Beating heart superior caval vein replacement for giant venous aneurysm: a case report
Kira Osipenko, Daniel Zimpfer, Maria Anwar, Stephane Mahr, Paul Werner

TL;DR
A 68-year-old man with a large superior vena cava aneurysm underwent successful surgical replacement with a graft, showing no complications after three months.
Contribution
This is the first documented use of a 20 mm ePTFE graft for adult SVC aneurysm replacement.
Findings
The patient recovered uneventfully after surgery with no complications.
Postoperative imaging confirmed graft patency and no signs of recurrence.
The technique ensures complete excision of affected tissue, reducing recurrence risk.
Abstract
Superior vena cava (SVC) aneurysms are rare vascular anomalies, with <80 cases reported worldwide. Large aneurysms carry a risk of rupture and thrombosis, eventually necessitating surgical intervention. We present the case of a 68-year-old male with a progressively enlarging SVC aneurysm and a history of paroxysmal atrial fibrillation. The patient underwent successful caval resection and replacement with a 20 mm expanded polytetrafluoroethylene (ePTFE) graft, accompanied by left atrial appendage exclusion and pulmonary vein isolation. The recovery from surgery was uneventful, and postoperative imaging confirmed excellent graft patency with no signs of thrombosis or recurrence at the three-month follow-up. This case highlights the successful management of a large SVC aneurysm through complete resection and prosthetic replacement with a 20 mm ePTFE graft, with the first documented use…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
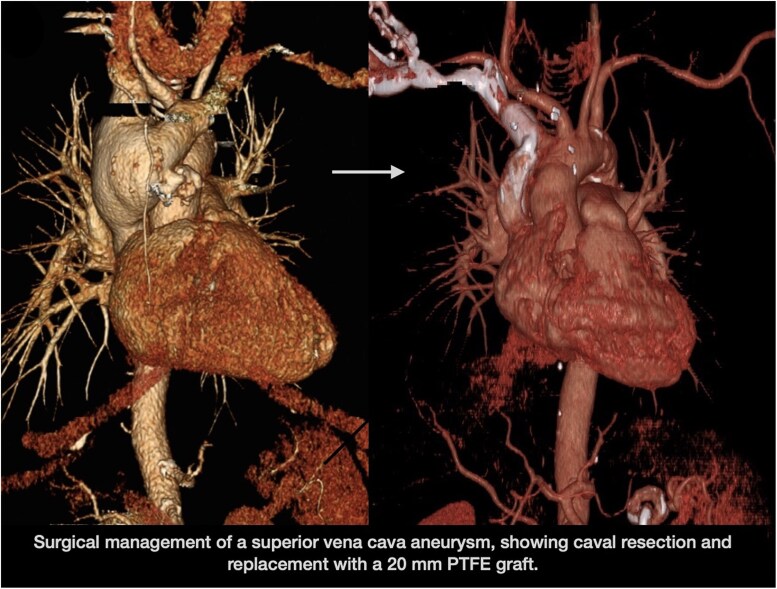 Figure 1
Figure 1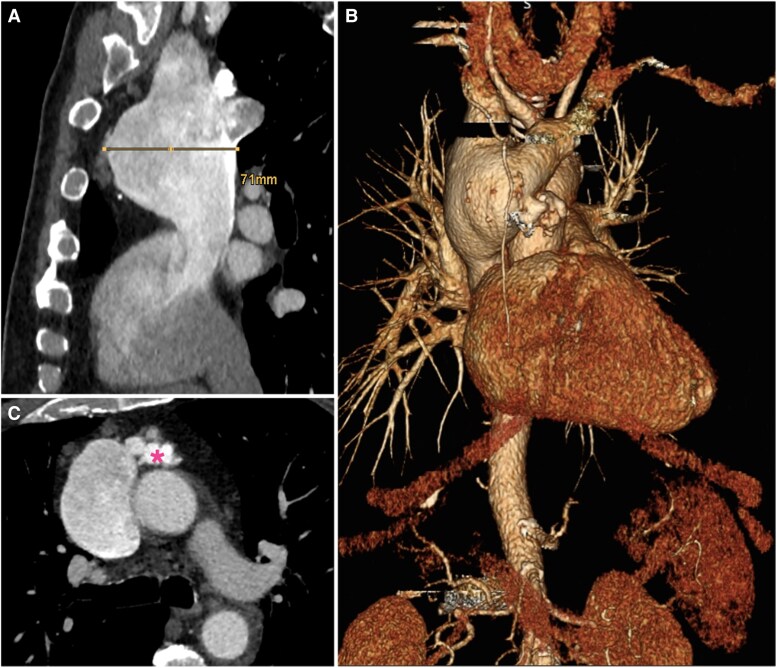 Figure 1
Figure 1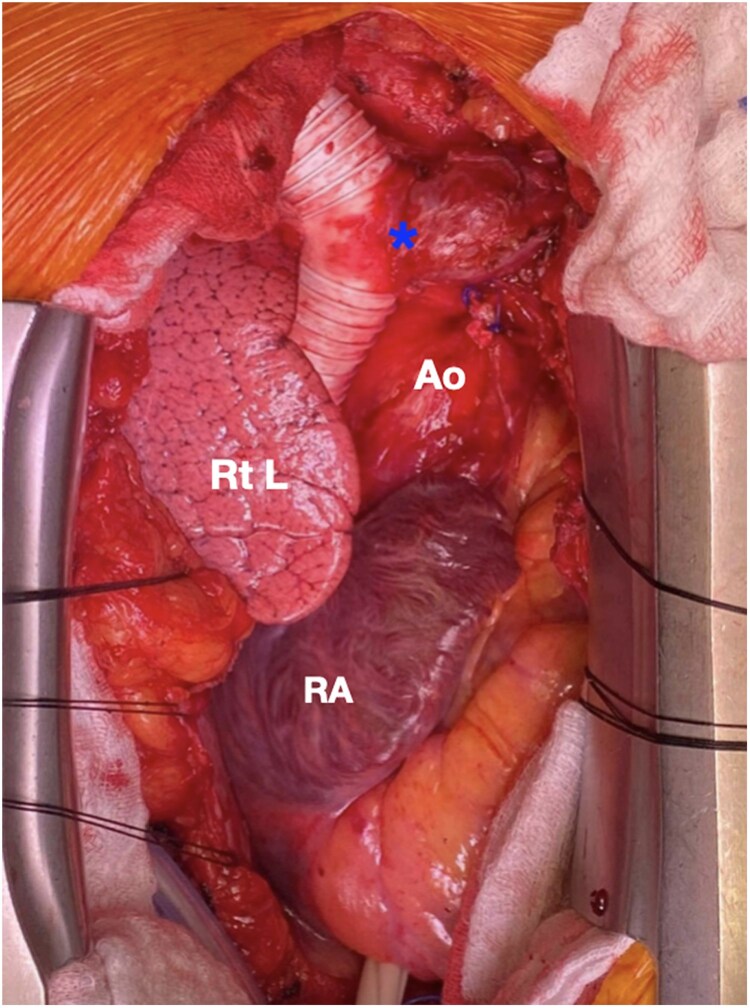 Figure 2
Figure 2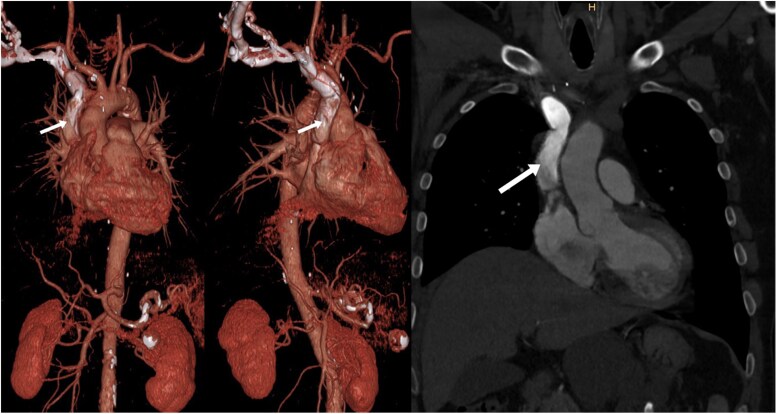 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Vascular anomalies and interventions · Cardiac Arrhythmias and Treatments
Introduction
Superior vena cava aneurysms (SVCAs) are a rare clinical diagnosis with <80 cases described worldwide.^1^ While some propose a conservative strategy, surgical treatment has been predominantly performed, especially in cases of aneurysm growth, because large aneurysms present a risk of rupture and thrombosis, eventually requiring surgical intervention.^2^ We herein describe to our knowledge the first case of caval replacement with an ePTFE prosthesis as a possible surgical strategy for SVCAs.
