Fading Away: A Case Report on Whipple's Disease
Nuno Carvalho, Sofia Miguelote, José Pimenta, Isabel Trindade, Jorge Cotter

TL;DR
This case report describes a rare disease called Whipple's disease and highlights the importance of early diagnosis and long-term treatment for recovery.
Contribution
The paper presents a new clinical case of Whipple's disease with detailed diagnostic and treatment outcomes.
Findings
The patient showed symptoms like diarrhea, fatigue, and weight loss, which led to the diagnosis of Whipple's disease.
Histologic and PAS staining confirmed the presence of spongy macrophages, characteristic of the disease.
Long-term antibiotic therapy resulted in significant clinical improvement and full recovery.
Abstract
Whipple’s disease (WD) is a rare, multisystemic chronic disease caused by Gram-positive bacteria Tropheryma (T.) whipplei. Transmission usually occurs by the fecal-oral route, as the bacillus has been identified in stagnant water, human feces, and soil. This disorder not only causes malabsorption in the gastrointestinal tract but also has cardiovascular, neurological, ophthalmic, and musculoskeletal effects. Prolonged symptoms are the hallmark of this pathology. Definitive diagnosis requires histologic demonstration of Periodic Acid-Schiff (PAS) staining in macrophages from small bowel mucosa and/or polymerase chain reaction identification of T. whipplei. Treatment requires prolonged antibiotics for up to two years. We present the case of a 69-year-old man, admitted to the emergency department with complaints of worsening nocturnal diarrhea within the last seven months. Fatigue, weight…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
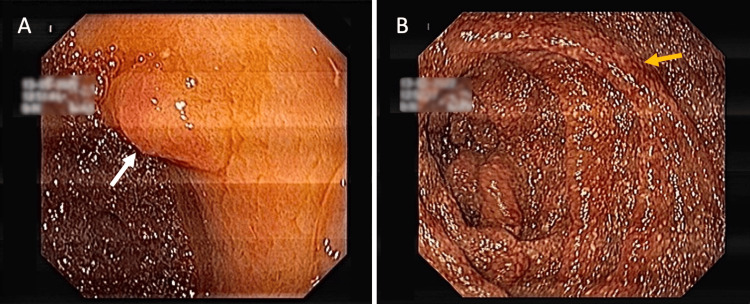 Figure 1
Figure 1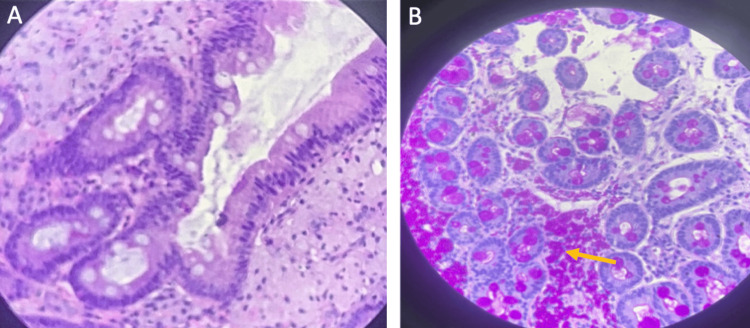 Figure 2
Figure 2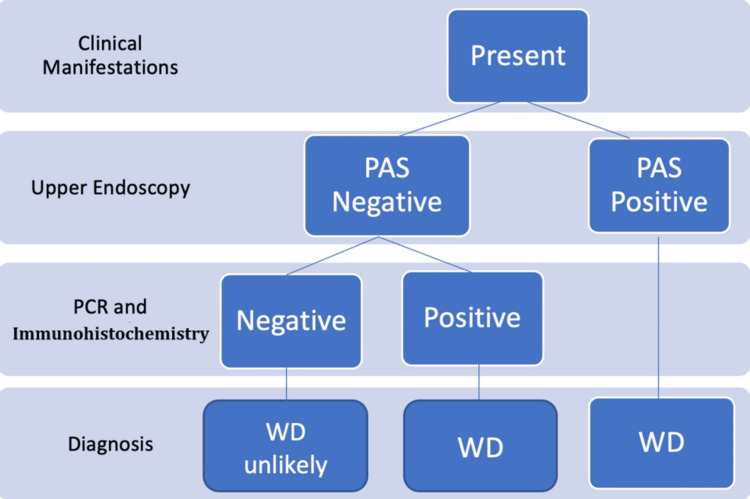 Figure 3
Figure 3| Parameters | Results | Reference range |
| Hg (g/dL) | 6.8 | 13.0-16.0 |
| Hematocrit (%) | 21.5 | 41-53 |
| Mean corpuscular volume (fL) | 71 | 83-103 |
| Mean corpuscular hemoglobin (pg) | 26.6 | 28-34 |
| Leukocytes (x103 /uL) | 3.7 | 4.8-10.8 |
| Neutrophils (x103 /uL) | 2.6 | 1.8-7.7 |
| Eosinophils (x103 /uL) | 0.1 | 0.0-0.49 |
| Basophils (x103 /uL) | 0.0 | 0.0-0.1 |
| Lymphocytes (x103 /uL) | 0.7 | 1.0-4.8 |
| Monocytes (x103 /uL) | 0.3 | 0.1-0.8 |
| Albumin (g/dL) | 2.4 | 3.4-5.0 |
| C-reactive protein (mg/dL) | 10.4 | <5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsWhipple's Disease and Interleukins · Helicobacter pylori-related gastroenterology studies · Mycobacterium research and diagnosis
Introduction
