The prognostic value of ultrasound features and parafibromin expression in parathyroid carcinoma
Ruifeng Liu, Liyuan Ma, Yu Xia, Luying Gao, Jiang Ji, Yuang An, Aonan Pan, Nengwen Luo, Yuxin Jiang

TL;DR
This study finds that ultrasound-detected calcification and parafibromin expression are linked to outcomes in parathyroid carcinoma patients.
Contribution
The study identifies ultrasound calcification as an independent risk factor for survival and parafibromin loss as a marker for recurrence/metastasis in parathyroid carcinoma.
Findings
Ultrasound-detected calcification is linked to a 9.4 times higher risk of death in parathyroid carcinoma patients.
Loss of parafibromin expression is associated with a 5.9 times higher risk of recurrence or metastasis.
Parafibromin expression did not significantly affect overall survival.
Abstract
To investigate prognostic factors related with parathyroid carcinoma (PC) based upon ultrasound (US) parameters and parafibromin expression. Between 2000/01 and 2022/07, thirty-four PC patients with detailed preoperative ultrasonography were enrolled in the research. Immunohistochemical staining of parafibromin was performed on pathological samples of these patients. Based on the expression of parafibromin, the cases were divided into a positive control group (parafibromin expression ≥ 10%) and a negative experimental group (parafibromin expression < 10%). The ultrasound and clinical features of the two groups were analyzed, and Cox regression was used to identify the independent prognostic factors regarding disease-free survival (DFS) and overall survival (OS). Among 34 patients with parathyroid carcinoma, 26 (76.5%) were parafibromin-positive, while 8 (23.5%) were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
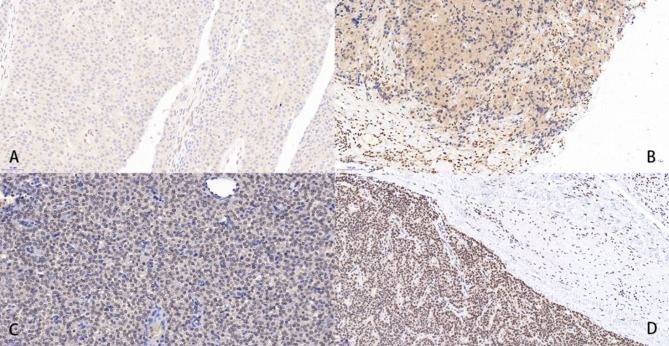 Figure 1
Figure 1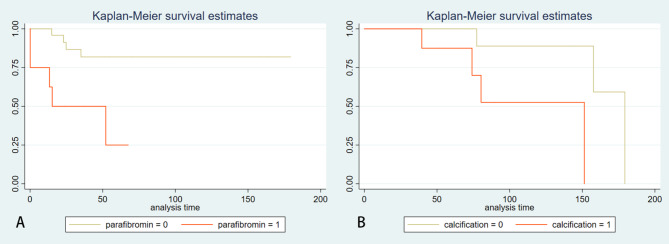 Figure 2
Figure 2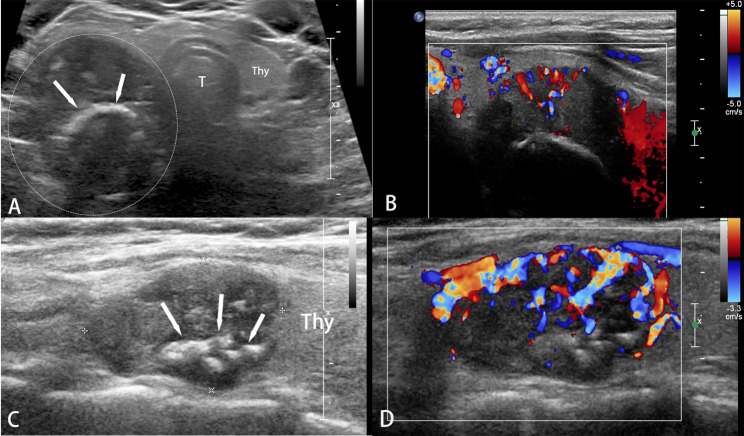 Figure 3
Figure 3- —National High Level Hospital Clinical Research Funding
- —Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences
- —http://dx.doi.org/10.13039/501100012151Sanming Project of Medicine in Shenzen Municipality
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Pancreatic and Hepatic Oncology Research · Bone health and osteoporosis research
Background
Parathyroid cancer (PC) is a rare endocrine disease with recurrence rate ranging from 49 to 82%. Most of the recurrences occurred within 2–5 years after the initial surgery for the primary tumor [1, 2, 3]. Once recurrence initiates, the probability of subsequent multiple recurrences and metastases significantly increases and patients result in death due to uncontrollable complications related to hypercalcemia [4]. Utilizing imaging and pathological information from the primary tumor to predict the prognosis of PC could help to develop a stratified management strategy for postoperative patients.
