Safety of Early Mobilization in Adult Neurocritical Patients: An Exploratory Review
Leonardo Arzayus-Patiño, José Luis Estela-Zape, Valeria Sanclemente-Cardoza

TL;DR
This review explores whether early mobilization is safe for adult patients with serious neurological conditions, finding it generally safe with few severe complications.
Contribution
The study provides a comprehensive scoping review on the safety of early mobilization in neurocritical care, highlighting protocol variability and the need for further research.
Findings
Early mobilization in neurocritical patients is generally safe with low severe adverse events.
Complications were manageable with protocol adjustments and continuous monitoring.
There was no significant increase in risks like vasospasm.
Abstract
Introduction: Early mobilization has shown significant benefits in the rehabilitation of critically ill patients, including improved muscle strength, prevention of physical deconditioning, and reduced hospital length of stay. However, its safety in neurocritical patients, such as those with strokes, traumatic brain injuries, and postsurgical brain surgeries, remains uncertain. This study aims to map and examine the available evidence on the safety of early mobilization in adult neurocritical patients. Methods: A scoping review was conducted following PRISMA-SCR guidelines and the Joanna Briggs Institute (JBI) methodology. The research question focused on the safety of early mobilization in neurocritical patients, considering adverse events, neurological changes, hemodynamic changes, and respiratory changes. A comprehensive search was performed in databases such as PubMed, BVS–LILACS,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
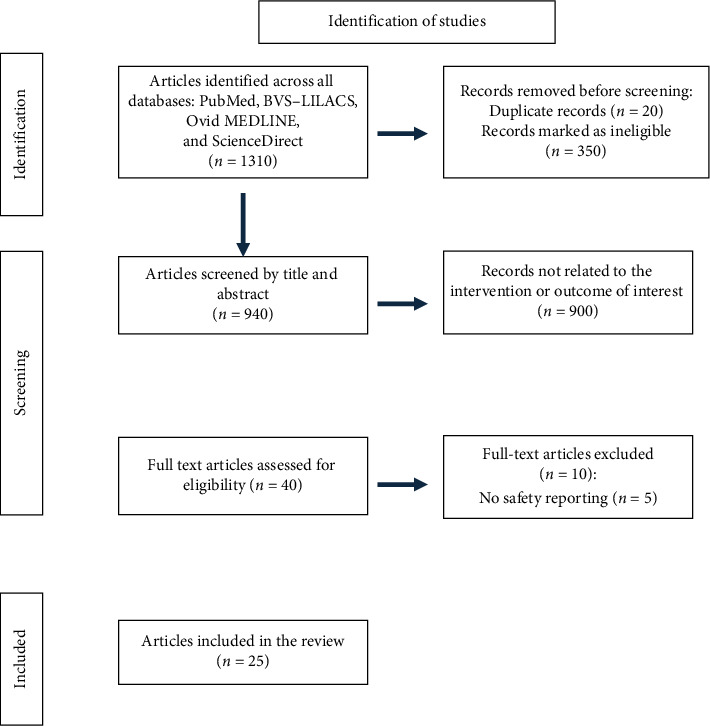 Figure 1
Figure 1- —Universidad Santiago de Cali
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStroke Rehabilitation and Recovery · Botulinum Toxin and Related Neurological Disorders · Cerebrospinal fluid and hydrocephalus
1. Introduction
Early mobilization (EM) has been identified as a potentially beneficial intervention in the field of rehabilitation, with positive effects observed in critically ill patients and those with prolonged hospital stays [1]. Among the potential benefits are improved muscle strength [2, 3], prevention of physical deconditioning [4], and an increase in days out of the hospital and intensive care unit [2, 5], which could contribute to better recovery and potentially reduce the economic burden on the healthcare system. Various clinical studies support the implementation of EM, and several clinical practice guidelines have emphasized its safety and effectiveness [6, 7, 8].
