Relationship of sleep and activity, assessed via a wristwatch-type pulsimeter with an accelerometer, with health status in community-dwelling older adults: A preliminary study
Akiyo Sasaki-Otomaru, Kyoko Saito, Kotaro Yamasue, Osamu Tochikubo, Yuka Kanoya, Hidetaka Hamasaki, Hidetaka Hamasaki, Hidetaka Hamasaki

TL;DR
This study explores how sleep and activity data from a wearable device relate to health status in older adults, finding that body movement is linked to health indicators in men.
Contribution
The study introduces a novel use of a wristwatch-type wearable device to assess health status and frailty risk in older adults.
Findings
Body-movement duration in men was strongly and negatively correlated with the Kihon Checklist (KCL) score.
Body-movement duration showed moderate correlations with various health metrics in men, including depression and physical functioning scores.
Body-movement duration was negatively associated with age and the KCL score in multiple linear regression analysis.
Abstract
Wearable devices have the potential to promote a healthy lifestyle; however, studies on the use of wearable devices in monitoring health in older adults are limited. We aimed to investigate the relationship of sleep and activity data with health status among older adults. Fifty-five community-dwelling older adults were asked to wear a wristwatch-type wearable device (the Pulsense [PS]) and measure home blood pressure (HBP) over a period of 5–7 consecutive days. Deep-sleep duration, physical and mental activity duration, and body-movement duration were obtained from PS data using special software. We also collected data on demographics and physical and mental health status. We found that the body-movement duration in women was longer than that in men. Among men, body-movement duration was strongly and negatively correlated with the Kihon Checklist (KCL) score. It also showed moderate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
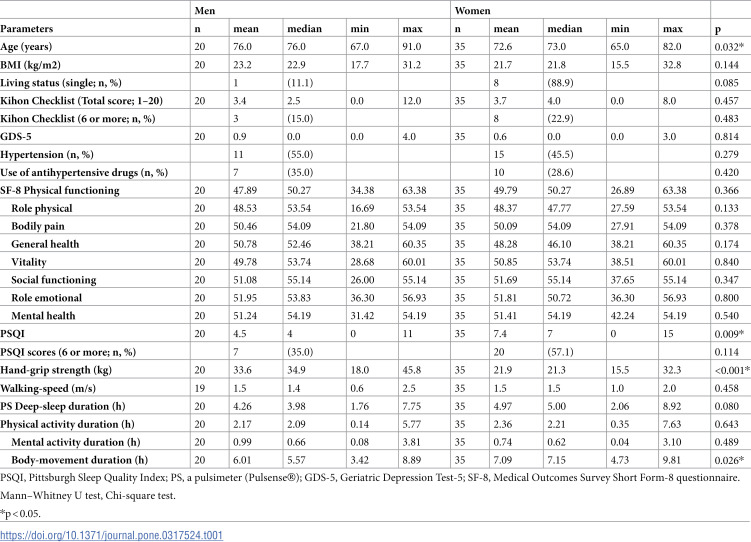 Figure 1
Figure 1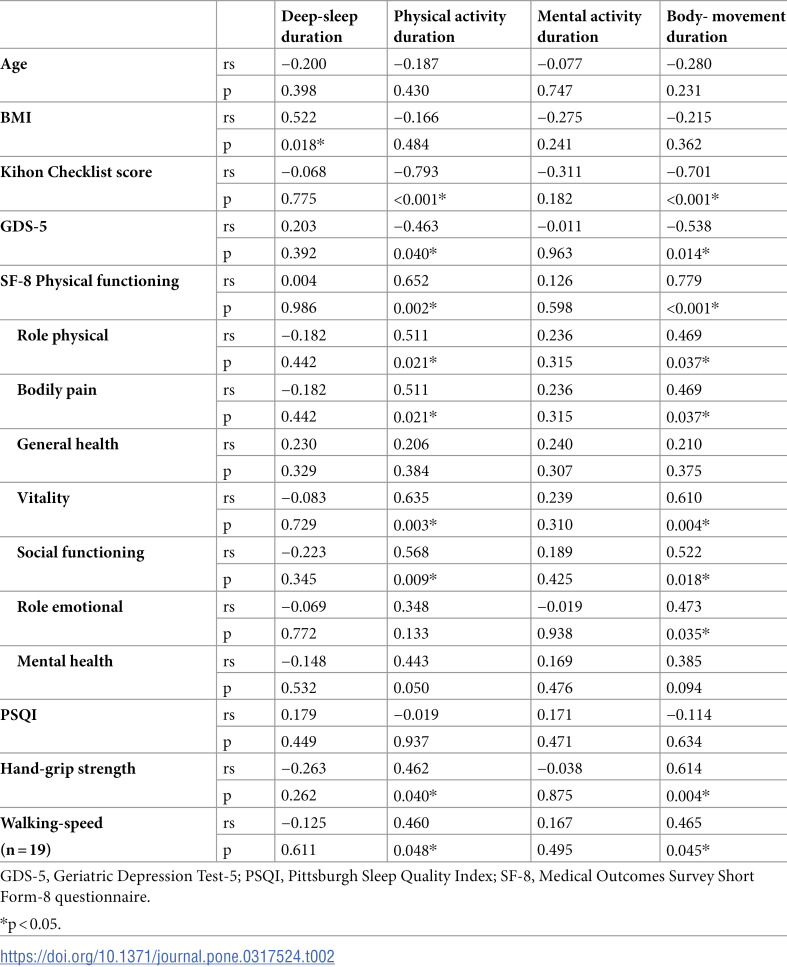 Figure 2
Figure 2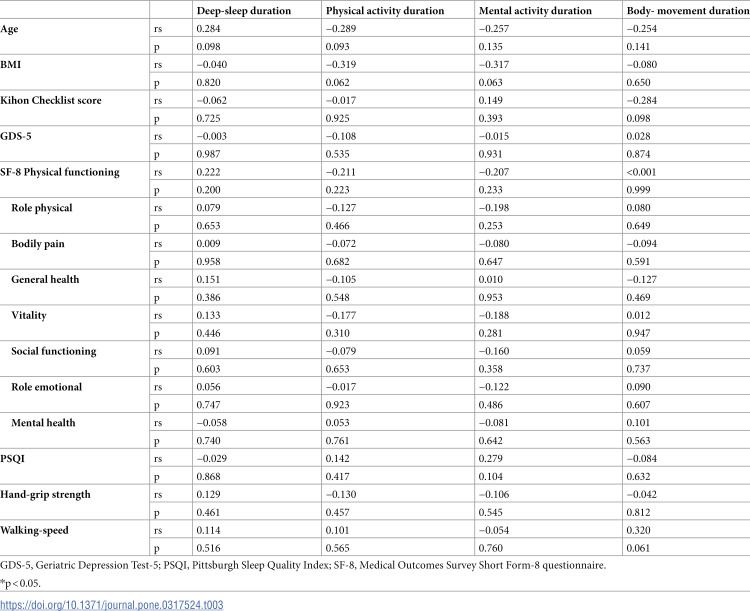 Figure 3
Figure 3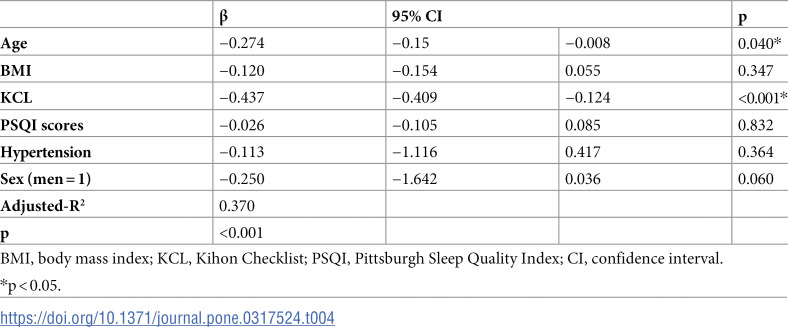 Figure 4