CDC73 is a tumor suppressor gene located on chromosome 1q31.2, consisting of 17 exons, and its protein product-parafibromin is composed of 531 amino acids. CDC73 was initially found to be widely mutated in Primary Hyperparathyroidism-Jaw Tumor Syndrome, and according to following studies, a significant correlation was discovered between CDC73 and tumor metastasis /invasion in the sporadic parathyroid carcinoma [5]. A systematic review on this topic suggests that the absence of parafibromin staining in the nucleus is a risk factor for poor prognosis in PC patients. In patients over 50 years old, the absence of parafibromin is associated with a shorter overall survival (OS) [6]. Imaging features are commonly used to predict the prognosis of patients with certain disease, often yielding favorable results. However, research about ultrasonographic features of parathyroid carcinoma and patients’ prognosis has not been reported. Considering the recognized value of parafibromin staining in the diagnosis and prognosis of PC, it is worth exploring the combined value of ultrasound (US) features and parafibromin expression for predicting the prognosis of PC patients.
Materials and methods
Subjects
Thirty-four patients diagnosed with parathyroid carcinoma at Peking Union Medical College Hospital from January 2000 to July 2022 were included in this study. The histopathological diagnosis of PC conforms to the 2017 WHO criteria. All cases had complete preoperative ultrasound data, biochemical test data, and immunohistochemical staining information of parafibromin from postoperative pathological specimens. Disease-free survival (DFS) and OS time were collected from medical records or follow-up phone call. The normal ranges of serum calcium level and serum iPTH level in this study are 2.13–2.70 mmol/L and 12–65 pg/mL, respectively. Recurrence was defined when serum calcium levels exceeded the upper normal limit after the previous remission, excluding other pathological conditions. The study was approved by the Ethics Committee of Peking Union Medical College Hospital (S-K1743), and written informed consent was obtained from the participants.
Ultrasound examinations
All the ultrasound examinations were performed by radiologists with over 10 years of experience in the field of thyroid/parathyroid disease. The equipment used was either a 7-15 MHz linear array probe from the HDI 5000 (Philips Medical Systems, Bothell, WA) or a 5-12 MHz linear array probe from the IU22 (Philips Medical Systems, Bothell, WA). Gray-scale and color Doppler ultrasound images of target lesions were reviewed by two radiologists who had undergone professional training in ultrasound evaluation of parathyroid diseases. In cases where there was disagreement between the two radiologists regarding characteristics of a specific lesion, they discussed with a third radiologist with over 20 years of thyroid/parathyroid ultrasonography specialty to determine the final result. The location, size, echogenicity, morphology, boundary, cystic change and calcification of the lesions were recorded according to a predetermined research protocol. The main contents are as follows: location (left, right), size (the maximum diameter measured on the different planes), lesion diameter ratio (DR, the ratio between the lesion’s maximum diameter and minimum diameter on two planes perpendicular to each other), morphology (round or oval, irregular), boundary (clear, infiltrative), and echogenicity of the lesion (homogeneous, heterogeneous).
