Fatal Seatbelt Syndrome in an Elderly Wheelchair User: A Case Report
Yuki Sugitani, Akihiro Yashio, Ayumu Kuwahara, Hiroya Chiba, Masahito Hitosugi

TL;DR
An elderly wheelchair user died from injuries caused by a poorly aligned seatbelt after a minor collision, highlighting the need for better safety systems and trauma care guidelines for this vulnerable group.
Contribution
This case report highlights the risks of seatbelt syndrome in elderly wheelchair users and suggests improvements in restraint systems and trauma care protocols.
Findings
A 90-year-old wheelchair user suffered fatal abdominal injuries consistent with seatbelt syndrome after a low-speed collision.
REBOA and emergency thoracotomy had limited success in stabilizing the patient, underscoring their limited efficacy in geriatric blunt trauma.
The case emphasizes the need for improved seatbelt systems and trauma care guidelines for elderly wheelchair users.
Abstract
Elderly wheelchair users face unique challenges in traffic collisions due to physiological fragility and the limitations of standard vehicle seatbelt systems. Seatbelt syndrome, a pattern of abdominal organ and spinal injuries, can be severe when seatbelts do not properly align with an individual's body configuration. Moreover, geriatric out-of-hospital cardiac arrest (OHCA) has a low survival rate, even with advanced prehospital care. This case study presents a 90-year-old woman, secured in her wheelchair with a two-point lap belt, who was involved in a low-speed rear-end collision. Initially alert, she rapidly deteriorated into shock and subsequently exhibited pulseless electrical activity (PEA), ultimately leading to her demise despite attempts at resuscitation using resuscitative endovascular balloon occlusion of the aorta (REBOA) and emergency thoracotomy. Postmortem examination…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
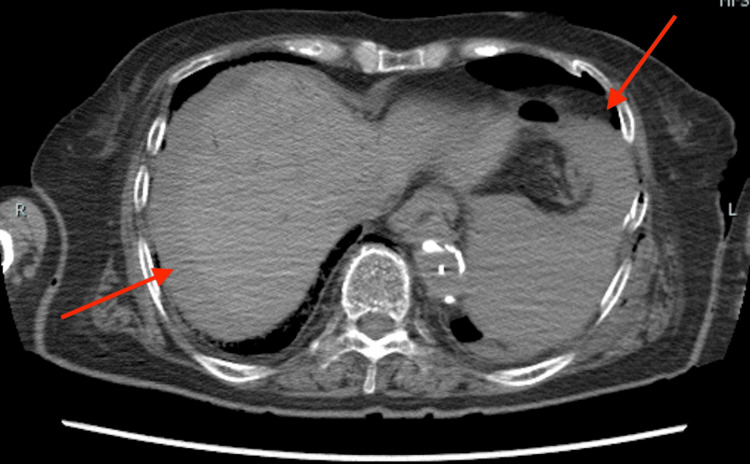 Figure 1
Figure 1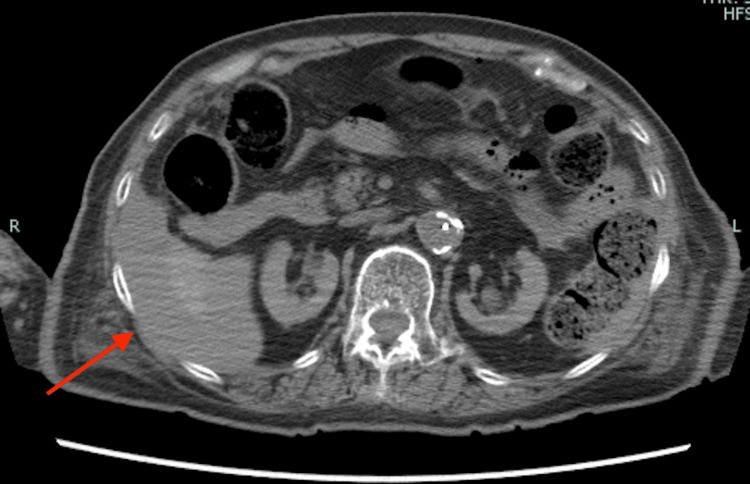 Figure 2
Figure 2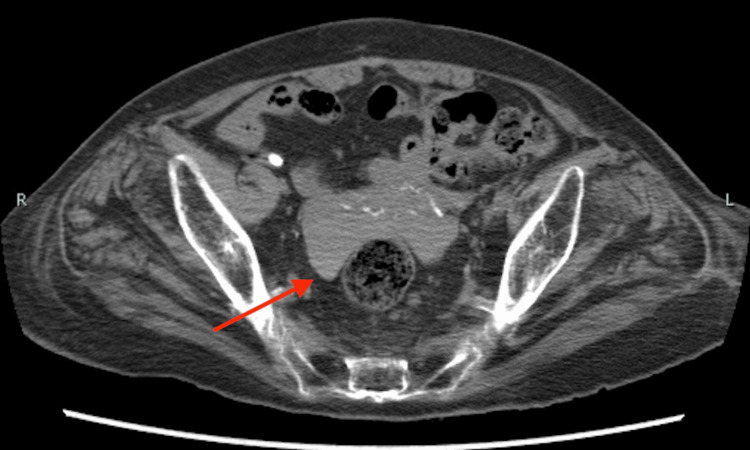 Figure 3
Figure 3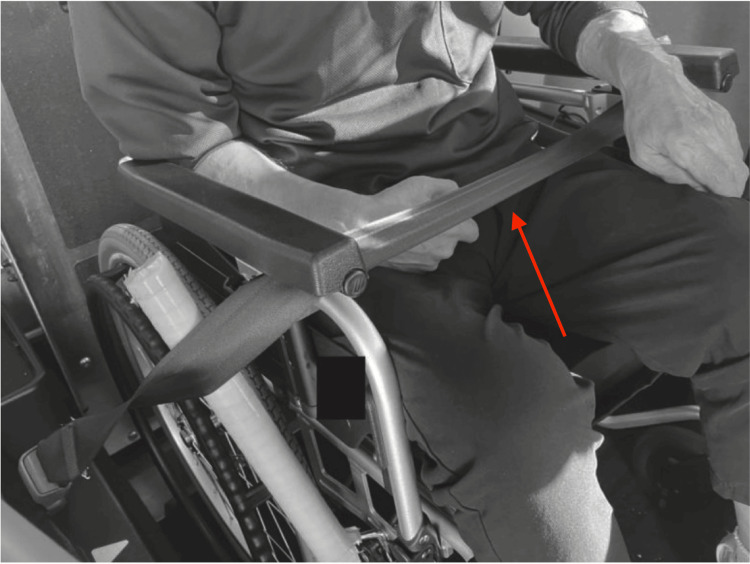 Figure 4
Figure 4| Time | Event |
| 10:30 | Accident occurred |
| 10:42 | EMS contacted |