Figure 4- —http://dx.doi.org/10.13039/501100001691Japan Society for the Promotion of Science
- —the 31th Foundation for Total Health Promotion
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and related disorders · Physical Activity and Health · Obesity, Physical Activity, Diet
Introduction
Wearable devices have become a topic of interest in recent years [1]. These devices can measure vital signs such as heart rate, respiration rate, and body temperature, in addition to physical activity and sleep conditions. Accelerometers, which were once mainly worn on the waist, are increasingly being replaced by wrist-type models [2,3]. An accelerometer could evaluate not only moderate-to-vigorous physical activity but also low physical activity (LPA) and sedentary behavior; LPA accounted for a large proportion of total physical activity time among older adults with declining functionality [4]. The Canadian 24-Hour Movement Guideline provides evidence-based recommendations for a healthy day (24-h), comprising a combination of sleep, sedentary behaviors, and light-intensity and moderate-to-vigorous-intensity physical activity [5]. The wristwatch-type wearable devices are expected to provide 24-h monitoring.
We previously used a wristwatch-type pulsimeter with accelerometer (PS-500B; Pulsense®, Seiko Epson Co. Ltd., Nagano, Japan), which is an improvement and productization of previously reported models [6–8]. Our study showed that home blood pressure (HBP) was affected by sleep, even after adjusting for age and body mass index (BMI) among healthy adults [8]. Therefore, we considered that wearable devices can be used to comprehensively assess the lifestyle of older adults.
Japan has the world’s highest life expectancy and a persistently low birth rate. Japan’s population is aging more rapidly than that of any other country [9]. With the increasing number of older adults, a substantial increase in health care and social security costs is expected. The ratio of individuals in need of nursing care increases because of dementia and physical functional deterioration. In Japan, the main reasons for needing nursing care are dementia, cerebrovascular disease, and frailty [10]; therefore, healthy behaviors, such as increased physical activity and improved quality of sleep, are important factors in preventing these diseases and symptoms.
