A Wide QRS Complex Tachycardia with Variation of Ventriculoatrial Interval: What is the Mechanism?
Engin Algul, Idriz Merovci, Meryem Kara, Elif Hande Ozcan Cetin, Duygu Kocyigit Burunkaya, Hamza Sunman, Ahmet Korkmaz, Firat Ozcan, Serkan Cay, Ozcan Ozeke, Ozcan Ozdemir, Dursun Aras, Serkan Topaloglu

TL;DR
This paper discusses the mechanism behind a type of heart rhythm disorder with a wide QRS complex and changing ventriculoatrial interval.
Contribution
The paper highlights how variation in a specific intracardiac interval can aid in diagnosing complex arrhythmias.
Findings
Variation in intracardiac intervals can change tachycardia cycle length.
Such changes can help distinguish between different types of arrhythmias.
Intracardiac interval analysis is a diagnostic tool for wide complex tachycardia.
Abstract
The differential diagnosis for wide complex tachycardia includes all causes of narrow complex tachycardia with bundle branch block, all causes of narrow complex tachycardia with antegrade pre-excitation, ventricular tachycardia, and antidromic and other pre-excited reciprocating tachycardias. The variation in a specific intracardiac interval that causes a subsequent change in the tachycardia cycle length or another intracardiac interval can be diagnostic in these arrhythmias.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
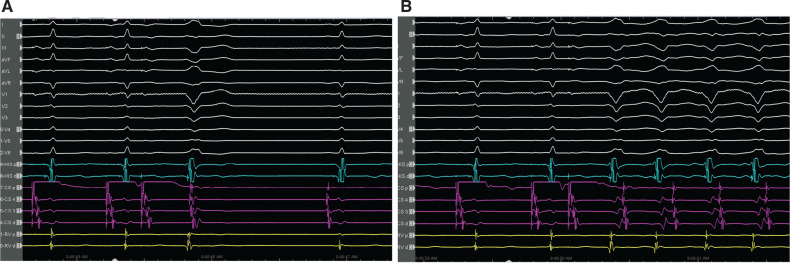 Figure 1
Figure 1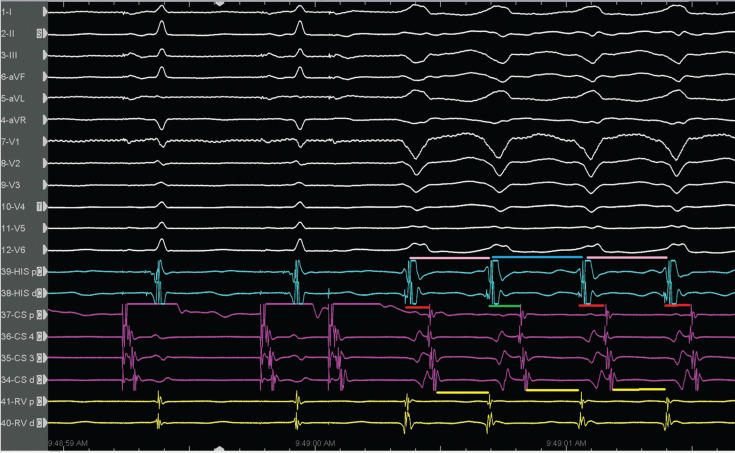 Figure 2
Figure 2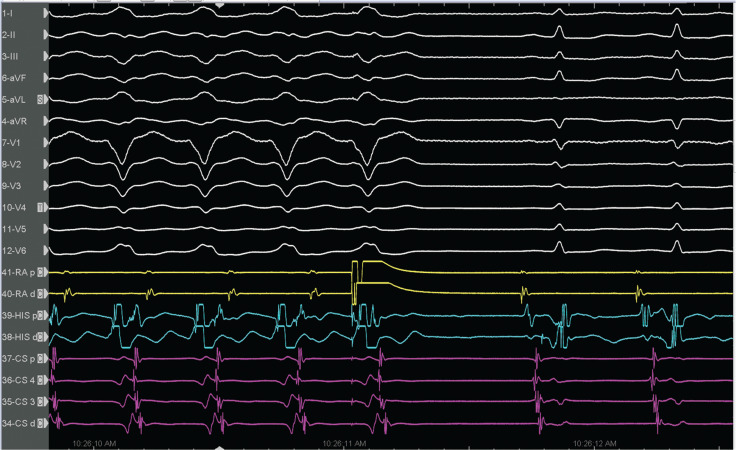 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Atrial Fibrillation Management and Outcomes · Cardiac electrophysiology and arrhythmias
Case presentation
A 28-year-old woman underwent an electrophysiology study (EPS) because of episodes of palpitations with documented narrow complex tachycardia (NCT) and wide QRS complex tachycardia (WCT) on a 24-h Holter electrocardiogram (ECG). Baseline ECG showed normal sinus rhythm without ventricular pre-excitation. During the EPS, the para-Hisian pacing demonstrated the nodal response. The programmed electrical stimulation from the right atrium (Figure 1) showed a left bundle branch block (LBBB)-shaped WCT. There was an interesting observation in the circuit during ongoing tachycardia (Figure 1B). What diagnostic information can be retrieved from the tracing?
Response to programmed atrial stimulation (A) and the initiation of the left bundle branch block tachycardia (B).