Whipple’s disease (WD) is a rare multisystemic chronic disease caused by Gram-positive bacteria Tropheryma (T.) whipplei, family Actinobacteria. Beyond gastrointestinal malabsorption, this disorder also has cardiovascular, neurological, ophthalmic, and musculoskeletal manifestations [1].
It was initially described by George Whipple in 1907 while reporting the case of a 36-year-old man presenting with diarrhea, weight loss, fever, and migratory polyarthritis. Further documentation of mesenteric lymphadenopathy and skin pigmentation led to its initial designation as “intestinal lipodystrophy” [1,2]. Only 40 years after bacteria identification inside macrophages in submucous tissue was the first patient successfully treated using antibiotics [2].
Case presentation
We present the case of a 69-year-old man who resorted to the emergency department (ED) with complaints of gradually worsening diarrhea for the last 7 months. Four years prior to the current admission, intermittent dorsolumbar inflammatory arthralgia, with scarce response to non-steroidal anti-inflammatory medication, was referred. Then, seven months before ED admission, the patient presented worsening nocturnal watery diarrhea (10 to 15 stools daily) without mucus, blood, or abdominal pain, along with fatigue, significant weight loss (approximately 30 kilograms), night sweats, and worsening lower limb edema. There was no dyspnea, nausea, vomiting, anorexia, or fever.
On physical examination, the patient had an emaciated appearance, discolored mucous membranes, skin hyperpigmentation, and symmetrical edema up to two-thirds of both legs. Non-adherent, elastic, and painless inguinal lymph nodes, two centimeters in diameter, were palpable. Blood tests revealed severe hypochromic/microcytic anemia, along with leucopenia, moderate hypoalbuminemia, and mildly elevated C-reactive proteins. These results are displayed in Table 1. Red blood cell transfusion (two units) was performed with good hematological yield (Hg increase to 9.8 g/dL). The patient was admitted into the Internal Medicine ward for further etiologic study and stabilization.
While hospitalized, a serologic study comprising anti-HIV, HBsAg, anti-HCV, antinuclear antibodies, rheumatoid factor, and thyroid stimulating hormone was negative or within normal limits. Multiple stool microbiologic and parasitological studies were performed; however, all were negative. A thoracoabdominal computed tomography scan (CT) revealed bilateral pleural effusion, with a maximum thickness of four centimeters on the right side and two centimeters on the left. Multiple mesenteric, celiac, periportal, pancreatoduodenal, pericaval, iliac, and inguinal lymphadenopathies were visible, the largest being four centimeters in diameter.