The use of wristwatch-type devices has the potential to promote healthy lifestyles in terms of physical activity and weight [11,12]. However, studies on the use of wearable devices in monitoring health in older adults are limited [13,14]. Data on sleep and activity duration in healthy older individuals would be valuable for monitoring purposes. This study aimed to examine the relationship of sleep and activity data (obtained using Pulsense) with the health status of community-dwelling older adults.
Materials and methods
Participants
From July 2015 to August 2017 and from June 2020 to October 2020, we recruited community-dwelling older adults participating in health classes at local health centers. The eligibility criteria were as described in the previous study [8]. Of the 61 participants in the present study, six were excluded due to a lack of sleep and activity data. Finally, we included 55 older adults.
Ethical considerations
The research was conducted according to the principles of the World Medical Association Declaration of Helsinki. Informed consent was obtained from all participants, and this cross-sectional study was approved by the Ethical Committee of the Yokohama City University School of Medicine (approval numbers: A150326011 and A200200005).
Variables
Sleep and activity.
Sleep and activity data were measured using the Pulsense (henceforth termed PS) and processed using special software to yield data on deep-sleep, physical-activity, mental- activity, and body-movement durations [8]. The participants wore the PS over a period of 5–7 consecutive days and nights, as described in a previous study [8].
HBP.
HBP was measured twice a day, in the morning and at night, in a sitting position after at least 10 min of rest according to the guidelines, and the data were averaged over a 5- to 7-day period for each participant [15]. Hypertension was defined as the use of antihypertensive drugs, systolic blood pressure (SBP) ≥ 135 mmHg, and/or diastolic blood pressure (DBP) ≥ 85 mmHg.