| 10:52 | EMS arrival: GCS 3, RR 12 breaths/min, HR 99 bpm, BP 70/59 mmHg |
| 10:56 | Assisted ventilation initiated |
| 11:03 | Transport commenced; sought shock-management guidance |
| 11:07 | PEA confirmed→CPR begun |
| 11:13 | Laryngeal tube inserted |
| 11:17 | IV access established |
| 11:18 | IV epinephrine 1 mg administered |
| 11:19 | Arrival at the receiving hospital |
| Patient value | Reference range | |
| ABG | ||
| pH | 6.999 | 7.35-7.45 |
| pCO₂ (mmHg) | 22.4 | 35-45 |
| pO₂ (mmHg) | 218.6 | 75-100 |
| Na (mEq/L) | 139 | 135-145 |
| K (mEq/L) | 5.9 | 3.5-5.0 |
| Cl (mEq/L) | 119 | 98-106 |
| Ca²⁺ (mmol/L) | 1.06 | 1.12-1.32 |
| Glucose (mg/dL) | 152 | 70-99 |
| Lactate (mmol/L) | 15.5 | 0.5-2.2 |
| HCO₃⁻ (mEq/L) | 5.4 | 22-29 |
| CBC | ||
| WBC (/µL) | 9900 | 4500-11,000 |
| RBC (×10⁶/µL) | 1.97 | 4.2-5.4 |
| Hemoglobin (g/dL) | 6.1 | 12-15.5 (F), 13.5-17.5 (M) |
| Hematocrit (%) | 20.3 | 37-47 (F), 42-52 (M) |
| Platelets (×10³/µL) | 41 | 150-400 |
| Coagulation | ||
| APTT (seconds) | >180 | 30-40 |
| Fibrinogen (mg/dL) | 34 | 200-400 |
| D-dimer (µg/mL) | 399.6 | <0.5 |
| Others | ||
| CK (U/L) | 86 | 55-170 |
| AST (U/L) | 262 | 10-40 |
| ALT (U/L) | 168 | 7-56 |
| LD (U/L) | 755 | 122-222 |
| γGTP (U/L) | 5 | 9-48 |
| ChE (U/L) | 66 | 4.6-11.2 |
| Total bilirubin (mg/dL) | 0.2 | 0.1-1.2 |
| Direct bilirubin (mg/dL) | 0.1 | 0.0-0.3 |
| Total protein (g/dL) | 2.9 | 6.4-8.3 |
| Albumin (g/dL) | 1.3 | 3.5-5.0 |
| BUN (mg/dL) | 13 | 7-20 |
| Creatinine (mg/dL) | 0.58 | 0.6-1.2 |
| CRP (mg/dL) | 0.17 | <0.5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma Management and Diagnosis · Trauma and Emergency Care Studies · Traumatic Ocular and Foreign Body Injuries
Introduction
In geriatric trauma, physiological vulnerability, multiple comorbidities, and skeletal fragility are well-known risk factors that lead to markedly poor outcomes, particularly in cases of out-of-hospital cardiac arrest (OHCA) [1,2]. Because older adults often lack sufficient physiological reserve to cope with severe injuries or prolonged shock, even relatively minor trauma can precipitate life-threatening complications.