These clinical practice guidelines generally focus on hospitalized patients or those in intensive care units with cardiovascular, respiratory, and neurological conditions [6, 7]. While they acknowledge contraindications such as intracranial hypertension, acute intracerebral hemorrhage, and severe cerebral edema, they do not comprehensively address neurocritical patients. This group includes those with strokes (CVA), traumatic brain injuries, and postoperative brain surgeries, who require intensive care due to the complexity of their neurological injuries.
Neurocritical patients present challenges due to the severity of their conditions and the need for specialized management to prevent complications. In particular, those with cerebral edema, aneurysmal or nonaneurysmal hemorrhage, and risk of vasospasm, even if not experiencing intracranial hypertension at the time of intervention, can develop complications requiring continuous monitoring. The management of these patients involves strategies to control and reduce the risk of increased intracranial pressure (ICP), as a significant rise in ICP could exacerbate neurological damage and complicate the recovery process [9–13].
In this group of patients, three main categories are identified: those with hemorrhagic or ischemic stroke, patients with traumatic brain injury (TBI), and those who have undergone brain tumor resection. Patients with aneurysmal subarachnoid hemorrhage (SAH), in particular, present a high risk of complications such as rebleeding and vasospasm, especially between the second and third weeks [14–17]. EM in these cases has been a topic of debate. According to the most recent guideline [18], retrospective studies have shown that early rehabilitation after securing the aneurysm is feasible and safe, with no significant increase in adverse events. However, the guideline also emphasizes that no randomized clinical trials specifically evaluate the safety and effectiveness of this practice in this population.
While EM has been observed to be viable under controlled conditions, questions remain about its impact on specific complications such as vasospasm. Some studies [19] suggest that it could increase the risk, while others indicate that, when conducted appropriately and with adequate monitoring, it could help reduce this risk [14].
The current literature on EM in neurocritical patients is limited and does not provide conclusive guidance on the safety of this practice in this specific group, leading to uncertainty regarding its safety [4]. Although some studies have addressed this issue, the results have been varied and, in many cases, inconclusive [20, 21]. Additionally, mobilization protocols can differ significantly between institutions, further adding to the uncertainty about the safe implementation of these interventions.
Nevertheless, the potential benefits of EM in neurocritical patients warrant consideration. This practice could offer improvements in clinical and functional outcomes for this population, such as enhanced muscle strength, reduced physical deconditioning, and decreased hospital length of stay [20], which could translate into better quality of life and faster recovery for these patients [22–24].
Therefore, it is relevant to map and analyze the available evidence on the safety of EM in neurocritical patients. This leads to the following research question: What is the safety of EM in adult neurocritical patients?
2. Methods
This review followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-SCR) checklist [25] and was based on the Johanna Briggs Institute (JBI) methodology [26], initially conceived by Arksey and O'Malley [27].
2.1. Research Question
To guide the scoping review, the following question was formulated: What is the safety of EM in adult neurocritical patients? The question was designed based on population (divided into three groups), intervention, comparison, and outcomes:
- • P (Population): Adult neurocritical patients (patients with acute and subacute ischemic and hemorrhagic stroke, TBI, and postsurgical patients from any brain surgery)
- • I (Intervention): Studies applying EM
- • C (Comparison): Not applicable
- • O (Outcomes): Adverse events, neurological changes, hemodynamic changes, respiratory changes
2.2. Selection Criteria
To identify relevant studies, a bibliographic search was conducted based on the research question. Studies were included if they met the following inclusion criteria: primary research, expert recommendations, gray literature, guidelines or protocols, studies published without time restrictions, and publications available in Spanish, English, or Portuguese.
Studies exclusively evaluating passive interventions, such as functional electrical stimulation, and those lacking specific data on active or EM were excluded. These criteria ensured that the selected studies were relevant and directly aligned with the objectives of the analysis.
2.3. Sources of Information
Based on the research question, a comprehensive search was conducted in the following electronic databases: PubMed, BVS–LILACS, Ovid MEDLINE, and ScienceDirect. Keywords were determined using Medical Subject Headings (MeSH), Health Sciences Descriptors (DeCS), and natural language.