Kihon checklist and depression.
The Kihon Checklist (KCL) score was used for a comprehensive evaluation of the physical, psychological, functional, and social status of the participants. The KCL consists of five subdomains (physical, nutritional, oral, cognitive function, and depressive mood). Each KCL score indicates the perceived level of difficulty of the activity in the question, and a higher score on the checklist indicates a higher risk of requiring support in each domain. A total score of ≥6 indicated frailty [16]. The current study applied the KCL without the depression score [17]. Instead, the Geriatric Depression Test-5 (GDS-5) was used to evaluate depressive mood, according to a previous study [16]. A higher score on the GDS indicated a higher risk of depression [18].
Subjective sleep.
Subjective sleep was assessed using the Pittsburgh Sleep Quality Index (PSQI), which included 19 self-administered questions that covered seven domains, namely subjective quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, sleep medication use, and daytime dysfunction. Sleep disturbance was defined as having a PSQI score ≥ 6 [19].
Health-related quality of life.
Health-related quality of life was assessed by administering the Medical Outcomes Survey Short Form-8 questionnaire (SF-8) [20]. The SF-8 consisted of eight items, each representing one health profile dimension: general health perception, physical functioning, role functioning–physical, bodily pain, vitality, social functioning, mental health, and role functioning–emotional. The Japanese version of the SF-8 met the standard criteria for content, construct, and criterion validity, as it was based on a nationwide survey [20].
Physical function.
Measures of physical function included gait speed (in m/s) and hand-grip strength (in kg) and were assessed to reflect physical functional status. To evaluate gait speed, the participants were asked to walk 11 m at their usual pace, and the time taken to traverse the middle 5 m of this distance was measured once [21]. The recorded times were converted to speed (in m/s). Hand-grip strength (kg) was measured using a digital hand dynamometer (T.K.K.5401; Takei Scientific Instruments Co., Ltd., Niigata, Japan). The grip strength of each hand was assessed twice, and the maximal value of each hand was averaged for analysis.
Statistical analysis.
All data were analyzed using SPSS Statistics version 28 (IBM Corp., Chicago, IL, USA). The normality of the data distribution was tested using the Shapiro–Wilk test. The KCL score, PSQI score, GDS score, physical activity duration, and mental activity duration data were not normally distributed. Therefore, differences between the sexes were compared using the Mann–Whitney U-test. Spearman’s correlation test was used to assess the relationship between the PS data and health status measurements, including HBP. We interpreted the relative strength of correlation as follows: < 0.1 = “negligible,” 0.1–0.39 = “weak,” 0.4–0.69 = “moderate,” 0.7–0.89 = “strong,” and 0.9–1.0 = “very strong” [22]. Lastly, multiple linear regression analyses were used to explore the association between the PS data (deep-sleep and body-movement durations) and variables identified as significant by the chi-square test and Spearman’s correlation test. All analyses were two-sided at the 5% level of significance.
Results
Participant characteristics
Of the 55 participants, 35 (63.6%) were women and 26 (47.3%) had hypertension. The mean age of the participants was 73.8 years. Table 1 compares the characteristics of the participants according to sex. There were significant differences in age, PSQI score, hand-grip strength, and body-movement duration between men and women.
Table 1: Characteristics of participants.
PS data and health status
Spearman’s rank correlation coefficients for correlations of sleep and activity data with other variables in each sex are shown in Tables 2 and 3. Among male participants, a strong negative correlation was found between physical activity duration and KCL score (rs = −0.793, p < 0.001) and a moderate negative correlation with GDS-5 score (rs = −0.463, p = 0.040). Physical activity duration showed moderate positive correlations with physical functioning (rs = 0.652, p = 0.002), role physical (rs = 0.511, p = 0.021), bodily pain (rs = 0.511, p = 0.021), vitality (rs = 0.635, p = 0.003), and social functioning (rs = 0.568, p = 0.009) in the SF-8. Physical activity duration was also moderately correlated with hand-grip strength (rs = 0.462, p = 0.040) and walking-speed (rs = 0.460, p = 0.048). Body-movement duration showed strong correlations with KCL score and physical functioning in SF-8. Additionally, deep-sleep duration was moderately correlated with BMI in male participants.
