Left nasal reconstruction using a concha cartilage for loss of substance post human bite: A case report
Boboe Jordan, Valimungighe Moise Muhindo, Yevide Agossou Barthelemy, Gbessi Mahugnon Emmanuel, Gbessi Dansou Gaspard, Jeannot Baanitse

TL;DR
This case report describes the successful use of conchal cartilage to reconstruct a nasal defect caused by a human bite injury.
Contribution
The paper highlights the effectiveness of conchal cartilage in nasal reconstruction with minimal donor site complications.
Findings
Conchal cartilage is suitable for reconstructing transfixing nasal substance loss.
The use of conchal cartilage results in minimal donor site morbidity.
A composite graft with conchal cartilage provides satisfactory aesthetic outcomes.
Abstract
Conchal cartilage is recommended for correction of substance loss of the nose. Transfixing nose substance loss presents an anatomical, functional, and aesthetic restoration challenge. The rate of complications associated with concha cartilage harvesting using a retroauricular approach is low. A 24-year-old presented with nose damage and loss of transfixing substance after being intentionally assaulted and injured (human bite during a fight). He underwent a nose wing reconstruction using a composite transplant from the auricular cartilage. Post-operative recovery was uneventful. Nonetheless, a minor disparity existed between the flap and the natural nasal wing. The three-dimensional anatomy of the nasal wing makes the aesthetic reconstruction of the transfixing loss of substance of the entire unit very difficult to achieve, especially when the reconstructed wing will be constantly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2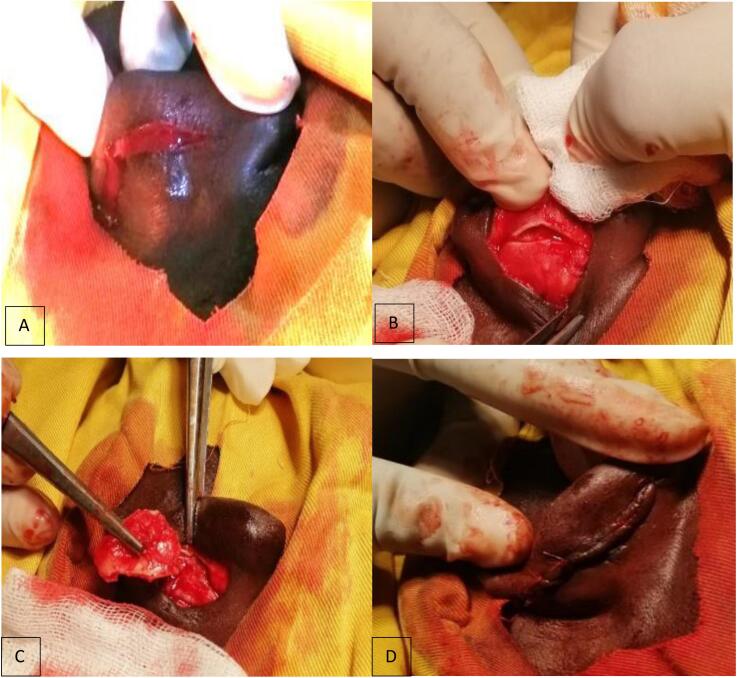 Figure 3
Figure 3 Figure 4
Figure 4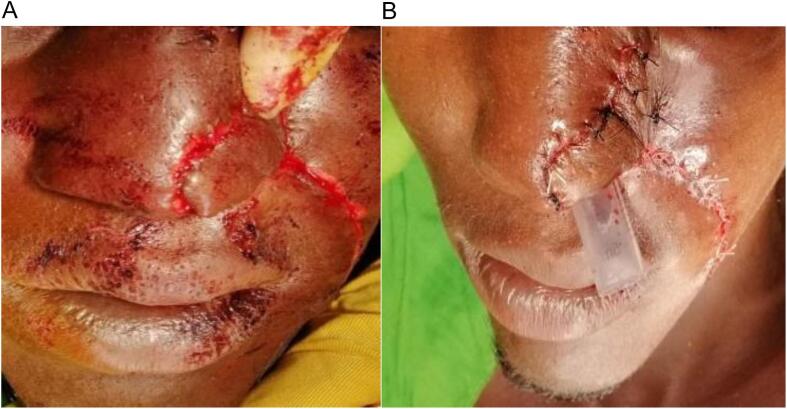 Figure 5
Figure 5 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRabies epidemiology and control · Tattoo and Body Piercing Complications · Facial Rejuvenation and Surgery Techniques
Introduction
1
One of the most important and aesthetic organs of the face is the nose. Transfixing nose substance loss presents an anatomical, functional, and aesthetic restoration challenge. Post-traumatic rhinoplasty, is a surgical procedure that treats the sequelae of nasal trauma to improve the function and shape of the post-traumatic nose [1]. Conchal cartilage is generally favored in rhinoplasty with a satisfied aesthetic outcome [2]. The nasal rehabilitation aims at improved function and aesthetic of patients with facial deformations resulting in considerable cosmetic impairment. The aim of this report was to describe the nasal rehabilitation, in which the Retroauricular cartilaginous graft harvest from the left ear's concha [1,3]. The work has been reported in line with the SCARE criteria [4].
