Clinical Challenges in Managing Bilateral Acute Iris Transillumination: Insights From a Case Triggered by Fluoroquinolone Therapy
Sina Hakami, Youssef Afifi, Majda Rachdi, Xavier Dominguez y Costa, Aurélie Le

TL;DR
This paper reports a rare case of bilateral acute iris transillumination triggered by moxifloxacin, highlighting its severe and persistent complications.
Contribution
The study provides clinical insights into managing BAIT, emphasizing differentiation from BADI and the role of fluoroquinolones.
Findings
BAIT can be triggered by moxifloxacin and presents with severe photophobia and intraocular hypertension.
Long-term management with carbonic anhydrase inhibitors and alpha-adrenergic blockers helps stabilize IOP.
Persistent iris atrophy and pigment dispersion may occur despite treatment.
Abstract
Bilateral acute iris transillumination (BAIT) is a rare ocular condition characterized by acute pigment dispersion from the iris pigment epithelium (IPE), resulting in diffuse iris transillumination, atonic mydriatic pupils, and intraocular hypertension. BAIT is often associated with severe photophobia and requires extended medical management. Differentiating BAIT from related conditions such as bilateral acute depigmentation of the iris (BADI) is critical, as BAIT presents with a more severe clinical course and lasting complications. Trigger factors include respiratory infections and fluoroquinolone use, particularly moxifloxacin. This report details a case of BAIT following oral moxifloxacin use. A 69-year-old male patient presented with bilateral ocular redness, pain, and severe photophobia one day after receiving an influenza vaccination and one-week post-moxifloxacin treatment.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
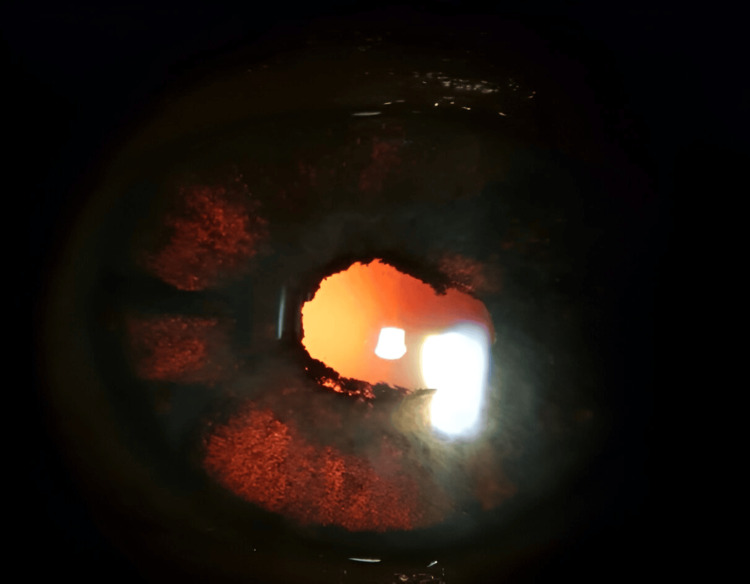 Figure 1
Figure 1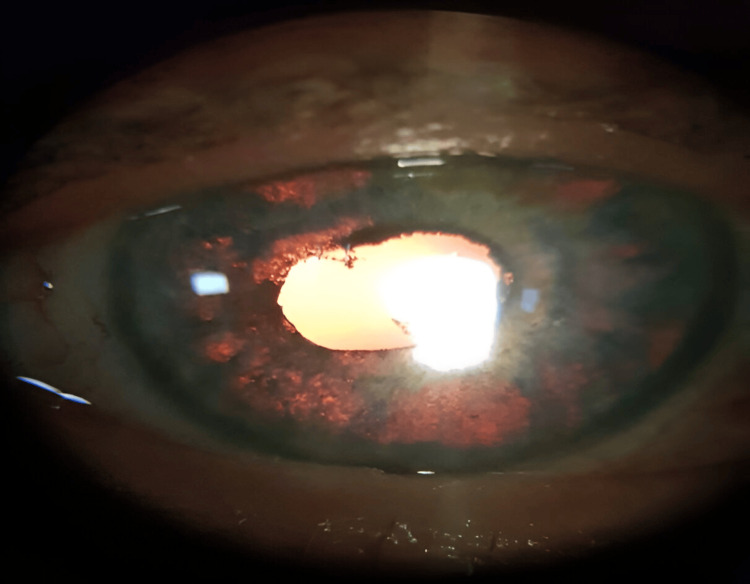 Figure 2
Figure 2 Figure 3
Figure 3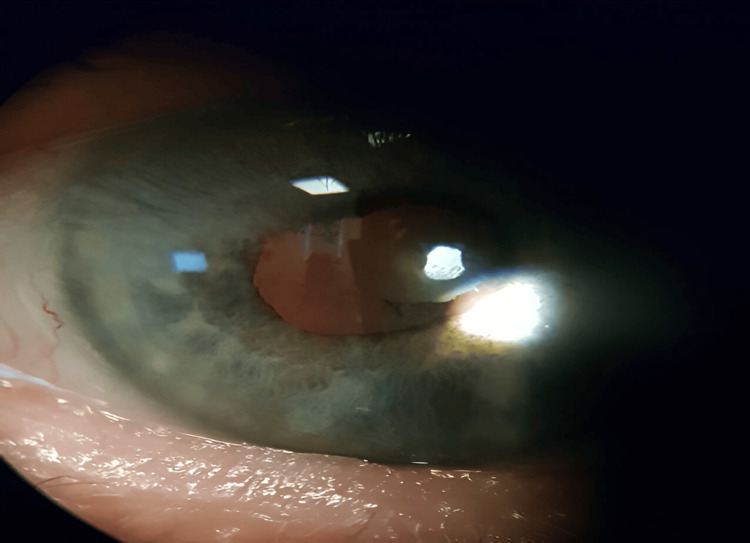 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Infections and Treatments · Ocular Diseases and Behçet’s Syndrome · Glaucoma and retinal disorders
Introduction
Bilateral acute iris transillumination (BAIT) is a clinical entity characterized by acute pigment dispersion originating from the iris pigment epithelium (IPE), leading to diffuse iris transillumination. First formally described by Tugal-Tutkun et al. in 2011 [1], BAIT typically presents with acute-onset severe photophobia, conjunctival hyperemia, and pigment dispersion in the anterior chamber. Clinical features include atonic mydriatic pupils unresponsive to light and persistent intraocular hypertension caused by dense pigment deposition in the trabecular meshwork [2]. These complications often require long-term medical management or surgical intervention.