2.4. Search Strategy
Both controlled and uncontrolled language was used, defining terms (MeSH) and (DeCS) with keywords in English, Spanish, and Portuguese. These were used to design specific search equations for each database. Keywords were defined according to the PICO question, allowing the creation of search equations with the main descriptors and qualifiers structured in the Thesaurus. The equations are described in Table 1. The search was manually completed by reviewing the bibliographic references of the found articles using the following updated keywords.
2.5. DeCS–MESH
• Neurocritical Care/Critical Care/Intensive Care Units (ICUs)/Brain Injuries/Traumatic Brain Injury (TBI)/Diffuse Axonal Injury/Brain Hemorrhage/Intracranial Hemorrhages/Subarachnoid Hemorrhage/Stroke/Ischemic Stroke/Hemorrhagic Stroke/Intracranial Pressure/Intracranial Hypertension/Neurocritical/critical care/brain injuries/stroke/intracranial pressure• Rehabilitation/Neurologic Rehabilitation/Early Ambulation/Exercise Therapy/Early Rehabilitation/Physical Therapy Modalities/Mobilization/Early Mobilization/Early Rehabilitation/Physical Therapy/Postural Balance/Postural Control/Muscle Strength/Muscle Weakness• Patient Safety/Safety Management/Risk Assessment/Adverse Effects/Adverse Events/Complications/Iatrogenic Disease
For the initial search, concepts were standardized in the BVS portal and PubMed databases. Subsequently, an advanced bibliographic search was conducted in the databases listed in Table 1. After reviewing the included articles and consulting additional references, new relevant terms were identified. This allowed for a more specific second search, with the terms and formulas detailed in Table 1.
2.6. Selection of Sources of Evidence
The search was conducted by two researchers, with guidance from a university biomedical librarian. The process of identification, review, and eligibility was carried out in consensus among the researchers, with oversight and review by a third member.
2.7. Data Extraction
Identified studies were downloaded and uploaded into the RAYAN application. The titles and abstracts of the resulting studies were examined, and duplicates were subsequently removed. A critical reading was conducted, and a descriptive table was created with relevant data. One team member reviewed the relevance and adherence to the criteria, and a third researcher performed quality control by evaluating the excluded articles. There were no discrepancies among the researchers. Tables 2 and 3 describe the characteristics of the studies.
2.8. Characteristics of the Interventions
The reviewed interventions included EM techniques encompassing activities such as bed exercises, assisted transfers, progressive ambulation, and active positioning. The intensity of the interventions was analyzed, identifying the most common activities and specifying the prescription in terms of frequency and intensity to provide a more precise description of the characteristics of the interventions performed.
2.9. Quality Assessment of the Studies
To evaluate the methodological quality of the selected studies, the Joanna Briggs Institute (JBI) tool [21] was used, with specific checklists for each type of study. Each tool included a numbering system for the evaluated items, and a percentage was calculated based on the total number of items to determine the risk of bias. Table 4 summarizes the scores obtained.
2.10. Definition and Classification of Adverse Events
To comprehensively evaluate the safety of EM, an analysis of the adverse events reported in the selected studies was included. These events were classified based on their severity and the affected system (hemodynamic, respiratory, or neurological), providing a standardized framework for interpretation. The classification was defined as follows:
- • Minor Adverse Events: Temporary changes that do not require significant medical intervention and resolve spontaneously, such as mild hypotension, fatigue, or transient desaturation that does not require oxygen support.
- • Moderate Adverse Events: Changes that require healthcare personnel intervention but do not pose an immediate life-threatening risk, such as sustained desaturation requiring oxygen support, controllable hypertension, or hypotension.
- • Severe Adverse Events: Significant changes that pose a life-threatening risk, require immediate intervention, or result in permanent sequelae, such as severe vasospasm, significant intracranial hypertension, severe arrhythmias, or cardiopulmonary arrest.
Table 5 provides detailed definitions and classifications used.