Discussion
Programmed atrial stimulation revealed an antegrade jump with a typical atrioventricular (AV) nodal echo beat with an LBBB-shaped QRS pattern (Figure 1A) and then induction of the LBBB-shaped WCT (Figure 1B). The differential diagnosis for WCT includes all causes of NCT with bundle branch block, all causes of NCT with antegrade pre-excitation, ventricular tachycardia (VT), and antidromic and other pre-excited reciprocating tachycardias.^1–8^ Careful examination of the His bundle activation sequence can lead to the correct diagnosis at first glance in an otherwise highly complex diagnostic challenge.^7^ The lack of a regular H–V interval preceding each QRS complex suggests that activation does not use the orthodromic infranodal conduction system, making aberrant conduction less likely.^9^
The LBBB tachycardia showed a 1:1 A–V relation and negative H–V interval, resulting in only two possibilities for the mechanism: pre-excited tachycardia (with active or passive bystander activation) or VT. The activation of the His bundle is retrograde during tachycardia, but still before ventricular activation. This is only possible in the presence of an extranodal pathway inserted in the fascicle just below the His bundle, most frequently the right bundle. An A–V interval of ≥150 ms during pre-excited tachycardia is also a fast and reliable method for detecting a decremental conducting accessory pathway.^10^ If retrograde activation of the His bundle has been determined and changes in the V–H or H–A intervals predict changes in the atrial cycle length and reset the tachycardia (Figure 2), then antidromic tachycardia, either with an atrioventricular bypass tract or an atriofascicular tract, is present. Changes in the V–H or H–A intervals that cause changes in the A–A interval but do not reset the tachycardia suggest VT as the mechanism of the wide complex rhythm. Therefore, the most striking finding in the present case was that there were oscillations in the cycle length and V–A intervals (Figure 2), which predicted subsequent changes in A–A intervals, implicating the retrograde conduction system in the tachycardia circuit.^4^
Oscillation in the cycle length and ventriculoatrial intervals. The V–A interval changes preceded and predicted the V–V intervals.
The rate changes in antidromic tachycardia in patients with atriofascicular fibers can be based on a shift in ventriculoatrial conduction from one bundle branch to the other by retrograde right bundle branch block.^10^ The ventriculoatrial wobble in Figure 2 was unlikely to be due to variation in retrograde right bundle versus left bundle conduction, as the V–H interval was unchanged. There was a long–short sequence due to a fast pathway block on the first pre-excited beat, with a shortening of the anterograde conduction on the second beat. This likely causes retrograde decrement in the fast pathway (identical atrial activation sequence). Furthermore, the late-coupled premature atrial contraction resulted in tachycardia termination (Figure 3), which suggests the participation of an anterogradely conducting accessory pathway, thus confirming the diagnosis of antidromic reciprocating tachycardia and ruling out pre-excited supraventricular tachycardia, nodofascicular tract, and VT.^7,11,12^ Then, a classical slow–fast atrioventricular nodal re-entrant tachycardia (AVNRT) was induced by programmed atrial stimulation (Figure 4). We made the final diagnosis of dual tachycardia by typical AVNRT with atriofascicular tachycardia.^13^ After ablations at the base of Koch’s triangle for the AV nodal slow pathway and the atriofascicular accessory pathway potential at the lateral tricuspid annulus sequentially, the tachycardias were rendered non-inducible.
Termination response to a premature atrial beat delivered during atrioventricular nodal refractoriness.
Initiation of the narrow complex tachycardia by a programmed atrial stimulation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tuncez A Merovci I Efe TH Transition from two wide to a narrow QRS complex tachycardia: what is the mechanism of tachycardia and transition?J Cardiovasc Electrophysiol 20223361316131910.1111/jce.1547935362173 · doi ↗ · pubmed ↗
- 2Ozeke O Cay S Ozcan F Topaloglu S Aras D Electrophysiological maneuvers for concealed nodofascicular or upper common pathways: positive findings always work, but negative findings does not Pacing Clin Electrophysiol 201942339239310.1111/pace.1360430653677 · doi ↗ · pubmed ↗
- 3Ozcan Cetin EH Kara M Merovci I A wide QRS tachycardia with the short and long ventriculoatrial interval in the presence of an atriofascicular pathway: what is the mechanism?J Cardiovasc Electrophysiol 202233112398240210.1111/jce.1568836150138 · doi ↗ · pubmed ↗
- 4Kara M Korkmaz A Ozeke O Wide QRS tachycardia with alternating QRS morphologies: what is the mechanism?Pacing Clin Electrophysiol 202043114614810.1111/pace.1384731774186 · doi ↗ · pubmed ↗
- 5Kara M Korkmaz A Karimli E A narrow QRS complex during a left bundle branch block morphology wide QRS tachycardia: a clue for manifest or bystander involvement of nodofascicular pathway?J Cardiovasc Electrophysiol 202031255255610.1111/jce.1434331916620 · doi ↗ · pubmed ↗
- 6Kara M Cetin EHO Korkmaz A Transient changes in QRS morphology during a narrow complex tachycardia: what is the mechanism?J Cardiovasc Electrophysiol 20223361320132110.1111/jce.1552335524413 · doi ↗ · pubmed ↗
- 7Korkmaz A Ozeke O Cay S Response to His-refractory premature atrial complex with antegrade and retrograde septal depolarization: what is the mechanism?J Arrhythm 201935577677810.1002/joa 3.1222231624522 PMC 6786982 · doi ↗ · pubmed ↗
- 8Aslan AO Merovci I Tuncez A Widening of the QRS complex during the wide complex tachycardia: what is the mechanism?J Cardiovasc Electrophysiol 20223371605160810.1111/jce.1556735671328 · doi ↗ · pubmed ↗