Case Report: Giant lung hamartoma : An usual cause of lobectomy in a five-year child
Sabrine Louhaichi, Besma Hamdi, Imen Bouacida, Yessmine Haddar, Sarra Trimech, Jamel Ammar, Aida Ayadi, Agnès Hamzaoui, Baccouche Ines, Adel Marghli, Duc T Nguyen, Kenneth J. Nobleza, Hüseyin Fatih Sezer

TL;DR
A 5-year-old child had a large benign lung tumor removed through surgery after experiencing repeated lung infections.
Contribution
This case report highlights a rare instance of a giant pulmonary hamartoma in a young child requiring surgical intervention.
Findings
A giant lung mass was diagnosed in a 5-year-old child causing recurrent pneumonia.
Surgical resection confirmed the diagnosis of a pulmonary hamartoma with specific histological features.
Abstract
Pulmonary hamartomas are the most common benign tumors of the lung in adults. They are usually asymptomatic because of their small size and their slow-growing character. We report the case of a 5-year-old child presenting with a giant lung mass causing recurrent right pneumonia. Surgical resection with middle lobectomy was performed. Final histology revealed pulmonary hamartoma with predominant adenofibromatous and lipomatous differentiation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
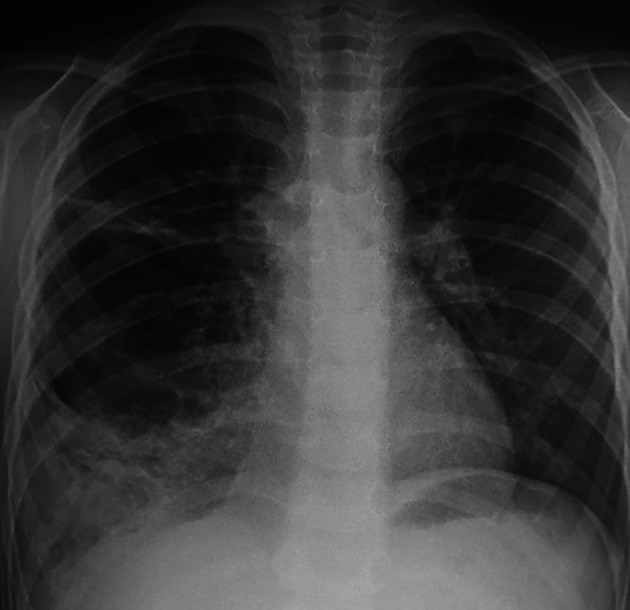 Figure 1
Figure 1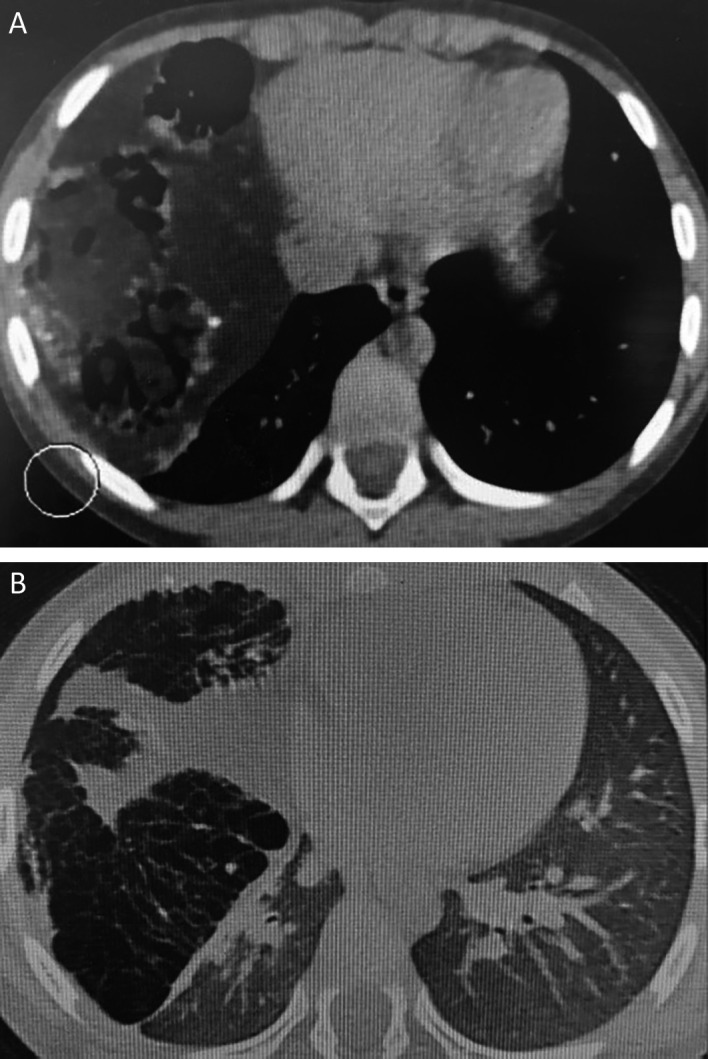 Figure 2
Figure 2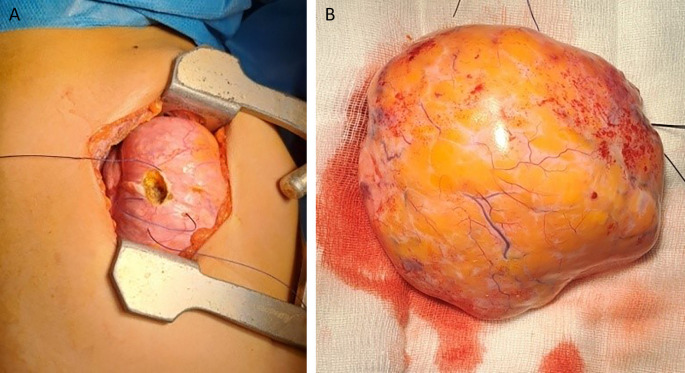 Figure 3
Figure 3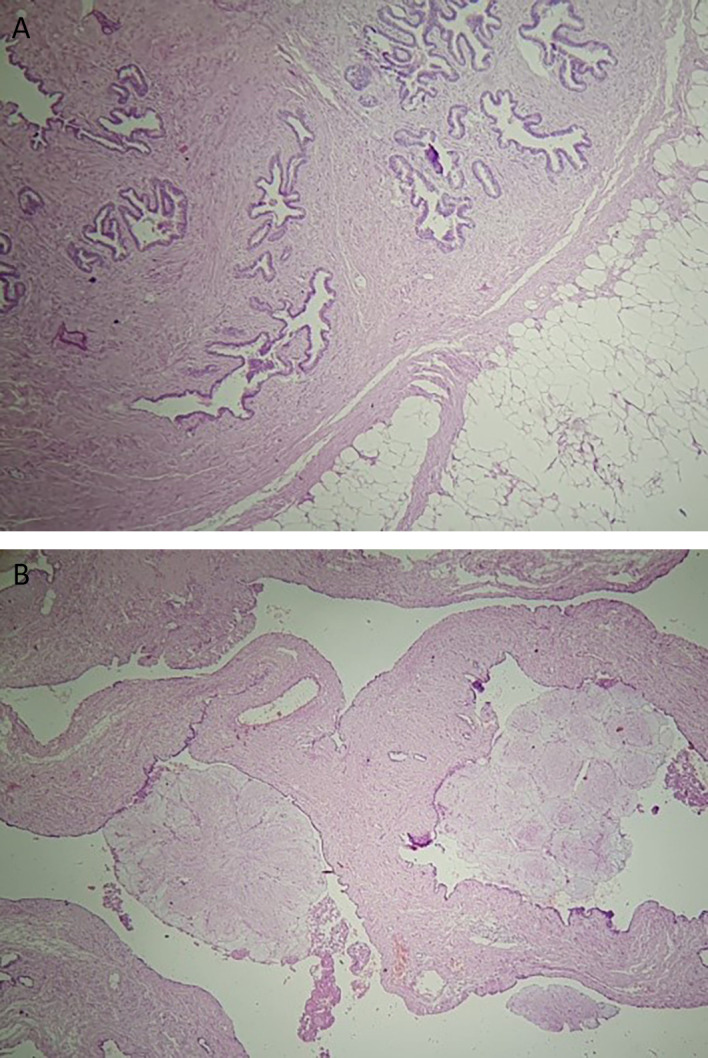 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Imaging and Pathology Studies · Soft tissue tumor case studies · Tumors and Oncological Cases
Introduction
Lung hamartomas are benign pulmonary tumors characterized by an incidental finding in most cases. ^ 1 ^ Compocased of a mixture of variant mesenchymal elements, it is more frequently seen in male adults. Pediatric cases are extremely rare. ^ 2 ^ ^–^ ^ 3 ^ Herein we report the case of a pulmonary hamartoma revealed by persistent pneumonia in a five-year-old child.
