A coronary coronary-to-coronary fistula around the main pulmonary artery
Stefan Gherca, Gregor Leibundgut, Jokin Zubizarreta-Oteiza, Philip Haaf

TL;DR
This paper describes a rare coronary-to-coronary fistula around the pulmonary artery and discusses its clinical implications.
Contribution
The study presents a unique case of a coronary-to-coronary fistula involving the main pulmonary artery.
Findings
Coronary-to-coronary fistulas are rare and often detected incidentally.
Management depends on symptoms, with asymptomatic cases typically requiring observation.
Abstract
Coronary-to-coronary fistulas are rare anomalies, often detected incidentally. These fistulas may involve complex vascular connections around major cardiac structures, such as the pulmonary artery. Functional assessments help determine clinical significance, with management typically involving observation for asymptomatic patients, while symptomatic cases may require intervention to prevent complications. The online version contains supplementary material available at 10.1007/s10554-024-03269-7.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
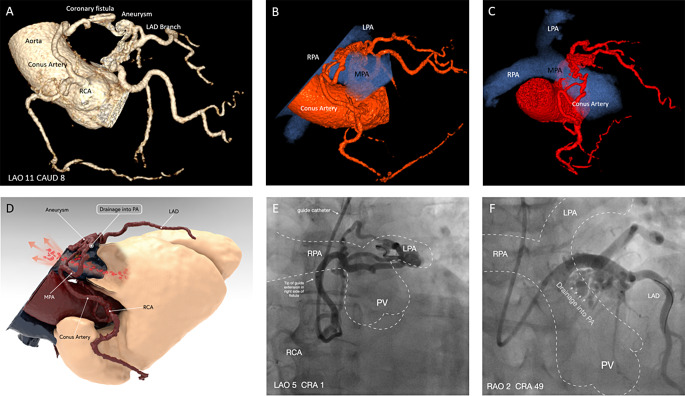 Figure 1
Figure 1- —University of Basel
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Artery Anomalies · Congenital Heart Disease Studies · Vascular anomalies and interventions
A 63-year-old female with recurrent, atypical chest pain underwent coronary computed tomography angiography (CCTA), which ruled out obstructive coronary artery disease (CAD). CCTA revealed a complex coronary-to-coronary fistula encircling the main pulmonary artery (MPA), fed by a conus artery from the right coronary artery (RCA) and a branch from the proximal left anterior descending artery (LAD). A coronary aneurysm (15 × 15 mm) of the LAD branch suggested a direct communication between RCA and LAD with drainage into the MPA (Fig. 1A-D; Supplement Video S1).
Invasive coronary angiography confirmed the ring-like coronary-to-coronary fistula draining into the MPA (Fig. 1E, F; Supplement Video S2, S3). Fractional flow reserve (FFR) revealed a steal phenomenon in the distal RCA (FFR = 0.74) but not in the distal LAD (FFR = 0.90). Rubidium Positron Emission Tomography showed no scar or ischemia and normal myocardial blood flow reserve (Supplemental Figure 1).
Based on these findings, the patient’s age, and her preferences, a conservative approach was chosen.
Coronary fistulas, often resulting from embryological defects, typically drain into low-pressure vasculature [1]. The widespread use of CCTA has led to more frequent detection of these fistulas [2]. Haemodynamically significant fistulae causing symptoms should be treated interventionally or surgically [3], while asymptomatic patients with small fistulas are usually managed conservatively [1].
Fig. 1. Panel (A) Coronary computed tomography angiography 3D volume rendering of the coronary-to-coronary fistula forming a complete circle around the main pulmonary artery (MPA not displayed). (B, C) Computed tomography 3D model showing the anatomy of the coronary-to-coronary fistula and its relationship with the pulmonary arteries. (D) Computed tomography 3D volume rendering of the fistula in relation to MPA. (E, ** F)** Invasive coronary angiography in different angulations with sketch of course of the pulmonary arteries and site of drainage of the coronary fistula into the main pulmonary artery
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4