Table 2: Spearman’s rank correlation coefficients between sleep and activity data and variables in male participants (n = 20).
Table 3: Spearman’s rank correlation coefficients between sleep and activity data and variables in female participants (n = 35).
In contrast, no significant correlation was found between PS data and health status among female participants.
Association between body-movement duration and health status
Multilinear regression analyses were conducted to explore the associations between demographic factors and body-movement duration. BMI, hypertension, PSQI, and KCL were selected as predictor variables, with age and gender included as covariates. As shown in Table 4, the KCL score was negatively associated with body-movement duration (β=−0.437, p < 0.001) after adjusting for age and gender. No significant model could be established for factors influencing deep-sleep duration after multiple regression analysis for deep-sleep duration and independent variables.
Table 4: Multilinear regression analysis between body-movement duration and independent variables (n = 55).
Discussion
The present study used physical and sleep data from PS to clarify their relationship with health status. Our results showed that shorter body-movement duration was associated with a higher risk of frailty in older adults after adjusting for age and sex. Frailty prevention is an important topic, particularly concerning Japanese older adult women [23]. The KCL is a governmental standardized index assessing frailty in Japanese individuals [24].
The body-movement duration in women was longer than that in men. The body-movement duration assessed by the PS included light physical activity, such as housework and cooking [25]. A nationwide survey in Japan reported that older women spent more time on housework compared to older men [26]. Another previous study showed that women spent more time in LPA compared to men [4]. Additionally, a cross-sectional study showed that light physical activity was positively associated with physical performance [27]. Light physical activity indicates 2.0–2.9 metabolic equivalents (METs) of physical activity, which includes cooking, feeding household animals, or doing laundry [28]. These activities might be easy to adopt into the lifestyle of older adults of both sexes. Although body-movement duration by PS did not imply LPA, PS might be a useful evaluator of light physical activity to set a target for maintaining and/or increasing body-movement duration. This is so that older adults can understand their own activity time and adjust it as needed.
PS also evaluates physical and mental activities. In this study, physical and mental activity data were not normally distributed; therefore, we did not conduct a multiple linear regression analysis. In simple linear regression analysis, physical activity duration correlated negatively with the KCL and GDS scores and positively with several items of the SF-8. Both physical and mental activity durations might be associated with health status; however, further research is needed to determine the specific factors that influence activity duration. Sedentary behavior in older adults has been linked with negative health outcomes [29]; older people are not always able to exercise because of underlying health conditions. However, PS evaluates acceleration and pulse. Future research should explore the duration of mental activity using PS to identify favorable sedentary behavior patterns.
Deep-sleep duration correlated positively with BMI in simple linear regression in men. Although short sleep duration is generally associated with an increased risk of obesity [30,31], a study reported that long sleep duration was associated with sarcopenic obesity in older men [32]. In our study, we did not find a significant model when deep-sleep duration was used as the dependent variable in a multiple regression analysis. This suggested that further investigation was needed.
In addition, a gender-specific approach is necessary to maintain and improve activity duration. Men spend their time on various activities, such as work, housework, and hobbies. Further reducing these activity times can have negative effects on their physical and mental health. Therefore, it is important to avoid further reducing time to maintain activity levels. Women have more reasons for decreased activity levels than men, such as injuries from falls and fractures. It is important to examine these reasons individually and take appropriate measures. For older adults, it is particularly important for family and caregivers to cooperate in monitoring physical activity duration. Family members living far away can check on the older adult’s condition by phone or video call and encourage them to exercise as needed. Caregivers can also observe and record the older adult’s activity time in their daily lives.