Clinical observation
2
A 24-year-old male patient with no specific past medical history was brought to the emergency room due to nasal trauma and substance loss by intentional assault and injury (a human bite during a fight). Two hours after the incident, he was referred to our hospital after consulting at two other health institutions. A transfixing loss of substance from the left wing of the nose, with damaged edges, measuring about 3 × 4 cm, was noted during the physical examination at admission (Fig. 1). The base of the wing was unaffected.Fig. 1. Transfixed wound of the nose's left wing after washing the wound.Fig. 1
Additionally, we discovered abrasions on the right forearm during physical examination.
The decision was taken to use a composite auricular cartilage transplant for nose reconstruction. He was transferred to the operating room following consent and prophylactic tetanus treatment. We debrided the lesion under local anesthesia while minimizing further tissue loss (Fig. 2).Fig. 2. Wound after debridement.Fig. 2
Next, a 3.5 × 1.5 cm rectangular piece of concha cartilage was harvested from the ipsilateral ear using the posterior approach (Retroauricular approach) (Fig. 3). After harvesting the concha cartilage, hemostasis was achieved using Vicryl suture 2–0 and nylon suture 2–0, using interrupted suture. Using 4/0 non-absorbable suture, the transplant was secured as a bridge to the remaining wing cartilages.Fig. 3. Retro-auricular cartilaginous graft harvest from the left ear's concha, where A) shows the incision through the skin of the left posterior ear. B) shows the incision through the concha cartilage. C) shows the harvest of the conchal cartilage, and D) shows the closed wound after harvesting the cartilage.Fig. 3
Next, we elevated a nasolabial flap on the angular artery using a superior pedicle (Fig. 4).Fig. 4. Harvesting the naso-labial flap to cover the concha cartilage.Fig. 4
To restore the mucosal side, it was first degreased and then folded. Two planes (layers) of the flap were secured and sutured with 3/0 absorbable suture. 3/0 absorbable suture was used to suture the donor region in two layers. For seventy-two hours, a plastic tube was inserted into the left nostril to keep the shape of the nose (Fig. 5).Fig. 5. Naso-labial flap fixation with the tube inserted in the left nostril. A) shows the fixation of the naso-labial flap before suturing it. B) shows the fixed naso-labial flap with a tube inserted in left nostril to maintain the normal shape.Fig. 5
Ten days of antibiotic treatment (Ceftriaxon 2 g daily for 10 days to prevent any post -operative infection) were recommended after surgery. On the tenth day post operation, the donor area had healed satisfactorily, and the flap had successfully integrated into the nasal pyramid (Fig. 6). Nonetheless, a minor disparity existed between the flap and the natural nasal wing.Fig. 6. Healed naso-labial flap recipient and donor locations at D-10 post-op. A–B) show a healed naso-labial flap at Day 10 post- operative when the patient came for stitch removal. C) shows the healed wound of the harvested part in retro-auricular.Fig. 6
Follow up
3
Post-operative recovery was uneventful. The patient was discharged on post-operative day 14 after removal of stitches. The nose wound had healed properly on the 21st day after discharge, no complication occurred in the follow up.
Our study was conducted in a teaching hospital and the surgery was performed by a senior consultant general surgeon with another general surgeon as an assistant.
Discussion
4
Loss of substances from the nasal pyramid most often occurs following excision of skin carcinomas in subjects with a white or light phototype [3]. The three-dimensional anatomy of the nasal wing makes the aesthetic reconstruction of the transfixing loss of substance of the entire unit very difficult to achieve, especially when the reconstructed wing will be constantly confronted and compared to the contralateral wing [5]. The chondrocutaneous graft is the most judicious choice for loss of substances less than or equal to 1 cm [6,7].