Case report
A five-year-old child was referred to our department in September 2023 because an abnormal pulmonary density of the lower right hemithorax. His past medical history revealed recurrent admissions for right pneumonia during the last two years. The patient complained of chronic productive cough without chest pain or hemoptysis. Physical examination did not reveal abnormalities apart from a decrease in breath sounds in the right lung. Chest radiography revealed a heterogeneous right opacity above the diaphragm as showed in Figure 1.
Chest radiograph view demonstrating a heterogeneous opacity in the middle and lower zones of the right lung.
Chest computed tomography revealed a giant cystic and solid mass measuring 122 × 80 × 102 mm compressing the right middle and lower lobes. This mass contained tissular, fatty, and calcified elements, along with multiple airy cysts, suggesting a giant pulmonary hamartoma ( Figure 2).
Pulmonary hamartoma: a contrast-enhanced lung CT scan is showing a large, lobulated soft-tissue density mass with foci of low attenuation and calcification with compression of the right lower lobe in mediastinal window (A) and lung window (B).
The patient underwent flexible bronchoscopy, which ruled out endobronchial development of the mass. Cytological examination of the bronchial aspiration fluid revealed negative results for malignancy. Common bacterial and acid-fast bacilli cultures were also negative, and surgery was performed. The patient underwent a right lateral thoracotomy. During exploration, the mass occupied two-thirds of the right thorax and compressed the upper and lower lobes ( Figure 3). It depended on the middle lobe, which appeared as a small strip of destroyed lung parenchyma, and atypical resection of the mass followed by a complete right middle lobectomy was performed. The postoperative course was uneventful, and the patient was discharged seven days later.
Resection of the tumor (A). The hamartoma after resection (B).
The final histology of the tumor showed a well-circumscribed mass measuring 14 × 10 × 5 cm, with predominantly adenofibromatous and lipomatous differentiation, calcifications, and ossified lesions ( Figure 4). There was no evidence of cartilage or muscle tissue. The tumor was covered by a thin fibrous capsule. Additionally, diffuse alveolar hemorrhage lesions were observed in the middle lobe. Follow-up at three weeks post-surgery indicated no adverse outcomes.
HE40 Pulmonary hamartoma with adenofibromatous proliferation associated adipose tissue (A) Adenofibromatous pattern with cystic changes and club-like papillae set against a collagenous stroma (B).*
Discussion
Pulmonary hamartomas are benign tumors that often occur in middle-aged adults with male predominance. ^ 4 ^ Within the pediatric population, pulmonary hamartomas are significantly rarer. ^ 5 ^ It is an incidental finding in most cases, with a diameter ranging from 1 to 8 cm. ^ 6 ^ This type of tumor has never been reported as a congenital lesion. Cytogenetic analysis showed abnormalities in chromosomal bands 6p21, 12q14–15, or other regions corresponding to mutations in high-mobility group (HMG) proteins. This group of proteins plays an important role in regulating chromatin architecture and gene expression. ^ 7 ^
The pathological pattern of the tumor usually shows predominant chondroid differentiation with a mixture of adipose tissue, fibrous tissue, smooth muscle, and bone, along with entrapped respiratory epithelium . Immunohistochemical staining is not necessary for the diagnosis. ^ 8 ^ In other cases, the major component can define various subtypes of the tumor: lipomatous, adenoleiomyomatous, and fibrous hamartomas. ^ 7 ^ ^,^ ^ 9 ^ In the current case, the tumor consisted histologically of glandular lumens and fibrous tissue with some calcifications. No evidence of cartilage or muscle tissue damage was observed.