Elderly patients who rely on a wheelchair face additional challenges associated with suboptimal seatbelt fit, which can significantly increase the risk of seatbelt syndrome, a constellation of abdominal organ, spinal, and vascular injuries [3-5].
We present the case of a 90-year-old woman (height 140 cm), seated in a wheelchair and restrained only by a two-point lap belt. She sustained fatal blunt abdominal trauma in a low-speed collision. Aggressive interventions, including resuscitative endovascular balloon occlusion of the aorta (REBOA) and emergency thoracotomy (ET), were attempted but ultimately proved unsuccessful.
Specifically, this report addresses the following four key points: (1) REBOA and ET in geriatric blunt trauma, (2) the low survival rate of geriatric traumatic OHCA and the importance of accident prevention, (3) mechanisms and risk factors underlying seatbelt syndrome, and (4) unique seatbelt fit challenges for wheelchair users. By examining these points, we aim to highlight the critical need for improved restraint systems, refined treatment guidelines, and multifaceted prevention strategies to reduce mortality in this growing vulnerable population.
In particular, wheelchair users may be at a heightened risk of seatbelt syndrome due to improper belt positioning, which can lead to severe intra-abdominal or spinal injuries in even low-speed collisions.
Case presentation
Patient background
A 90-year-old woman (height 140 cm, weight 40 kg) with a past medical history of left femoral neck fracture, urinary tract infection, and hypertension customarily relied on a wheelchair for mobility.
Accident circumstances and immediate course
She was being transported in an adapted vehicle, with her wheelchair secured behind the driver's seat. A two-point lap belt was placed across her abdomen as the sole restraint mechanism. The accident occurred at 10:30 AM. While traveling at approximately 30 km/h, the vehicle rear-ended another car that was stopped at a traffic signal.
Initially, the patient was alert and reported feeling fine. However, she then rapidly deteriorated, becoming unresponsive and showing signs of shock, which prompted an emergency call to the local emergency medical services (EMS) at 10:42 AM.