The nasolabial flap, ideally reinforced by a cartilaginous frame [8], the strengthened or reinforced forehead flap or the Schmid-Meyer flap [6] and repairs in three layers: mucosal, cartilaginous and cutaneous [2,8], take the lead in losses of more important substances [3]. Classically we distinguish 2 types of nasolabial flap, either with a superior pedicle [9], as in our case, or with a lower pedicle [1,9]. Several authors describe nasolabial flap techniques such as Pers, Burget, Spear and Préaux, [8]. We used the latter technique in our case report. Because it may be finished in a single step, it is the preferred method for substance loss in the centro-facial region. Technically, raising the flap is simple and has good vascular reliability [1,5]. The nose may appear straight and well-corrected on the operating table, but may re-deviate during healing [1,11].
Complications can occur, some of a general nature, inherent to any surgical procedure, others loco-regional more specific to the reconstruction of the upper aero-digestive tracts [10]. Infection, hematoma, suture disunity, partial distal necrosis of the flap and healing disorders [10,11]. As a disadvantage, possible edema, linked to its counter-current venous vascularization may persist for several weeks. Possible retraction may be bothersome in this location where the skin is thin. Sometimes secondary degreasing may occasionally be feasible [2,9]. Concha cartilage is recommended for correction of cleft nasal deformities of trauma. Morbidities at the donor site have been reported in aesthetic rhinoplasty cases [12].
Conclusion
5
Nose reconstruction with a concha cartilage transplant and a nasolabial flap is still a straightforward option for reconstructing the nose's wing in a low income country. Concha cartilage is a good choice for nasal's wing reconstruction and mostly recommended.
CRediT authorship contribution statement
BJ, YAB, GM and GB managed the patient and wrote the first draft. VM and JB helped in editing and reviewing the paper. All authors read and approved the final version to be published.
Consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Not applicable.
Strength and weakness of the study
Strength of the study: clear and concise data on nasal wing reconstruction with excellent iconographies are mentioned in this case presentation.
Weakness of the study: The discussion is not detailed very well. There is no much literature search on recommendations and results from previous publications.
Guarantor
Jeannot Baanitse.
Research registration number
Not applicable.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Funding
There was no external funding source for this report.
Declaration of competing interest
The authors declare no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berrezouk M.Kamal F.M.Maidam S.Lakouichmi M.Abouchadi A.Principles and techniques of post-traumatic rhinoplasty: a review of the literature Modern Plastic Surgery 1420247486
- 2Li Q.Chen Z.Jiang Z.Deng J.Cui W.Cai Z.Sheng Y.A novel conchal cartilage harvesting technique Aesth. Plast. Surg.4815 Aug 20242941295010.1007/s 00266-024-03958-738519571 · doi ↗ · pubmed ↗
- 3Amegble K.J.D.Amana E.Diabo K.W.Gayito Adagba R.A.Rhinopoièse partielle post-traumatique chez un adulte jeune J. Tun Orl 492023
- 4Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int J Surg Lond Engl.10952023113610.1097/JS 9.0000000000000373 PMC 1038940137013953 · doi ↗ · pubmed ↗
- 5Belmahi A.Rhinopoièses esthétiques triplan de l’unité de l’aile après ablation de lésions basocellulaires évoluées. À propos de 26 cas Ann. Chir. Plast. Esthet.671202226343512078110.1016/j.anplas.2021.10.002 · doi ↗ · pubmed ↗
- 6Deranque C.Rouffet A.Dejean M.Rousseau P.Reconstruction des pertes de substances du nez: algorithme décisionnel à propos de 229 cas Ann. Chir. Plast. Esthet.67120227133507867410.1016/j.anplas.2021.12.002 · doi ↗ · pubmed ↗
- 7Jun Arata Yamashita Teruyo Suzuki Mayu Rhinoplasty for post-traumatic deviation of the nose with non-incisional external perforated osteotomy J. Plast. Reconstr. Aesthet. Surg.952024 P 124P 12610.1016/j.bjps.2024.06.00838905788 · doi ↗ · pubmed ↗
- 8Nemoto T.Matsui Y.Shirota T.Irie T.Tachikawa T.Two cases of scar formation in donor site for conchal cartilage grafting J Jpn, Stomatol Soc 572008278282