A closely related condition, bilateral acute depigmentation of the iris (BADI), is also characterized by acute pigment dispersion but involves the iris stroma rather than the IPE. Unlike BAIT, BADI does not lead to transillumination defects or pupillary abnormalities and generally follows a milder, self-limiting course with transient intraocular pressure (IOP) elevation [2]. While BAIT is associated with a more severe clinical course and lasting sequelae, the distinction between the two conditions can be challenging due to overlapping features [2].
Both BAIT and BADI have been associated with various potential triggers, including respiratory tract infections [1,3,4], genetic factors [5], and the use of fluoroquinolone antibiotics, particularly moxifloxacin [3,4,6]. The exact etiopathogenesis still remains unclear, and multiple case reports suggest that these conditions affect individuals of various ethnic backgrounds with a predominant involvement of women [2]. We present a case of BAIT in a patient who developed the condition following oral moxifloxacin use.
This report was previously presented as a poster at the 2024 Controversies in Ophthalmology (COPHy) Congress on March 15 and 16, 2024.
Case presentation
Our case concerns a 69-year-old male patient who was referred to the ophthalmology department for bilateral ocular redness, pain, and photophobia. Symptoms appeared a day after receiving influenzae vaccination and one week after undergoing treatment with oral moxifloxacin, prescribed by his family doctor for a lung infection. Prior to presenting to the emergency ophthalmology department, the patient had no history of ophthalmologic disease or similar attacks.
On slit lamp examination, the patient exhibited bilateral palpebral edema, important chemosis, and diffuse bullous keratopathy, with an IOP estimated to be higher than 35 mmHg on bi-manual palpation since applanation tonometry was unfeasible. Fundus examination was also unachievable. Initial diagnosis leaned towards herpes virus activation: oral acyclovir, oral acetazolamide, and tetracyclin ointment were started. A subsequent check after 24 hours showed no improvement, leading to a prescription of methylprednisolone 64 mg, tobramycine-dexamethasone drops, cyclopentolate drops, and continued oral acyclovir as a precautionary measure.