Immunohistochemical staining
Parafibromin immunohistochemical staining was performed on formalin-fixed, paraffin-embedded tissue samples from primary, recurrent, or metastatic parathyroid carcinoma tumor tissues. The tissue sections were dewaxed, underwent antigen retrieval, and were then soaked in a 3% H2O2 solution to block endogenous peroxidase. Heat-induced antigenic retrieval was performed using an antigen retrieval solution containing ethylenediaminetetraacetic acid (EDTA). After incubating in 3% bovine serum albumin for 30 min to block nonspecific antibody binding sites, the slides were co-incubated with the primary antibodies against parafibromin (ab223840, Abcam, Cambridge, UK) overnight at 4 °C. Then washing the slides with PBS, diaminobenzidine and a secondary antibody working solution coupled with horseradish peroxidase (HRP) (Wuhan Goodbio Technology, China) were used for staining. The sections were counterstained with hematoxylin, differentiated with 0.1% hydrochloric acid ethanol, and rinsed to restore the blue color. They were then dehydrated using graded alcohol solutions and mounted. Each stained section was evaluated by two pathologists without information of the corresponding pathological diagnosis. Parafibromin staining was defined as negative when the staining area of the tumor cell nuclei was less than 10%, while staining was visible in internal controls (vascular endothelial cells and stromal cells). Correspondingly, focal or diffuse staining of tumor cell nuclei (area > 10%) was defined as parafibromin staining positive (Fig. 1).
Fig. 1. Immunohistochemical staining of parafibromin in parathyroid carcinoma tissue sections. A-B Parafibromin-negative parathyroid carcinoma tissue, where staining of the tumor cell nuclei is scarcely observed, while the surrounding endothelial cells show brown staining of the nuclei; C-D: Parafibromin-positive parathyroid carcinoma tissue, where diffuse staining of the tumor cell nuclei is observed
Statistical analysis
Data analysis were completed using SPSS 25.0 (Chicago, IL, USA) and R 3.6.3 (R Foundation for Statistical Computing, www.R-project.org). Continuous variables were expressed as mean ± standard deviation or median ± quartile according to the results of the Shapiro-Wilk normality test. Independent sample t-test or Mann-Whitney U test was used for the comparison between groups. Categorical variables were expressed as the number of cases (percentage), and comparison between groups was performed using ANOVA or Fisher’s exact test. Cox regression was used to identify independent risk factors that significantly affect the overall survival and disease-free survival of patients with parathyroid carcinoma. Based on clinical and past research experience, infiltrative margin, calcification, DR value, iPTH, and parafibromin expression status were selected as candidate variables. Kaplan-Meier survival curves were plotted for variables with prognostic value. A two-tailed p < 0.05 was considered statistically significant.
Results
Among all the 34 patients with PC, twenty-six were categorized as parafibromin-positive (male: female, 12:14), while eight were categorized as parafibromin-negative(male: female, 7:1). The median age (interquartile range) of all cases was 49 (37, 59) years, with a mean follow-up time of 72.6 (11.0-179.3) months. There were 7 deaths (20.6%) and 9 cases (26.5%) of recurrence or metastasis during the follow-up period. The median overall survival time (interquartile range) was 65.7 (35.5, 89.7) months, and the median disease-free survival time (interquartile range) was 38.2 (22.2, 69.7) months. There were no significant statistical differences in patient age, gender, iPTH levels, and blood calcium levels between the positive and negative groups (p = 0.626, p = 0.053, p = 0.465 and p = 0.542). Similarly, there were no statistical differences in various ultrasound features between the two groups, including lesion size, lesion diameter ratio, morphology, echo heterogeneity, infiltrative borders, calcification, and cystic degeneration (p = 0.339, p = 0.583, p = 0.309, p = 0.160, p = 0.152, p = 1.000 and p = 0.693) (Table 1).