Summary figure
**
Case presentation
A 68-year-old asymptomatic male patient was incidentally diagnosed with a fusiform SVCA on computed tomographic angiography (CTA) performed for further evaluation of a suspicious mass seen on a chest X-ray. He was followed up for two years at our outpatient clinic, and a disease progression was notable. At last follow-up, the venous aneurysm measured at 7 cm involving the innominate and right subclavian veins (Figure 1). Due to the presence of atypical venous malformations and to rule out a possible malignancy, a positron emission tomography-magnetic resonance imaging was performed, showing no suspicious fluorodeoxyglucose uptake. The patient also suffered from paroxysmal atrial fibrillation and had a history of two ablation procedures for atrioventricular nodal re-entrant tachycardia. Coronary angiography demonstrated no significant coronary artery disease, and transthoracic echocardiography revealed good biventricular function and unremarkable valve status. The physical examination, including heart auscultation, showed no abnormalities.
Preoperative CTA illustrating the aneurysm of the superior vena cava (SVC). (A) 7 cm maximum diameter in anterior–posterior axis. (B) 3D reconstruction of the SVC aneurysm. (C) Atypical venous malformations (asterisk) below the brachiocephalic vein origin.
Surgical correction of the SVCA with concomitant atrial fibrillation ablation and left atrial appendage exclusion was planned.
Perioperative course
Following median sternotomy, dissection of the innominate vein, the right subclavian vein, the right jugular vein, and the mostly extra-pericardial and extra-pleural located SVCA was performed with care to the surrounding structures such as the right phrenic and recurrent nerve.
Following full heparinization, arterial cannulation was performed in the ascending aorta and venous cannulation directly in the inferior vena cava with a 32 French angled tip and percutaneously in the right jugular vein via a 17 French heparin-coated cannula in Seldinger technique. After initiation of cardiopulmonary bypass (CPB), radiofrequency ablation of the pulmonary veins was performed and a 40 mm AtriClip (Atricure, Mason, OH, USA) was applied to the left atrial appendage. An additional venous cannula (20 mm metal tip) was introduced in the innominate vein, and total CPB was initiated.
The venous aneurysm was completely resected up to the origin of the brachiocephalic vein, while the azygos vein was ligated externally. The aneurysm was sent for frozen section procedure, where no malignancy was found, thus the phrenic nerve could be spared. The distal anastomosis to the right subclavian vein was performed with a 20 mm PTFE graft and 5-0 polypropylene in running technique. The brachiocephalic vein was anastomosed end-to-side with that 20 mm graft, and the proximal anastomosis of the graft was then sewn to the cava stump at the right atrium (Figure 2). Uneventful cardiopulmonary bypass weaning and subsequent chest closure concluded the procedure.
Intraoperative image demonstrating the operative result after 20 mm PTEF graft replacement of the superior vena cava, with the asterisk indicating the end-to-side anastomosis of the brachiocephalic vein. Ao, ascending aorta; Rt L, right lung; RA, right atrium.
Following extubation and catecholamine weaning, the patient was transferred to the normal ward on the second postoperative day. A left-sided vocal cord motility disorder was noted before discharge, which fully resolved after one month of treatment with medications containing vitamins B1 and B6.
At three-month follow-up, the patient showed excellent recovery, and CTA demonstrated no pathological findings with good contrast filling of the PTFE graft without any signs of thrombosis (Figure 3). Due to recurrent episodes of atrial fibrillation, the patient was placed on anticoagulation with rivaroxaban.
Postoperative CTA at 3-month follow-up demonstrated a satisfactory surgical result with homogenous contrast filling of the PTFE graft without any signs of thrombosis (white arrow).
Discussion
Superior vena cava aneurysms are extremely rare vascular abnormalities, generally classified into two subtypes: fusiform and saccular.