Overview of the Traffic Accident
A kei car traveling at approximately 30-40 km/h collided with a standard passenger vehicle that was stopped at an intersection, waiting to make a right turn. The passenger vehicle sustained moderate rear-end damage, while the kei car incurred minor front-end damage. Neither vehicle's airbags deployed, and there was no airbag installed in the rear seat of the kei car. The driver of the rear-ended passenger vehicle suffered minor injuries, and the kei car's driver was unharmed.
EMS course
The patient's prehospital course is summarized in Table 1. The accident occurred at 10:30 AM, and EMS was notified at 10:42 AM, representing a 12-minute interval from crash to call. Upon EMS arrival (10:52), she was found to be in shock, with a blood pressure of 70/59 mmHg and Glasgow Coma Scale (GCS) score of 3 (E1, V1, M1). Although assisted ventilation was initiated promptly, the patient's condition deteriorated to pulseless electrical activity (PEA) at 11:07, necessitating cardiopulmonary resuscitation (CPR).
In-hospital course
Despite ongoing resuscitative efforts, her rhythm remained in PEA. On examination, there were no overt external hemorrhages or seatbelt marks. The Focused Assessment with Sonography for Trauma (FAST) revealed pericardial effusion and fluid around the spleen, suggesting liver and spleen injuries. The team proceeded with an ET, which showed clear pericardial fluid and effectively excluded cardiac tamponade. The patient's admission laboratory data are shown in Table 2. Notably, she had severe metabolic acidosis (pH 6.999), hyperkalemia (5.9 mEq/L), marked coagulopathy (activated partial thromboplastin time (APTT) >180 seconds, fibrinogen 34 mg/dL), and profound anemia (hemoglobin 6.1 g/dL). Intra-aortic balloon occlusion (IABO/REBOA) catheter was then inserted via the right femoral artery, and four units of packed red blood cells (PRBCs) were transfused. However, PEA persisted, and the patient was pronounced dead at 12:23 PM. Because the patient's hemodynamic status had deteriorated, performing a CT or contrast-enhanced CT was deemed difficult.
Postmortem CT
Postmortem CT findings revealed extensive bloody ascites in the abdomen and pelvis. Figure 1 shows findings suggestive of lacerations in the liver and spleen, while Figure 2 displays hemoperitoneum likely due to liver injury, and Figure 3 indicates bleeding within the pelvic cavity. These observations are consistent with blunt abdominal trauma.
CT image (abdomen)On the CT scan, intraperitoneal hemorrhage was observed around the liver and spleen, suggesting possible hepatic and splenic injuries. The red arrows indicate areas around the liver and spleen where what appears to be bloody ascites is present.
CT image (abdomen)CT scan showing hemoperitoneum with evidence of hepatic lacerations.
CT image (pelvic cavity)CT image demonstrating blood accumulation in the pelvic cavity, suggestive of intra-abdominal hemorrhage.
Postmortem examination findings
Although a formal autopsy was not performed, a limited external examination after death revealed a faint seatbelt mark in the upper abdomen that had not been apparent during the initial evaluation. This finding was consistent with blunt abdominal trauma attributed to seatbelt syndrome.
Discussion
REBOA and ET
REBOA and ET are aggressive interventions used in traumatic hemorrhagic shock and cardiac arrest.
Although REBOA can provide temporary hemorrhage control, its impact on overall survival remains uncertain. A national trauma registry study reported a mortality rate of 35.7% in the REBOA group compared to 18.9% in the non-REBOA group. However, this difference likely reflects the greater injury severity in the REBOA group rather than a direct effect of REBOA itself [6]. A recent systematic review found no significant difference in survival between REBOA and non-REBOA patients after adjusting for injury severity, highlighting the need for strict patient selection criteria [6].
Similarly, ET has limited efficacy, particularly in elderly patients with blunt trauma. The survival rate for ET in blunt trauma is approximately 1.4% [7]. Studies have reported near-zero survival in patients over 57 years of age, emphasizing the need for extreme caution when considering ET in this population.