2.11. Presentation of Results
The results are presented in descriptive tables highlighting relevant aspects of each study, such as study type, objective, population, type of mobilization, adverse events related to mobilization, and safety. Tables illustrating the search strategy with the equations used (Table 1) and the final number of included studies are presented, along with a flowchart describing the search process and the final number of studies (Figure 1).
3. Results
A total of 1310 articles were identified in the databases. After preselection and evaluation by title and abstract, inclusion and exclusion criteria were applied, and nonrelevant articles were excluded. Following this review, 40 articles were selected for full-text reading. Finally, 25 articles were included in this review (Figure 1).
3.1. Study Characteristics
Among the identified articles, there were twelve randomized controlled trials, six prospective observational studies, three retrospective studies, two pre- and postimplementation intervention studies, and three prospective intervention studies. Of these studies, seven were conducted in the United States [29–33, 28, 47], three in Norway [14, 34, 35], one in Australia, New Zealand, Malaysia, Singapore, and the United Kingdom (The AVERT Trial Collaboration Group, 2015) [36], two in Taiwan [46, 52], one in Japan [37], one in Switzerland [57], two in Italy [39, 49], one in France [51], one in Denmark [55], one in China [53], and one in India [56].
Table 3 details the main characteristics of the studies that included stroke patients. This table was divided into two population groups: patients whose severity required admission to intensive care units, and those admitted to specialized stroke care units, considered noncritical in some settings. Table 4 presents the characteristics of studies that included patients with TBI and postsurgical brain surgery patients.
3.2. Intervention Characteristics
Regarding the interventions performed, seven studies applied EM in stroke patients in specialized care units [34, 36, 51,52, 54, 56, 57], while eight studies focused on stroke patients admitted to intensive care units [28, 29, 35, 30, 31, 37, 53]. Four studies were conducted on patients with moderate-to-severe TBI [32, 46, 39, 49]. Additionally, one study evaluated an intervention protocol in neurocritical patients with various conditions [46], and another investigated a progressive mobility program in the neurosurgical ICU [38]. Other studies included EM in patients with chronic subdural hematoma [40], gradual mobilization in severe brain injuries [49], and the neurological ICU [35]. Finally, one study evaluated light exercise to reduce cerebral vasospasm [31].
3.3. EM
Interventions in patients with stroke (CVA), TBI, and brain surgery exhibit notable heterogeneity in terms of type, frequency, and intensity. The interventions ranged from passive mobilization techniques to progressive active mobilization, with significant differences in initiation times and session durations, depending on the clinical condition of the participants.
In CVA patients, EM was typically initiated within 24–72 h after the event or hospital admission. Common activities included getting out of bed, sitting, standing, and walking. Studies such as the AVERT trial [36] and those conducted by Yen et al. 2020 [52] reported variable intervention frequencies, ranging from multiple daily sessions with durations of 5–30 min. However, these interventions lacked uniform prescriptions.
For TBI patients and those in postsurgical conditions, mobilization strategies included techniques such as assisted passive movements, standing exercises, and progressive walking. The author [46] implemented progressive mobilization within a range of 24–72 h after admission, adjusting activities based on each patient's tolerance. Similarly, Pinto et al. [40] applied EM out of bed following surgery, emphasizing the need to tailor interventions individually. Nonetheless, the duration and intensity of sessions varied considerably across studies.
3.4. Safety and Adverse Events in Stroke Patients
3.4.1. Studies in Specialized Stroke Units
Studies conducted in specialized units for the management of stroke evaluated different subgroups of patients, including those with SAH, ischemic stroke, and a combination of both types of stroke.
In the SAH patient group, a specific study [53] reported no adverse events in the intervention group. For patients with ischemic stroke [52, 54, 57], EM was well-tolerated, with no major complications attributed to the intervention [51]. Although minor adverse events, such as falls, were observed, there were no significant differences between groups [54]. Additionally, EM reduced severe complications without affecting cerebral blood flow or neurological outcomes [57].