Our study had some limitations. First, a major methodological limitation was the inability to determine causality. Second, only a small number of participants were included. To detect a moderate correlation of 0.4 using R software, we estimated a required sample size of 47 and aimed to recruit 50 participants. Although we successfully recruited 55 individuals, our gender-stratified analysis resulted in smaller sample sizes within each subgroup. Moreover, participants were generally health-conscious, which may limit generalizability. Third, although sleep and activity durations may be affected by the season of the year, the data were collected over periods throughout the year due to weather considerations. This resulted in a survey that was not a comprehensive daily 1-week assessment. Finally, we did not collect information on the nutritional status, which could notably influence frailty. Lastly, the PS could measure only activity and sleep. Other wearable devices with oximeters, electrocardiograms, and other functions are also currently available and warrant further research.
Conclusions
This cross-sectional study suggests that decreased body-movement duration may indicate a potential risk for frailty in older adults. Monitoring physical activity duration and body-movement duration by PS could be important data not only for older adults themselves but also for their families, especially those living far away, and informal caregivers who cannot observe them constantly.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Piwek L, Ellis DA, Andrews S, Joinson A. The rise of consumer health wearables: promises and barriers. P Lo S Med. 2016;13(2):e 1001953. doi: 10.1371/journal.pmed.1001953 26836780 PMC 4737495 · doi ↗ · pubmed ↗
- 2Strain T, Wijndaele K, Dempsey PC, Sharp SJ, Pearce M, Jeon J, et al. Wearable device measured physical activity and future health risk. Nat Med. 2020;26(9):1385–91. doi: 10.1038/s 41591-020-1012-3 32807930 PMC 7116559 · doi ↗ · pubmed ↗
- 3Doherty A, Jackson D, Hammeria N, Plötz T, Olivier P, Granat MH, et al. Large scale population assessment of physical activity using wrist worn accelerometers: The UK Biobank Study. P Lo S ONE. 2017;12:e 0169649. doi: 10.1371/journal.pone.016964928146576 PMC 5287488 · doi ↗ · pubmed ↗
- 4Amagasa S, Inoue S, Ukawa S, Sasaki S, Nakamura K, Yoshimura A, et al. Are Japanese women less physically active than men? Findings from the DOSANCO Health Study. J Epidemiol. 2021;31(10):530–6. doi: 10.2188/jea.JE 20200185 32779629 PMC 8421197 · doi ↗ · pubmed ↗
- 5Ross R, Chaput JP, Giangregorio LM, Janssen I, Saunders TJ, Kho ME, et al. Canadian 24-hour movement guidelines for adults aged 18-64 years and adults aged 65 years or older: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2020;45(10 Suppl 2):S 57–102. doi: 10.1139/apnm-2020-0467 33054332 · doi ↗ · pubmed ↗
- 6Ono K, Yamasue K, Tochikubo O, Terauchi Y, Mizushima S. Lifestyle monitoring with the use of an earphone-type thermometer, and ambulatory blood pressure monitoring and a new wrist watch-type pulsimeter with accelerometer. Clin Exp Hypertens. 2014;36(2):97–102. doi: 10.3109/10641963.2014.892120 24625336 · doi ↗ · pubmed ↗
- 7Sawai A, Fujii H, Sato Y, Takuma A, Utsumi M, Sawai S, et al. Development of wristwatch-type stress-caloriemonitor and its wireless communication management system. Gazz Med Ital. 2016;175:442–5.
- 8Sasaki-Otomaru A, Yamasue K, Tochicubo O, Saito K, Inamori M. Association of home blood pressure with sleep and physical and mental activity, assessed via a wristwatch-type pulsimeter with accelerometer in adults. Clin Expl Hypertens. 2020;42:131–8. doi: 10.1080/10641963.2019.159038230887842 · doi ↗ · pubmed ↗