Table 1. Comparison of demographic, clinical, and ultrasound parameters between parathyroid carcinomas with positive and negative parafibromin stainingParafibrominpositive (n = 26)Parafibrominnegative (n = 8)P valueMean age (years)49 ± 3149 ± 160.626Gender (male/female)12/147/10.053Serum iPTH (pg/mL)1183.5 ± 8821085.5 ± 12110.465Serum Calcium (mMol/L)3.3 ± 0.73.2 ± 0.80.542Lesion size (cm)3.9 ± 1.53.2 ± 1.20.339DR1.7 ± 0.71.6 ± 0.80.583Shape (irregular/oval)21/58/00.309Echogenicity (heterogeneous/homogeneous)19/78/00.160Infiltration18(69.2%)8(100%)0.152Calcification8(30.8%)3(37.5%)1.000Cystic change13(50.0%)5((62.5%)0.693iPTH, intact parathyroid hormone; DR, the ratio between the lesion’s maximum diameter and minimum diameter measured in all the ultrasound dimensions
In terms of the disease-free survival, the loss of parafibromin expression is an independent risk factor for recurrence and metastasis in patients with parathyroid carcinoma (p = 0.009). The risk of recurrence and metastasis in patients with loss of parafibromin expression is 5.9 times higher than that in patients with evident parafibromin expression (95% CI 1.569–22.190). No statistical differences were calculated in iPTH, DR value, calcification and infiltrative boundaries observed by ultrasound (p = 0.096, p = 0.552, p = 0.362 and p = 0.539). In terms of the overall survival, intralesional calcification detected by ultrasound is an independent risk factor for death in PC patients (p = 0.046). The risk of death during the overall survival period for patients with calcification in the lesion is 9.4 times higher than that for patients without calcification (95% CI 1.037–85.915). No statistical differences were found in iPTH, DR value, parafibromin expression, and infiltrative boundaries either (p = 0.443, p = 0.953, p = 0.667 and p = 0.119) (Figs. 2 and 3).
Fig. 2. The Kaplan-Meier survival curve analysis. A The Kaplan-Meier survival curve shows that PC patients with loss of parafibromin expression (parafibromin = 1) have significantly shorter disease-free survival (DFS) compared with those with positive parafibromin expression (parafibromin = 0) (p = 0.009); B The Kaplan-Meier survival curve indicates that PC patients with calcification in the lesion (calcification = 1) have significantly shorter overall survival (OS) compared with those without calcification (calcification = 0) (p = 0.046)
Fig. 3. Calcification in the parathyroid carcinoma on ultrasonography. A Parathyroid carcinoma of a 45-year-old female with coarse calcification observed in the lesion (arrows); B Color Doppler ultrasound shows abundant blood flow in the lesion; C Parathyroid carcinoma of a 62-year-old female with multiple calcifications detected in the lesion (arrows); D Color Doppler ultrasound shows circumferential and internal blood flow in the lesion. Thy: thyroid; T: trachea
Discussion
Due to the rarity of parathyroid carcinoma, single-center retrospective studies are the mainstream of the field. It is difficult for us to fully understand the natural course and prognosis of this disease. The reported 5-year and 10-year survival rates among Caucasian populations are 78–85% and 49–77%, respectively [7, 8, 9, 10, 11]. According to a study by Obara et al. based on the Japanese population, the median survival time after the first recurrence of parathyroid carcinoma is only 7 years, but no data on deaths during the overall survival period is present [12]. Studies based on Chinese population by Song et al. from Shanghai Ruijin Hospital and Hu et al. from Peking Union Medical College Hospital suggest that the 5-year and 10-year overall survival rates for patients with parathyroid carcinoma are 78.9-90.2% and 60.7-77.9% [13, 14], respectively. Thus, precise stratification of prognosis in the early stage is crucial for the postoperative monitoring of parathyroid carcinoma.
Many studies have conducted exploratory analyses on prognostic risk factors for parathyroid carcinoma. The Schulte TNM staging system and Schulte Risk Classification are important contributions, which use the degree of invasion into surrounding tissues and vital organs as the main staging criteria. Both systems indicate a significant increase in recurrence and mortality risk for patients with T3-T4 staging or high-risk classification [15, 16]. Other notable influencing factors include age, extent of surgical resection, preoperative parathyroid hormone and blood calcium levels, parafibromin and Ki-67 expression in pathological specimens. Nevertheless, the potential value of imaging for predicting the prognosis of parathyroid carcinoma is unexplored, but worthwhile. Studies about the correlation between medical imaging features and the prognosis of certain diseases are common and have yielded many meaningful results. Our research also suggests that calcification identified by US within the primary PC lesion is an independent risk factor affecting the overall survival of patients with parathyroid carcinoma. It also reconfirms that parafibromin is an independent risk factor for recurrence and metastasis of parathyroid carcinoma. Both factors play vital roles in the natural course of PC.