In studies including patients with both ischemic and hemorrhagic strokes, the AVERT Trial Collaboration (2015) [36] found no significant differences in nonfatal serious adverse events between the EM and usual care groups. Conversely, Sundseth and Thommessen, and Rønning [34] reported similar complications in both groups, although the late mobilization group experienced more events related to immobility. However, they concluded that very EM (VEM) might not be safe, showing a trend toward worse outcomes and higher mortality. EM was considered safe, resulting in better functional status without major complications [56].
3.5. Intensive Care Unit
In the group of stroke patients admitted to intensive care units, no adverse events or complications were attributed to EM [29, 30, 38, 54]. Olkowski et al. reported events such as a decrease in mean arterial pressure and an increase in heart rate over 120 beats per minute in 5.9% of the sessions. Karic et al. (2015) [35] documented headaches, fatigue, hypertension, tachycardia, and hydrocephalus, all appropriately managed and not directly attributed to early rehabilitation.
Vasospasm was a major concern in the setting of EM and SAH in several studies. Karic et al. [14] reported vasospasm in 21.6% of patients, which was managed appropriately by allowing mobilization to continue in mild cases and pausing in severe cases. Riordan et al. [31] found that light exercise, including EM, significantly reduced vasospasm frequency and severity, as well as markers of inflammation and oxidative stress. Young et al. [29] documented episodes of hypertension, elevated ICP, and symptomatic vasospasm leading to session interruptions, but no serious adverse events were attributed to EM.
3.6. Safety and Adverse Events in TBI and Surgery Patients
In the evaluated studies, EM in patients with TBI and neurosurgery was found to be safe, with manageable adverse events. Pinto et al. [40] and Elkbuli et al. [32] reported significant improvements in mobility and reductions in hospital and ICU stays, without serious adverse events. Rocca et al. [38] observed episodes of hypotension in the standard mobilization group, but mobilization with Erigo was safe and well-tolerated. Yen et al. [46] and Frazzitta et al. [49] also highlighted improvements in functional and neurological outcomes, with no serious adverse events. Bartolo et al. [39] showed significant improvements in patients with severe acquired brain injury, and Bahouth et al. [47] documented minor events such as hypotension, desaturation, and arrhythmias, all properly managed. Jarvis et al. [33] reduced hospital stays, with manageable episodes of hypotension and desaturation.
Riberholt et al. [55] confirmed that early orthostatic exercise in patients with severe TBI was feasible and safe, with a high completion rate of sessions and only minor events, such as orthostatic hypotension and fever, without serious complications.
3.7. Risk-of-Bias Assessment (Methodological Quality)
The methodological quality was assessed using the JBI tool [26]. The studies generally showed a low risk of bias with moderate-to-high methodological quality. Table 3 shows the evaluation of the articles.
4. Discussion
The objective of this review was to describe and present evidence on the safety of EM in neurocritical patients, finding that the practice results in a low level of adverse events. Most studies report that EM is safe and feasible. The reviewed studies indicated a low incidence of serious adverse events, which were mostly manageable through adjustments in mobilization protocols and continuous monitoring. Additionally, improvements in functional outcomes and a reduction in hospital stay duration were observed, without a significant increase in complications.
The results suggest that EM is safe in stroke patients (CVA) [14, 29, 30, 31, 36, 37, 51, 52, 54, 57], trauma patients [32, 33, 38], and postsurgical patients [40]. Kumar, Romero, and Dharaneeswaran [41] highlighted that EM in critical patients helps reduce ICU stay duration, improve clinical and functional outcomes, and alleviate the economic burden on the healthcare system. Only one study concluded that the VEM group showed a trend toward worse outcomes and higher mortality [34].
The safety of EM in patients with SAH varies depending on the type of bleeding and the presence of aneurysms. In patients with nonaneurysmal SAH, there is a high risk of rebleeding between 48 and 72 h, as reported by Minhas et al. [42]. This risk is considerably high due to the fragility of the vessels and the hemodynamic instability that characterizes these patients. Ma, Wang, and Liu [43] suggest that EM in these cases should be evaluated cautiously due to the significant risk of rebleeding.