Geriatric traumatic OHCA and accident prevention
Traumatic OHCA has a historically dismal prognosis, with a survival-to-discharge rate of approximately 2% [1]. However, recent studies indicate that survival can reach 5-8% in specific scenarios, such as in military settings or regions with highly advanced prehospital care systems [2]. This emphasizes the importance of rapid intervention and proper patient selection.
A nationwide Japanese study analyzing injured patients over a 10-year period reported a significant decrease in in-hospital mortality among elderly trauma patients [8]. In particular, mortality among severely injured elderly patients (Injury Severity Score (ISS) ≥16) declined from 26.1% to 14.5%, likely due to improvements in trauma care.
Given these challenges, primary and secondary prevention strategies are paramount. Seatbelt use is one of the most effective interventions, reducing fatality risk by up to 50% for front-seat occupants [5]. For rear-seat passengers, the risk reduction varies between 25% and 75%, depending on crash circumstances and proper belt use.
Seatbelt syndrome and risk factors
Seatbelts are essential for reducing injury severity, but improper fit can lead to "seatbelt syndrome," which involves injuries to the abdomen, spine, and vascular structures [4,9]. Multiple case reports have documented severe intra-abdominal injuries associated with seatbelt misuse. For example, Nigam and Nigam described a case in which a lap belt led to extensive hepatic and intestinal trauma, emphasizing the importance of improved restraint systems for high-risk populations [9]. Notably, two-point lap belts concentrate force on the abdominal organs and pose a particular danger to children and small adults under 140 cm [5]. Standard seatbelts are designed for individuals 140 cm or taller, and improper belt positioning in shorter occupants increases the risk of abdominal injuries associated with seatbelt syndrome.
In our case, the patient's short stature (140 cm) and wheelchair-dependent posture likely resulted in inadequate belt positioning, contributing to her fatal injuries. Research has highlighted that individuals with atypical body configurations, including wheelchair users, are disproportionately affected by seatbelt misalignment [10]. Improved restraint systems that can be adapted to diverse body types and mobility needs are crucial for reducing injury risk. Notably, the vehicle involved in this collision was manufactured in 2008, just before Japan's mandatory regulation requiring three-point seatbelts in rear seats took effect, leaving only a two-point lap belt available for this wheelchair-dependent occupant.
Additionally, the "submarine effect," wherein an occupant slides beneath the lap belt, has been documented in case studies and is another mechanism of severe injury [11,12]. These reports underscore the critical importance of proper restraint geometry and positioning.
Wheelchair users and seatbelt syndrome
Wheelchair users face disproportionately high risks in vehicle collisions due to inadequate seatbelt fit and limited restraint options [13]. Figure 4 provides an example of how a lap belt may be positioned in a small adapted vehicle for wheelchair users, highlighting potential fit issues. A Japanese regional study found that wheelchair users accounted for 7.8% of fatal vehicle-occupant crashes in Shiga Prefecture from 2020 to 2022, nearly doubling from previous years [14]. However, this statistic is not based on a nationwide dataset, and further research is needed to assess trends at the national level.
Example of a lap belt restraint for a wheelchair user in a kei carThe wheelchair's armrest interferes with the belt, preventing it from being properly secured at the navel. As shown in this photograph, depending on the wheelchair user's body type and seating position, the belt may not fit snugly and thus may be ineffective.Adapted from Kuwahara and Hitosugi [12], with permission from the authors and publishers.
Despite the clear risks, comprehensive data on injury mechanisms and outcomes for wheelchair users remain scarce. A recent study in Japan emphasized the need for a nationwide registry of wheelchair-occupant injuries and fatalities, which could facilitate better policy-making and more effective safety improvements [14].