Photophobia, palpebral edema, and chemosis were greatly resolved under treatment two days later. However, three large keratic bubbles remained on the right eye.
One week later, the examination showed a clear cornea without epithelial blisters, atonic mydriatic pupils with posterior synechiae on both eyes, pigment cells in the anterior chamber, and bilateral diffuse iris depigmentation with transillumination (Figures 1, 2). Visual acuity was measured, using the Snellen chart, at 0.4 in the right eye and 0.8 in the left eye, and applanation tonometry measure showed an IOP of 15 mmHg on both eyes. The fundus examination and posterior segment optical coherence tomography (OCT) were normal.
Slit lamp photograph of the right eye showing diffuse iris transillumination defects with large patches of atrophy and posterior synechia
Slit lamp photograph of the left eye showing diffuse iris transillumination defects with large patches of atrophy and posterior synechia
The tapering of methylprednisolone was initiated, with the continuation of tobramycine-dexamethasone only. During follow-up, the patient developed an increase of IOP, predominantly in the right eye measured at 27 mmHg, attributed to significant pigmentation in the anterior chamber. A treatment with carbonic anhydrase inhibitors and local alpha-adrenergic inhibitors was then initiated.
Nearly one year after treatment, the patient showed improved visual acuity, reduced symptoms, and IOP within a normal range. The anterior chamber remained deep, and the angle remained open and free of synechiae, although persistent pigment was noted in the anterior chamber. The lens showed pigment deposits on the anterior capsule, but no anterior subcapsular cataract was present. Nonetheless, persistent iris depigmentation (Figures 3, 4), with large areas of transilluminable diffuse atrophy, was observed.
Photograph of the eyes during the one-year follow-up showing persistent synechia and depigmentation zones
Slit lamp photograph of the left eye showing stromal depigmentation zones from the peripheral iris to the peripupilary area with spared sectors that retain normal iris color
Discussion
The presented case illustrates an interesting form of BAIT, where our patient demonstrated key clinical features of BAIT, including diffuse iris transillumination, atonic mydriatic pupils, and persistent pigment dispersion in the anterior chamber, with the additional finding of bilateral bullous keratopathy, demonstrating that severe cases of BAIT can present with significant ocular structural alterations.
Also, the clinical evolution in this case shows the importance of careful monitoring during corticosteroid tapering. The resolution of acute symptoms under systemic corticosteroids was followed by a recurrence of IOP elevation upon dose reduction, reflecting the risk of recurrent symptomatic pigment discharge especially when associated with rapid tapering or early discontinuation of corticosteroids [1]. Such episodes highlight the necessity for regular IOP monitoring and extended follow-up until the resolution of pigment dispersion to prevent long terms sequelae such as glaucomatous damage or irreversible photophobia [2,7]. Pigment circulation in BAIT can persist for months, with a median of five months ranging from one to 18 months [1], compared to BADI, where it generally lasts between one and 16 weeks, with a median of eight weeks [2]. Luckily, in this case, carbonic anhydrase inhibitors and alpha-adrenergic inhibitors were effective in controlling IOP. Nonetheless, some described cases required filtration surgery due to insufficient response to pharmacologic treatment alone [8].
Differential diagnosis was important given the similarities between BAIT with BADI. Both conditions share bilateral pigment dispersion as a hallmark but differ in the origin of pigment loss. In BADI, pigment dispersion occurs from the iris stroma without transillumination defects or atonic pupils, and the condition generally follows a more benign and self-limiting course. By contrast, BAIT involves severe pigment release from the IPE, resulting in diffuse iris transillumination and a higher risk of persistent complications, including significant IOP elevation.
Mixed presentations, where one eye displays features of BADI and the other of BAIT, or cases with overlapping characteristics, have been reported [6,9], further complicating the differentiation between these entities. These findings suggest that BAIT and BADI may represent phenotypic variations of a single pathological entity [2].