In aneurysmal SAH, the reviewed studies do not include patients whose aneurysm has not been secured due to the high risk of rebleeding. This suggests that EM in these cases has not been extensively explored, as the risk may outweigh the potential benefits and increase morbidity and mortality. Dukatz et al. [44] emphasize the need for a cautious approach, recommending initiating EM only after securing the aneurysm.
In contrast, once the aneurysm is secured, EM in patients with aneurysmal SAH is considered feasible and safe. Karic et al. [14] reported the absence of severe adverse effects, although pauses were made due to headaches, fatigue, hypertension, tachycardia, and hydrocephalus, which were managed appropriately. Young et al. [29] demonstrated that EM is safe in patients with SAH and external ventricular drainage, and it was associated with better functionality at discharge. Olkowski et al. [28] concluded that EM is viable, with a low rate of adverse events and no increase in 30-day mortality. Jarvis et al. [33] evidenced that, with adequate monitoring, EM improved mobility and significantly reduced hospital stay. However, it is crucial to monitor blood pressure and ICP, as they can be altered by physical activity and increase the risk of rebleeding.
The safety of EM in patients with SAH has been widely evaluated. Although vasospasm is a common complication in up to 70% of patients, usually occurring between the third and tenth days posthemorrhage [43], studies have not shown that EM increases this risk. Karic et al. [14, 17] reported that EM, initiated from the first day after securing the aneurysm, did not significantly increase adverse events related to vasospasm. Young et al. [29] confirmed that EM in patients with SAH and external ventricular drainage did not increase the incidence of vasospasm, and Riordan et al. [31] observed that light exercise was associated with a reduction in the frequency and severity of vasospasm.
In patients with severe vasospasm, EM should be performed with caution. Karic et al. [14, 35] emphasized that in cases of severe vasospasm, mobilization had to be interrupted until the vasospasm resolved to avoid additional complications. Young et al. [29] found that some mobilization sessions in patients with symptomatic vasospasm also had to be suspended. The evidence suggests that the decision to mobilize should be based on continuous evaluation of the patient's neurological and hemodynamic status, adapting or suspending mobilization in the presence of severe vasospasm to ensure patient safety. This aligns with Hodgson et al. [45], who support that out-of-bed mobilization is contraindicated in the presence of acute neurological changes or when vasopressors are required.
Regarding EM in patients with TBI, it was found to be safe and beneficial with adequate monitoring. Yen et al. [46] reported improvements in mobility without significant adverse events. Elkbuli et al. [32] demonstrated a significant reduction in hospital stay and lower complication rates, without serious adverse events. Similarly, Yen et al. [46] observed improvements in functional mobility without additional harm. However, Rocca et al. [38] indicated that EM is well-tolerated and safe with monitoring devices, although caution should be taken in patients with orthostatic hypotension. Bahouth et al. [47] support the safety of EM in neurocritical patients, including TBI, and emphasize the need for continuous monitoring to manage minor adverse events.
Despite the reported safety, associated risks such as hypotension and increases in ICP should be considered. A decrease in cerebral perfusion pressure can damage recovering ischemic areas. Godoy [48] highlights that to preserve neuronal survival after severe TBI, it is crucial to maintain adequate cerebral perfusion pressure. Although EM can cause variations in this pressure, close monitoring is essential to ensure the patient's hemodynamic stability.
Variations in the type, frequency, and intensity of EM interventions can significantly impact outcomes in neurocritical patients. The observed heterogeneity in the timing of initiation, activities performed, and session duration complicates the generalization of findings across different studies. For instance, the AVERT trial [37] documented an increase in minor adverse events in groups subjected to very early and high-intensity mobilization, suggesting that excessive intensity might be associated with greater risks. Conversely, studies by Karic et al. [14] and Young et al. [29] found that less intensive interventions tailored to the specific conditions of patients were better tolerated and not associated with a significant increase in complications.