Engineering analyses demonstrate that standard vehicle seatbelts are often inadequate for wheelchair users, as suboptimal positioning significantly increases the risk of severe injuries [15]. As shown in this photograph (Figure 4), depending on the wheelchair user's body type and seating position, the belt may not fit snugly and thus may be ineffective. Although the WHO has emphasized the importance of occupant restraints for all passengers, it has not issued specific guidelines for wheelchair restraint systems [10]. In the absence of such guidance, international safety standards, such as ISO 10542, recommend dedicated wheelchair tiedown and occupant restraint systems (WTORS) to improve safety for wheelchair users. Implementing WTORS could markedly reduce injury in this vulnerable population. Additionally, ensuring that transport personnel and caregivers are properly trained in seatbelt positioning is essential to minimizing preventable fatalities.
Conclusions
This case illustrates how the convergence of multiple risk factors, namely, advanced age, wheelchair dependence, and short stature, can lead to catastrophic injuries even during relatively low-speed collisions. While REBOA may offer transient hemodynamic stabilization, prolonged full occlusion carries a substantial ischemic burden. Similarly, ET in geriatric blunt trauma has shown very limited efficacy, emphasizing the need for stringent patient selection. The concept of "seatbelt syndrome" further underscores how improperly fitted restraints can concentrate force on the abdomen or spine, thereby heightening the risk of severe injury.
These findings highlight the importance of developing specialized restraint systems, such as three-point belts and pelvic harnesses, tailored to wheelchair users and smaller-framed elderly individuals, as well as the critical role of education and policy initiatives for caregivers and drivers.
It is important to acknowledge that this report is based on a single case and may not be broadly generalizable. Moreover, current data regarding the efficacy of REBOA and ET in older adults, particularly those traveling in wheelchairs, remain sparse, underscoring the need for larger-scale research. Nevertheless, given the growing population of elderly individuals who rely on wheelchairs, a comprehensive, patient-centered approach to preventing seatbelt syndrome and improving trauma care in this vulnerable group is becoming increasingly imperative.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Outcomes of prehospital traumatic cardiac arrest managed by helicopter emergency medical service personnel in Japan: a registry data analysis Int J Emerg Med Nagasawa H Omori K Muramatsu KI Takeuchi I Ohsaka H Ishikawa K Yanagawa Y 701620233782844310.1186/s 12245-023-00550-9PMC 10568871 · doi ↗ · pubmed ↗
- 2Epidemiology and outcome of adult out-of-hospital cardiac arrest of non-cardiac origin in Osaka: a population-based study BMJ Open Kitamura T Kiyohara K Sakai T 04201410.1136/bmjopen-2014-006462 PMC 427568425534213 · doi ↗ · pubmed ↗
- 3Estimated injury risk for specific injuries and body regions in frontal motor vehicle crashes Traffic Inj Prev Weaver AA Talton JW Barnard RT Schoell SL Swett KR Stitzel JD 01616201510.1080/15389588.2015.101266426027962 · doi ↗ · pubmed ↗
- 4The seat belt as a cause of injury Marq Law Rev Snyder RG 212228531970 https://scholarship.law.marquette.edu/mulr/vol 53/iss 2/5
- 5A radiographic and physical analysis of factors affecting seat belt position in sitting car seat Sci Rep Yamagata H Nishida N Izumiyama T 107321220223575071910.1038/s 41598-022-14607-x PMC 9232530 · doi ↗ · pubmed ↗
- 6Aortic balloon occlusion (REBOA) in pelvic ring injuries: preliminary results of the ABO Trauma Registry Updates Surg Coccolini F Ceresoli M Mc Greevy DT 5275367220203213066910.1007/s 13304-020-00735-4 · doi ↗ · pubmed ↗
- 7Emergency thoracotomies in traumatic cardiac arrests following blunt trauma - experiences from a German level I trauma center Eur J Trauma Emerg Surg Niemann M Graef F Hahn F 217721854920233727046710.1007/s 00068-023-02289-7PMC 10519862 · doi ↗ · pubmed ↗
- 8Ten-year in-hospital mortality trends among Japanese injured patients by age, injury severity, injury mechanism, and injury region: a nationwide observational study P Lo S One Toida C Muguruma T Gakumazawa M Shinohara M Abe T Takeuchi I 017202210.1371/journal.pone.0272573 PMC 939483435994453 · doi ↗ · pubmed ↗