Mutations in the tumor suppressor gene CDC73 represent one of the essential molecular mechanisms about the onset of parathyroid carcinoma. Germline mutations in CDC73 are closely associated with hyperparathyroidism-jaw tumor syndrome (HPT-JT), which lead to the loss of parafibromin, a kind of protein consisting of 531 amino acids. Parafibromin functions as a tumor suppressor by inducing apoptosis and inhibiting cell cycle-its absence results in overexpression of Cyclin D1 [17]. Ruizhe Zhu et al., through a systematic review and meta-analysis based on individual patient data, found that negative parafibromin immunohistochemical staining is an independent risk factor for recurrence/metastasis (HR 2.73, p = 0.002) and death (HR 2.54, p = 0.004) in patients with PC, while CDC73 gene mutations were not significantly correlated with any clinical outcomes [18]. In this study, the loss of parafibromin expression was significantly associated with a shorter disease-free survival but not with the overall survival. Davies et al. suggested that parafibromin can be present in either the nucleus or cytoplasm of chief cells of parathyroid tumor [19]. Inspired by facts stated above, we raise the hypothesis that the localization of parafibromin may influence the prognosis of PC patients in different ways, which represents a direction for future research.
Tumor calcification is a pathological mineralization process that shares many similarities with physiological mineralization (such as bone formation and remodeling). Existing research regarding this topic is not consolidated, and there are many controversies concerning the chemical composition of deposited minerals, crystal characteristics, participating cells and intracellular regulation, gene expression characteristics, mineralization timeline, and other aspects. Nevertheless, some studies suggesting that deposited minerals affect tissue interactions, thereby participating in disease progression, provide valuable insights for us [20]. Calcification within parathyroid lesions is relatively rare, and there is no study reporting its formation mechanism or prognostic impact to our knowledge. For discussion, we can refer to the field of breast cancer microcalcifications, which has yielded significant findings. It assists in exploring the possible reasons of the poor prognosis of PC patients with calcification in the lesion [21]. The chemical substances that constitute breast cancer microcalcifications mainly include calcium oxalate and calcium phosphate, with disparities in molecular formulas, such as (Ca)10(PO4)6(OH)2, Ca3(PO4)2, Ca8H2(PO4)6·5H2O, etc [22, 23]. The microscopic differences behind the similar imaging manifestations may account for the heterogeneity in the prognosis of patients with the same characteristic-calcification. The formation of calcification can be understood as an imbalance between promoting and inhibiting factors caused by changes in the microenvironment. Factors promoting calcification include overexpression of the BMP2 gene, inflammation, oxidative stress, necrosis, and metalloproteinase expression, etc., while inhibiting factors include magnesium ions, osteopontin, etc. The imbalance between them leads to a cellular phenotypic shift towards osteogenesis, resulting in mineral deposition [24]. The relationship between microcalcification and the prognosis of breast cancer is mainly reflected in three aspects: increased risk of death (mainly cast calcification), increased risk of recurrence, and increased HER2 expression (high consistency among researches) [25, 26, 27, 28]. In vitro and in vivo studies indicate that this may be related to mechanisms such as microcalcification promoting cell mitosis, enhancing cell migration ability, mediating high expression of inflammatory factors, promoting epithelial-mesenchymal transition, and regulating immune monitoring [29, 30]. Given all above, we speculate that calcification in parathyroid carcinoma may reflect dramatic changes of intratumoral microenvironment-greater oxidative stress, higher inflammation levels, and increased necrosis. Calcification itself may also interact with tumor cells to form a cascade reaction, further increasing tumor invasiveness, leading to a poor prognosis of the patient.
Conclusions
In conclusion, our study firstly reveals that calcification in the parathyroid carcinoma detected by preoperative US may be related to worse overall survival among PC patients, and we also confirm that the parafibromin significantly affects disease-free survival.