The comparison of these variations highlights the importance of designing personalized protocols that take into account the specific clinical conditions of patients. Moreover, studies such as those by Riordan et al. [31] and Olkowski et al. [28] emphasize that a gradual progression, based on patient tolerance, could reduce the incidence of adverse events while optimizing functional benefits. These differences underscore the need to develop standardized protocols that include key parameters such as the timing of initiation, intensity, and duration, enabling more consistent comparisons across studies and yielding more robust and applicable conclusions regarding the safety and efficacy of EM in neurocritical populations.
The safety of EM can be significantly enhanced through the implementation of standardized protocols and systematic tools for risk assessment. The findings of this review highlight that continuous monitoring and the personalization of interventions are essential to minimize adverse events such as hypotension, desaturation, or increased ICP.
The use of safety detection algorithms, such as standardized evaluation scales or presession checklists [45], represents a key strategy to identify specific risk factors before initiating EM. These tools not only allow for precise risk identification but also facilitate risk stratification by classifying patients according to their likelihood of experiencing adverse events. This is particularly crucial in vulnerable populations, such as neurocritical patients, who require stricter monitoring and highly personalized care.
A comprehensive initial assessment should include an integral analysis of the patient's neurological [58], hemodynamic [59], and respiratory status [60]. This involves continuous monitoring of key parameters such as blood pressure, ICP, heart rate, oxygen saturation, and cerebral perfusion pressure levels. The detection of signs of instability, such as altered consciousness, fluctuations in blood pressure, or oxygen saturation, may indicate the need to postpone or adjust mobilization. Additionally, it is essential to identify temporary contraindications before the intervention, such as severe vasospasm, hemodynamic instability [61], high oxygen support requirements [62], fever, or active infections. It is also crucial to assess the use of invasive medical devices, such as catheters, drains, or ICP monitoring systems, to ensure their stability and functionality during EM.
These evaluations must be complemented by the implementation of clear criteria for the progression or suspension of mobilization, based on the patient's tolerance. Any deterioration in monitored parameters or the appearance of symptoms such as pain, dyspnea, or extreme fatigue should signal the need to halt or modify the intervention. This approach could optimize the safety of EM.
The progression of activities should be based on a gradual evaluation of the patient's tolerance, beginning with low-energy movements in bed, followed by activities such as sitting on the edge of the bed, assisted transfers, and, finally, supervised standing and walking with or without assistance. Furthermore, progression must be personalized and adapted to the patient's clinical response, with immediate interruptions or modifications in cases of decompensation.
EM in neurocritical patients requires a multidisciplinary approach [63] to ensure both its safety and efficacy. Physical therapists lead the implementation of progressive physical activities, tailoring them to each patient's clinical conditions. Physicians oversee neurological and hemodynamic stability, adjusting critical parameters to minimize risks. Nurses continuously monitor patients, manage barriers such as catheters and intravenous fluids, and provide support during sessions. Additionally, disciplines such as occupational therapy and nutrition contribute to the process by promoting functionality and optimizing muscle and energy recovery.
The integration of standardized bundles, such as the ABCDEF model in critical care, which incorporates EM and fosters multidisciplinary collaboration, has proven effective in optimizing implementation and reducing secondary complications [64, 65, 66]. Furthermore, adequate collaboration and communication between rehabilitation and medical teams have been suggested to significantly improve outcomes, increase mobilization in this patient population [67], and reduce hospital stays in neurological patients [68]. Interdisciplinary collaboration in the intensive care unit is essential, as constant and efficient communication between the different disciplines ensures that safety measures and medical interventions are maintained during the implementation of EM [69], thereby reducing potential risks.
The methodological quality of the studies was evaluated using the JBI tools. The randomized controlled trials [36, 38, 40, 49, 50, 51–56] demonstrated high methodological quality with scores ranging from 81% to 90%. Other studies presented moderate methodological quality [28, 29, 31, 34, 35, 38, 39, 46, 47, 57] with scores ranging from 70% to 82%. Retrospective and quality improvement studies, such as those by Elkbuli et al. [32] and Jarvis et al. [33], were considered of high quality with a score of 100%. These results demonstrate the validity of this review's findings, as the included studies meet good quality standards in their research.