Diagnostic thoracocentesis was performed, revealing transudative effusion without malignant cells, as well as negative bacteriological pleural fluid analysis. Interferon-gamma release assay (IGRA) was also negative. Upper endoscopy was then performed, showing a sessile lesion measuring 12 mm in the antrum (Figure 1A). Progression of the endoscope into the duodenum revealed marked mucosal edema, congestion, and diffuse punctiform lymphangiectasia, and biopsy samples were obtained (Figure 1B). Histologic analysis unveiled spongy macrophages in the lamina propria using hematoxylin-eosin (HE) and PAS staining, suggestive of WD (Figures 2A, 2B).
Upper endoscopic findings(A) Sessile lesion in the antrum (white arrow). (B) Duodenum with marked edema, congestion, and diffuse punctiform lymphangiectasia (yellow arrow).
Histologic findings(A) Duodenum stained with hematoxylin-eosin, displaying macrophages in the lamina propria. (B) Periodic acid-Schiff (PAS)-stained macrophages (yellow arrow).
For a definitive WD diagnosis, two inguinal lymph nodes were excised. Histologic analysis displayed overall preserved architecture, along with reactive alterations within the sinus, and interfollicular histiocytosis with a focus of epithelial cells in small nests. No neoplastic cells were present. Given these results, the diagnosis of WD was confirmed.
Following diagnosis confirmation, antibiotic therapy with intravenous ceftriaxone two grams/daily was initiated. After two weeks of intravenous therapy, the patient was discharged with an indication to complete antibiotic therapy with sulfamethoxazole/trimethoprim 800/160 milligrams every 12 hours for at least 1 year. Follow-up revaluation was scheduled in an outpatient Internal Medicine consultation.
Upon 12 months of antibiotic therapy, clinical improvement was remarkable as the patient fully recovered his previous weight. Fatigue, lower limb edema, and night sweats, as well as diarrhea, were no longer present. Blood tests showed complete resolution of hematological and biochemical abnormalities. Follow-up CT scan demonstrated a significant decrease in previously mentioned lymphadenopathy. Endoscopic follow-up was performed after one year of therapy, with duodenal biopsies revealing an absence of PAS-positive macrophages in histologic analysis.
Discussion
WD is a rare disorder, with a higher prevalence reported in North America and Europe. The incidence rate is 1-3 cases per 1,000,000 people, with the mean age of symptom onset at 55 years. Males are more frequently affected, with a male/female ratio of 4-8/1 [3]. Transmission is usually through the fecal-oral route, as the bacillus has been identified in stagnant water, human feces, and soil [4]. WD susceptibility is thought to be associated with the HLA-B27 haplotype, similar to other infectious diseases, as only some carriers of the WD pathogen develop clinically overt disease. This suggests a probable complex interplay of bacterial, host, and environmental factors in its pathogenesis, with patients at risk of disease likely exhibiting some type of immune deficiency [5].
In WD, there is a massive infiltration of the intestinal mucosa with macrophages due to T. whipplei presence [5]. The bacteria is phagocytized by macrophages, which are unable to eliminate the internalized bacteria due to their ability to reduce the inflammatory response. Perpetuation of this process is accounted for by IL-16 secretion, increasing macrophage recruitment to sites of infection [2,5].
Due to the bacteria’s ability to infect different organs, clinical manifestations may be diverse thus making prompt diagnosis challenging.
Classic WD consists of three progressive stages: the first stage is characterized by musculoskeletal and constitutional symptoms such as arthralgia, arthritis, fever, and asthenia. The latter is followed by gastrointestinal, dermatological, and hematological signs and symptoms such as abdominal pain, diarrhea, weight loss, anemia, and edema. Ascites is an uncommon manifestation of WD, possibly resulting from malabsorption that leads to protein-losing enteropathy and hypoproteinemia, and a serum-ascites albumin gradient (SAAG) lower than 1.1. In the final stage, there is neurologic, ophthalmologic, and cardiac involvement [2,5]. A pathognomonic sign of neurological impairment due to WD is oculomasticatory myorhythmia, which consists of synchronous eye converging movements at the time of masticatory muscle contractions [6]. Since *T. whipplei *has a high affinity for lymph node tissue, lymphadenopathy is a common finding.