Fusiform aneurysms are the more frequently encountered variant and are typically identified incidentally, as most patients remain asymptomatic.^3^ These aneurysms are generally associated with a benign clinical course and are managed conservatively, with anticoagulation therapy and regular monitoring to prevent complications.^1,4^
Saccular aneurysms, on the other hand, are considerably less common. They typically develop as a consequence of post-interventional or post-inflammatory events and are associated with a significantly elevated risk of serious complications, such as rupture, thrombosis, and venous obstruction. Due to these risks, surgical resection is generally the treatment of choice, particularly when there are concerns about the aneurysm’s morphology, its increasing size beyond 40 mm, or the presence of thrombus.^1,5^
Various surgical approaches for the treatment of SVCAs have been described in the literature. In early reports from the 1950s, one case described treating an aneurysm by applying polythene cellophane to the affected area.^6^ Nowadays, the most common approach for managing SVCAs is caval reconstruction using a bovine pericardial patch. Although easily reproducible, this technique presents with a shortcoming, that not all aneurysmatic tissue is resected. In contrast, when performing caval resection and replacement as described in this case, complete resection of affected tissue limits the chance of recurrence. An expanded polytetrafluoroethylene graft was the conduit of choice as it demonstrates good long-term durability with lower dilatation rates, particularly in comparison to polyester grafts.^7^ Due to their longevity, ePTFE grafts are commonly used as venous conduits in paediatric cardiac surgery, namely the extracardiac Fontan procedure, which demonstrates favourable long-term outcomes with a 32-year survival probability of 84% and a graft failure risk of 12%.^8^ However, long-term studies also mentioned potential risks, such as stenosis and thrombosis and the necessity of anticoagulation.^9^ Currently, no data are available on the long-term outcomes of ePTFE grafts for superior vena cava replacement, particularly regarding the risks of thrombosis or stenosis.
For high-risk patients where surgery is not feasible, endovascular techniques may be employed. One such approach is the first reported use of balloon-protected transcatheter thrombin injection, applying latex balloon protection to avoid SVC thrombosis.^10^ This technique could be a valuable alternative for treating large and growing saccular central vein aneurysms in this patient group. The application in fusiform aneurysms, however, might be of limited value. A recently described true transcatheter alternative includes coil occlusion of the vein, placement of an uncovered stent in the SVC, and coil closure of the aneurysm sac’s neck through the stent framework.^5^
Conclusion
Superior vena cava aneurysms present a rare clinical entity, with surgical (and endovascular) approaches available depending on the patient’s risk profile. While conservative management may be applied in absence of aneurysmal growth, our case highlights the necessity of timely surgical intervention. The use of a 20 mm PTFE graft for reconstruction demonstrates mirrors established paediatric cardiovascular procedures and provides a novel solution for adult SVCAs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brilla MAR, Kausen KD, Ollé A, Bautista-Hernandez V. Surgical resection of superior vena cava saccular aneurysm. Ann Thorac Surg Short Rep 2024;2:559–562.39790412 10.1016/j.atssr.2024.04.005PMC 11708133 · doi ↗ · pubmed ↗
- 2Patel A, Cobb R, Rivera V, Simpson S. Untreated superior vena cava aneurysm: radiological significance and review of the literature. Case Rep Radiol 2016;2016:6960757.28050303 10.1155/2016/6960757 PMC 5165137 · doi ↗ · pubmed ↗
- 3Sharma R, Ravi M, Unni TG. Primary fusiform superior vena cava aneurysm. Cardiol Res 2017;8:176–178.28868105 10.14740/cr 570w PMC 5574292 · doi ↗ · pubmed ↗
- 4Kapoor H, Gulati V, Pawley B, Lee JT. Massive fusiform superior vena cava aneurysm in a 47-year-old complicated by pulmonary embolism: a case report and review of literature. Clin Imaging 2022;81:43–45.34598003 10.1016/j.clinimag.2021.08.008 · doi ↗ · pubmed ↗
- 5Morales MM, Anacleto A, Leal JCF, Greque VG, Souza AS, Wolosker N. Saccular superior vena cava aneurysm: case report and comprehensive review. Ann Vasc Surg 2021;72:666.e 23–666.e 32.10.1016/j.avsg.2020.10.03333333194 · doi ↗ · pubmed ↗
- 6Abbott OA . Congenital aneurysm of superior vena cava. Ann Surg 1950;131:259–263.15402799 10.1097/00000658-195002000-00013 PMC 1616389 · doi ↗ · pubmed ↗
- 7Stollwerck PL, Kozlowski B, Sandmann W, Grabitz K, Pfeiffer T. Long-term dilatation of polyester and expanded polytetrafluoroethylene tube grafts after open repair of infrarenal abdominal aortic aneurysms. J Vasc Surg 2011;53:1506–1513.21536404 10.1016/j.jvs.2011.02.028 · doi ↗ · pubmed ↗
- 8Giannico S, Trezzi M, Cantarutti N, Cafiero G, Ravà L, Adorisio R, et al Late outcome of extracardiac Fontan patients: 32 years of follow-up. Eur J Cardiothorac Surg 2022;62:ezac 301.35543463 10.1093/ejcts/ezac 301 · doi ↗ · pubmed ↗