The review is notable for its methodological strengths, including the rigor in applying standardized protocols and evaluating the quality of the studies. However, several limitations were identified in the present study, particularly regarding the safety of EM. Many studies did not primarily focus on providing detailed documentation of adverse events related to this intervention, which made it difficult to gather accurate and consistent data. Additionally, a considerable number of included studies were retrospective or nonrandomized in design, which can introduce bias and limit the generalizability of the findings. Heterogeneity in EM protocols was also observed, with differences in prescriptions across studies, complicating direct comparisons of results and the development of standardized recommendations. Furthermore, the small sample sizes in some studies provided low statistical power and limited the ability to detect significant differences, underscoring the need for randomized clinical trials to rigorously evaluate this intervention.
5. Conclusion
EM in neurocritical patients has been shown to be potentially safe under specific conditions, without a significant increase in severe complications when properly monitored. However, the available evidence is limited by the heterogeneity of protocols and study designs, emphasizing the need for further research. The importance of tailoring mobilization protocols to each patient and ensuring continuous monitoring is highlighted. Additional studies with larger sample sizes are needed to fully understand the associated risks and optimize mobilization strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yang X. Zhang T. Cao L. Ye L. Song W. Early Mobilization for Critically Ill Patients Respiratory Care 202368678179510.4187/respcare.1048137041029 PMC 10209006 · doi ↗ · pubmed ↗
- 2Tipping C. J. Harrold M. Holland A. Romero L. Nisbet T. Hodgson C. L. The Effects of Active Mobilisation and Rehabilitation in ICU on Mortality and Function: A Systematic Review Intensive Care Medicine 201743217118310.1007/s 00134-016-4612-02-s 2.0-8499578469027864615 · doi ↗ · pubmed ↗
- 3Kayambu G. Boots R. Paratz J. Early Physical Rehabilitation in Intensive Care Patients With Sepsis Syndromes: A Pilot Randomised Controlled Trial Intensive Care Medicine 201541586587410.1007/s 00134-015-3763-82-s 2.0-8493776325225851383 · doi ↗ · pubmed ↗
- 4Schweickert W. D. Pohlman M. C. Pohlman A. S. Early Physical and Occupational Therapy in Mechanically Ventilated, Critically Ill Patients: A Randomised Controlled Trial The Lancet 200937396781874188210.1016/s 0140-6736(09)60658-92-s 2.0-65849187703 PMC 990665519446324 · doi ↗ · pubmed ↗
- 5Dong Z. H. Yu B. X. Sun Y. B. Fang W. Li L. Effects of Early Rehabilitation Therapy on Patients With Mechanical Ventilation World Journal of Emergency Medicine 201451485210.5847/wjem.j.issn.1920-8642.2014.01.00825215147 PMC 4129870 · doi ↗ · pubmed ↗
- 6Lang J. K. Paykel M. S. Haines K. J. Hodgson C. L. Clinical Practice Guidelines for Early Mobilization in the ICU: A Systematic Review Critical Care Medicine 20204811 e 1121 e 112810.1097/CCM.000000000000457432947470 · doi ↗ · pubmed ↗
- 7Rethnam V. Hayward K. S. Bernhardt J. Churilov L. Early Mobilization After Stroke: Do Clinical Practice Guidelines Support Clinicians’ Decision-Making? Frontiers in Neurology 202112 p. 60652510.3389/fneur.2021.606525 PMC 790192333633667 · doi ↗ · pubmed ↗
- 8Cartotto R. Johnson L. Rood J. M. Clinical Practice Guideline: Early Mobilization and Rehabilitation of Critically Ill Burn Patients Journal of Burn Care and Research 202344111510.1093/jbcr/irac 00835639543 · doi ↗ · pubmed ↗