesis, the foregut differentiates into the respiratory tract ventrally and the gastrointestinal tract dorsally [1-4]. The tongue develops during the fourth week, forming from the pharyngeal endoderm, branchial mesoderm, and occipital somites. As a result, the primitive foregut and developing branch arches are in close proximity. Bronchogenic cysts can develop from undifferentiated remnants from the primitive tongue that are entrapped during tongue development [4-10]. The presentation of bronchogenic cysts in early life suggests a developmental aberrancy as the underlying cause. One hypothesis proposes that the cysts form from small buds of diverticula that separate from the foregut during tracheobronchial tree development [3].
The most common sites for bronchogenic cyst development are in the mediastinum and lung (75% and 25%, respectively). The incidence of this cyst in the head and neck region, however, is less than 1% of cases [5-9]. Even rarer is a lingual bronchogenic cyst, with less than 30 cases being reported. Most of the cases demonstrate a male predilection with an onset age of six years or younger. While these are present at birth, they can present as late as 61 years of age (Table 1). The most common location is the ventral tongue (Figure 5). Lingual bronchogenic cysts are typically noticed at birth clinically presenting as asymptomatic lingual masses or with feeding difficulties during infancy. If sufficiently large, they may be detected during prenatal ultrasonography screening [3]. In our case, the bronchogenic cyst presented initially as an enlarging mass that eventually became indurated and painful.
Locations of bronchogenic cysts reported intraorally in the literature.Generated from intraoral sites from Table 1 with Microsoft Excel.
Multiple authors have reported the use of magnetic resonance imaging (MRI) and computed tomography (CT) to characterize bronchogenic cysts and define the boundaries for surgical excision [1,3]. While these imaging modalities aid in characterizing the mass, they do not provide a definitive diagnosis. The differential diagnosis for a bronchogenic cyst includes other developmental anomalies, such as branchial cysts, thyroglossal duct cysts, and other foregut duplication cysts [2]. Additionally, more common head and neck pathologies, such as lipomas, mucoceles, ranulas, vascular malformations, dermoid cysts, and teratomas, must also be considered [3-8].
On histopathological analysis, all reported cases of bronchogenic cysts have been shown to contain pseudostratified columnar epithelium [4-12]. Focal areas of non-ciliated cuboidal, columnar or stratified squamous epithelium [13-18]. The presence of cartilage and smooth muscle is often seen [3]. Additionally, mild chronic inflammation has been reported in the majority of cases, as presented in this case [3-8].
With regard to treatment, the majority of the cases reported were managed with surgical excision alone (Table 1). Surgical excision is considered the definitive treatment [12-17]. Furthermore, there have been no documented cases of the role of adjuvant therapy following surgical excision [16-20]. In general, there is no recurrence following complete excision of the cysts in both short- and long-term follow-up periods [10-20]. However, there have been cases of adenocarcinoma, arising from intra-thoracic bronchogenic cysts [6]. Volchok et al. described a case of adenocarcinoma arising from a previously undiagnosed lingual foregut duplication cyst in a 61-year-old man [6]. In this case, the adenocarcinoma was treated and monitored according to the standardized cancer guidelines.
Conclusions
Lingual bronchogenic cysts are extremely rare foregut choristomas that are typically diagnosed within the first decade of life. In the head and neck region, the majority generally present asymptomatically on the ventral tongue. These cysts are managed with surgical excision with a low recurrence rate. The defining histopathologic characteristic distinguishing this cyst from other common cysts in the head in neck is a pseudostratified ciliated columnar epithelium, which is consistent with respiratory tissue. As with many conditions in the oral cavity, early recognition of the disease process is important in treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lingual bronchogenic cyst in a young child: a case report Acta Otolaryngol Case Rep Gunnarsdottir AB Nilsson JS 394232018
- 2A detached bronchogenic cyst occurring in the tongue of a neonate Br J Oral Surg Bailey BM 288293201982696193710.1016/s 0007-117x(82)80025-5 · doi ↗ · pubmed ↗
- 3A bronchogenic cyst masquerading as a tongue mass Head Neck Pathol Aldawood Z Moyer DJ Woo SB 140414081520213363876010.1007/s 12105-021-01303-x PMC 8633169 · doi ↗ · pubmed ↗
- 4Lingual cyst lined by respiratory and gastric epithelium in a neonate Br J Oral Maxillofac Surg Joshi R Cobb AR Wilson P Bailey BM 1731755120132255469410.1016/j.bjoms.2012.04.003 · doi ↗ · pubmed ↗
- 5Sublingual foregut cyst J Dermatol Kim YS Ahn SK Lee SH 476478251998971498310.1111/j.1346-8138.1998.tb 02438.x · doi ↗ · pubmed ↗
- 6Adenocarcinoma arising in a lingual foregut duplication cyst Arch Otolaryngol Head Neck Surg Volchok J Jaffer A Cooper T Al-Sabbagh A Cavalli G 71771913320071763878710.1001/archotol.133.7.717 · doi ↗ · pubmed ↗
- 7Retention cyst of the tongue (glossocele)Oral Surg Oral Med Oral Pathol Fink HA 129012931619631408230010.1016/0030-4220(63)90401-8 · doi ↗ · pubmed ↗
- 8Intralingual cysts of foregut origin S Afr J Surg Constantinides CG Davies MR Cywes S 227232201982 https://pubmed.ncbi.nlm.nih.gov/7179033/7179033 · pubmed ↗