Pulmonary hamartomas are typically asymptomatic. The patient had a medical history of recurrent pneumonia before being referred to our department. Respiratory infections may occur because of mechanical obstruction of the bronchus.
On tomodensitometry, lung hamartoma usually appears as a lobulated nodule with a heterogeneous density and no pleural traction. Characteristic imaging manifestations include the presence of fat (60% of the cases) and a popcorn appearance of calcifications observed in 5-50% of the cases. ^ 10 ^ Malignant transformation is exceedingly rare. ^ 11 ^
Surgery is indicated for symptomatic masses or those in which malignancy cannot be excluded. ^ 12 ^ ^,^ ^ 13 ^ Enucleation and wedge resection are the most common surgical choices for preserving functional lung tissue. ^ 14 ^ However, in our case, tumor resection and middle lobectomy were mandatory because of the large size of the tumor and compression of the surrounding parenchyma.
Conclusions
Lung hamartomas typically occur in adults and are asymptomatic in most cases; parenchymal resection is rarely required when surgery is indicated. Our case is unusual because of its many peculiarities. A 5-year-old child presented with recurrent pneumonia. Moreover, owing to its large size, the tumor caused parenchymal damage, leading to middle lobectomy during surgery. Finally, the tumor was characterized by predominant adenofibromatous differentiation, with no cartilage. Knowledge of atypical presentations of this neoplasm is crucial to avoid misdiagnosis and to guide appropriate surgical treatment, especially in pediatric patients.
Consent
Written informed consent was obtained from the patient’s parents for the publication of this case report and accompanying images.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shukla I Stead TS Aleksandrovskiy I : Symptomatic Pulmonary Hamartoma. Cureus. 2021;13(9):e 18230. 10.7759/cureus.18230 34692355 PMC 8526074 · doi ↗ · pubmed ↗
- 2Pouessel G Thumerelle C Santos C : Pulmonary hamartochondroma: a rare cause of solitary pulmonary nodule in children. J. Radiol. 2005;86:79–82. 10.1016/S 0221-0363(05)81326-5 15785421 · doi ↗ · pubmed ↗
- 3Zapala MA Ho-Fung VM Lee EY : Thoracic Neoplasms in Children: Contemporary Perspectives and Imaging Assessment. Radiol. Clin. North Am. 2017;55(4):657–676. 10.1016/j.rcl.2017.02.008 28601174 · doi ↗ · pubmed ↗
- 4GrigoraşA Amălinei C Lovin CS : The clinicopathological challenges of symptomatic and incidental pulmonary hamartomas diagnosis. Romanian J. Morphol. Embryol. 2022;63(4):607–613. 10.47162/RJME.63.4.02 36808195 PMC 10028331 · doi ↗ · pubmed ↗
- 5Saadi MM Barakeh DH Husain S : Large multicystic pulmonary chondroid hamartoma in a child presenting as pneumothorax. Saudi Med. J. 2015;36(4):487–489. 10.15537/smj.2015.4.10210 25828288 PMC 4404485 · doi ↗ · pubmed ↗
- 6Ganti S Milton R Davidson L : Giant pulmonary hamartoma. J. Cardiothorac. Surg. 2006;1:19. 10.1186/1749-8090-1-19 16887035 PMC 1552053 · doi ↗ · pubmed ↗
- 7Wick MR : Hamartomas and other tumor-like malformations of the lungs and heart. Semin. Diagn. Pathol. 2019;36(1):2–10. 10.1053/j.semdp.2018.11.002 30473462 · doi ↗ · pubmed ↗
- 8Hashimoto H Tsugeno Y Sugita K : Mesenchymal tumors of the lung: diagnostic pathology, molecular pathogenesis, and identified biomarkers. J. Thorac. Dis. 2019;11(Suppl 1):S 9–S 24. 10.21037/jtd.2018.12.04 30775024 PMC 6353741 · doi ↗ · pubmed ↗