In upper endoscopy, macroscopic duodenal abnormalities include villi edema and widening, whitish plaques, and signs of duodenitis, mucosal erythema, or hemorrhage [7]. Definitive diagnosis typically requires histologic demonstration with PAS staining in macrophages from small bowel mucosa and/or polymerase chain reaction (PCR) identification of T. whipplei (Figure 3) [7].
Diagnostic algorithm for Whipple's diseasePAS: Periodic Acid-Schiff stain; WD: Whipple's disease
Although the patient had been symptomatic for many months, this presentation of WD was considered of moderate severity, as no cardiac nor neurologic impairment was evident through clinical or imagiologic investigation. During diagnostic workup, many alternative diagnoses were excluded, specifically more frequent infectious causes (such as HIV, tuberculosis, hepatitis) as well as inflammatory/autoimmune etiologies. Furthermore, the presence of nonspecific imaging findings as well as transudative pleural effusion led to a diagnostic consideration of potentially rare causes. Macroscopic duodenal abnormalities in upper endoscopy raised clinical suspicion for WD diagnosis, and final confirmation was obtained with histologic analysis.
The patient's treatment plan is in accordance with current guidelines, which recommend a short course (two weeks) of either intravenous (IV) beta-lactam (ceftriaxone or penicillin (PCN) G) or meropenem (if PCN/cephalosporin allergy), followed by maintenance treatment with trimethoprim/sulfamethoxazole for one to two years, according to clinical response [1]. Follow-up with clinical, analytic, and endoscopic revaluation is recommended to ensure response to treatment and guide antibiotic duration.
Conclusions
Whipple’s disease is a rare condition and its diagnosis is challenging. Nevertheless, as previously demonstrated, in patients with prolonged clinical presentations of gastrointestinal complaints associated with constitutional symptoms, clinicians should be aware of WD. Although in earlier stages, symptomatic presentation may be nonspecific, in advanced disease, some characteristic signs may prompt diagnosis. In particular, when common infectious/inflammatory etiologies are excluded, diagnostic workup should take into account rarer causes, further promoting WD exclusion. Upper endoscopy and subsequent histologic analysis with PAS staining or PCR detection of *T. whipplei *in duodenal samples are mandatory.
Thus, considering WD in the differential diagnosis of prolonged diarrhea is essential, as delays could lead to disease progression and multisystem involvement with possibly fatal outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Whipple Disease 1 2025 Antunes C Singhal M 2025 Treasure Island (FL)Stat Pearls [Internet]2023 https://www.ncbi.nlm.nih.gov/books/NBK 441937/28722966 · pubmed ↗
- 2Whipple's disease: a case report in Santa Catarina, Brazil Infez Med Stroher CK Santos AL Ceron L Fabrin LL 1391423020223535025010.53854/liim-3001-18PMC 8929735 · doi ↗ · pubmed ↗
- 3Whipple's disease? A case report and discussion Med Pharm Rep Turcan S Tofan-Scutaru L Istrate V Tirbu V 0894202110.15386/mpr-2237 PMC 841182034527918 · doi ↗ · pubmed ↗
- 4Whipple's disease--a challenging diagnosis Acta Med Port Carneiro A Lima P Barbosa I Chaves F 48148652004 https://www.actamedicaportuguesa.com/revista/index.php/amp/article/view/111716197860 · pubmed ↗
- 5Hepatobiliary manifestations of Whipple disease Clin Liver Dis (Hoboken) Kuftinec G Deshpande AR Carrion AF 1801831720213386866210.1002/cld.1004 PMC 8043691 · doi ↗ · pubmed ↗
- 6Hiding in plain sight N Engl J Med Naser JA Fogwe D Ho M Corsini Campioli C Shah A 2075208138720223644942410.1056/NEJ Mcps 2205021 · doi ↗ · pubmed ↗
- 7Role of enteroscopy in the diagnosis of Whipple's disease Acta Gastroenterol Belg Mascarenhas Saraiva M Ribeiro T Costa Pereira T Andrade P Cardoso H Macedo G 6696718420213496505110.51821/84.4.020 · doi ↗ · pubmed ↗