The etiopathogenesis of BAIT and BADI remains uncertain, but the association between oral moxifloxacin use and symptom onset in this case supports its role as a potential trigger. Interestingly, the occurrence of unilateral BAIT-like syndromes following intracameral moxifloxacin use provides further evidence supporting its role as a direct toxic trigger [10-13]. Given the growing evidence of this association, clinicians should exercise caution when prescribing fluoroquinolones, especially to patients with a history of BADI or BAIT, as re-exposure could exacerbate pigment dispersion and lead to significant ocular morbidity.
Moreover, another differential diagnosis considered initially was herpetic iridocyclitis, which can mimic BADI and BAIT [2,14]. Herpetic involvement is often unilateral and associated with atrophy of the iris with transillumination defects and elevated IOP [15] as seen in BAIT. Fuchs' iridocyclitis, often associated with heterochromia, represents another differential diagnosis [16]. Similarly, pigment dispersion syndrome (PDS) should also be considered, and is distinguished by the characteristic pigment deposition along Scheie’s stripe on the posterior lens capsule [2]. Finally, in cases of BAIT, it is essential to differentiate it from chronic angle-closure glaucoma (CACG). In CACG, the pupil may be unreactive, remaining mid-dilated and fixed due to ischemia of the iris sphincter, whereas in BAIT, it may be unreactive due to posterior synechiae. BAIT presents with bilateral iris transillumination defects and open angles, whereas CACG is typically characterized by a shallow anterior chamber (usually unilateral) and angle closure.
Conclusions
This case highlights the clinical variability of BAIT and reinforces the importance of individualized management, particularly during corticosteroid tapering. Accurate differentiation from BADI and other pigment dispersion syndromes is critical to ensure appropriate treatment and follow-up. Additionally, the potential role of moxifloxacin as a trigger underscores the need for vigilance when prescribing fluoroquinolone antibiotics, particularly in at-risk populations. Long-term follow-up remains essential to address potential recurrences and manage chronic sequelae.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bilateral acute iris transillumination Arch Ophthalmol Tugal-Tutkun I Onal S Garip A Taskapili M Kazokoglu H Kadayifcilar S Kestelyn P 1312131912920112198767410.1001/archophthalmol.2011.310 · doi ↗ · pubmed ↗
- 2Bilateral acute depigmentation of iris (BADI) and bilateral acute iris transillumination (BAIT)-an update Turk J Ophthalmol Tuğal-Tutkunİ AltanÇ 3423475220223631781210.4274/tjo.galenos.2022.09552 PMC 9631498 · doi ↗ · pubmed ↗
- 3Bilateral acute iris transillumination following systemic administration of antibiotics Eye (Lond) Tranos P Lokovitis E Masselos S Kozeis N Triantafylla M Markomichelakis N 119011963220182949713310.1038/s 41433-018-0054-y PMC 6043476 · doi ↗ · pubmed ↗
- 4Is oral moxifloxacin associated with bilateral acute iris transillumination?Acta Ophthalmol Kreps EO Hondeghem K Augustinus A Sys C Van de Veire S Leroy BP Schauwvlieghe PP 0896201810.1111/aos.1355829068528 · doi ↗ · pubmed ↗
- 5Bilateral acute depigmentation of the iris in two siblings simultaneously Am J Ophthalmol Case Rep Amin R Nabih A Khater N 2572601020182978094610.1016/j.ajoc.2018.03.016PMC 5956750 · doi ↗ · pubmed ↗
- 6Acute depigmentation of the iris: a retrospective analysis of 22 cases Can J Ophthalmol Kawali A Mahendradas P Shetty R 33395420193085177210.1016/j.jcjo.2018.03.020 · doi ↗ · pubmed ↗
- 7Bilateral acute iris transillumination (BAIT) syndrome: literature review Clin Ophthalmol Perone JM Chaussard D Hayek G 9359431320193123963510.2147/OPTH.S 167449 PMC 6556534 · doi ↗ · pubmed ↗
- 8Long-term results of trabeculectomy with mitomycin-C in patients with bilateral acute iris transillumination J Glaucoma Bayraktar S Oray M Altan C Basarir B Izgi B Tugal-Tutkun I 7978022820193123345610.1097/IJG.0000000000001309 · doi ↗ · pubmed ↗