A case report of cardiogenic shock due to tachycardic atrial fibrillation: a life-saving catheter ablation for atrial fibrillation and prone position during veno-arterial extracorporeal membrane oxygenation
Masaki Wakita, Yusuke Hosokawa, Shiro Ishihara, Mitsunori Maruyama, Kuniya Asai

TL;DR
A 71-year-old man with severe heart failure and pneumonia was successfully treated with catheter ablation and prone positioning during VA-ECMO.
Contribution
Demonstrates the effectiveness of catheter ablation and prone positioning in VA-ECMO for tachycardia-induced cardiomyopathy.
Findings
Prone positioning during VA-ECMO improved respiratory status without causing complications.
Radiofrequency catheter ablation successfully converted tachycardic AF to sinus rhythm.
LVEF improved from 20% to 55% after treatment.
Abstract
Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) is vital for acute cardio-respiratory failure, but challenges persist sometimes in weaning. Prone positioning, beneficial in veno-venous extracorporeal oxygenation (VV-ECMO), is generally avoided in VA-ECMO patients because of the risks such as bleeding from the catheter insertion site and dislodging of the perfusion cannula or tracheal tube. A 71-year-old male with paroxysmal atrial fibrillation (AF) presented with dyspnoea. Chest computed tomography (CT) and echocardiogram revealed severe pneumonia and decreased cardiac function [left ventricular ejection fraction (LVEF) 20%]. The patient was diagnosed with heart failure complicated by severe pneumonia. Despite treatment, respiratory and circulatory status deteriorated, necessitating a VA-ECMO. Chest CT showed collapsed lungs, especially on the dorsal side. Thus, prone…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
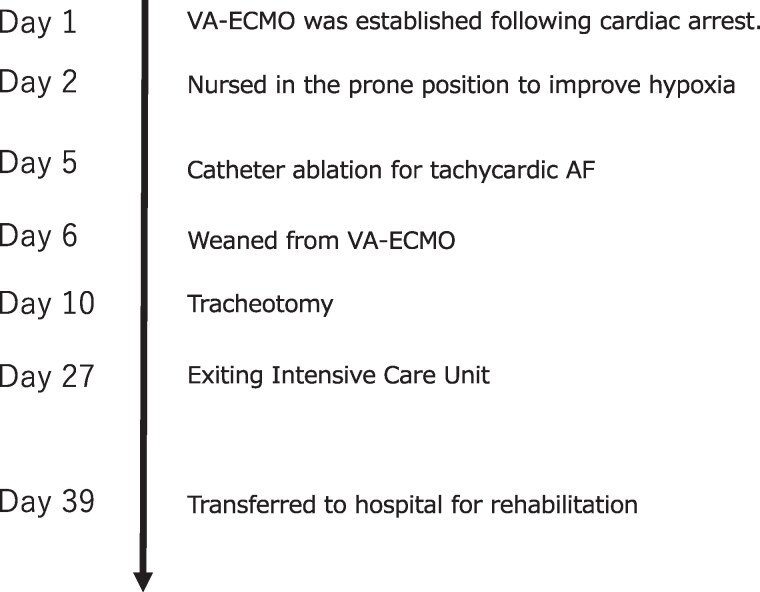 Figure 1
Figure 1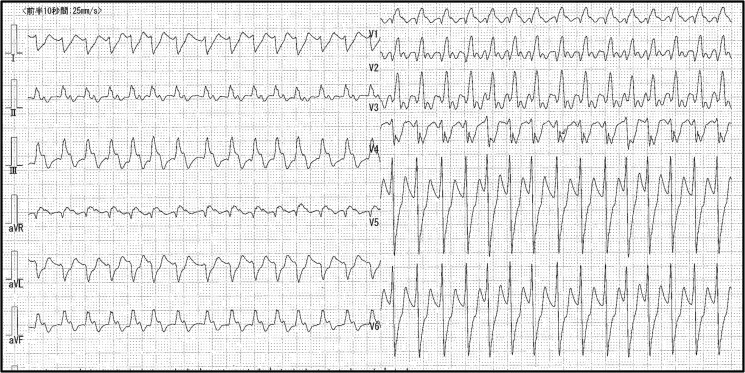 Figure 1
Figure 1 Figure 2
Figure 2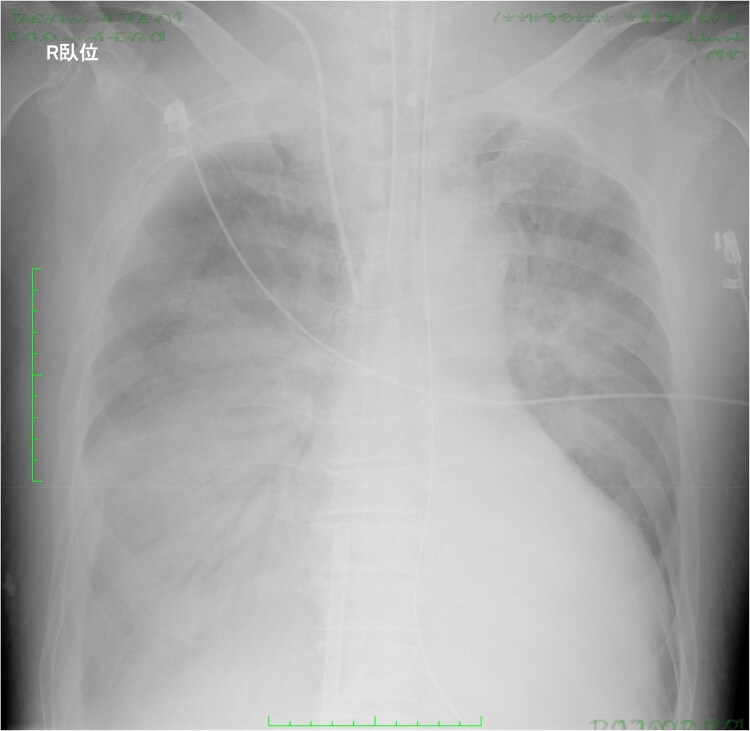 Figure 3
Figure 3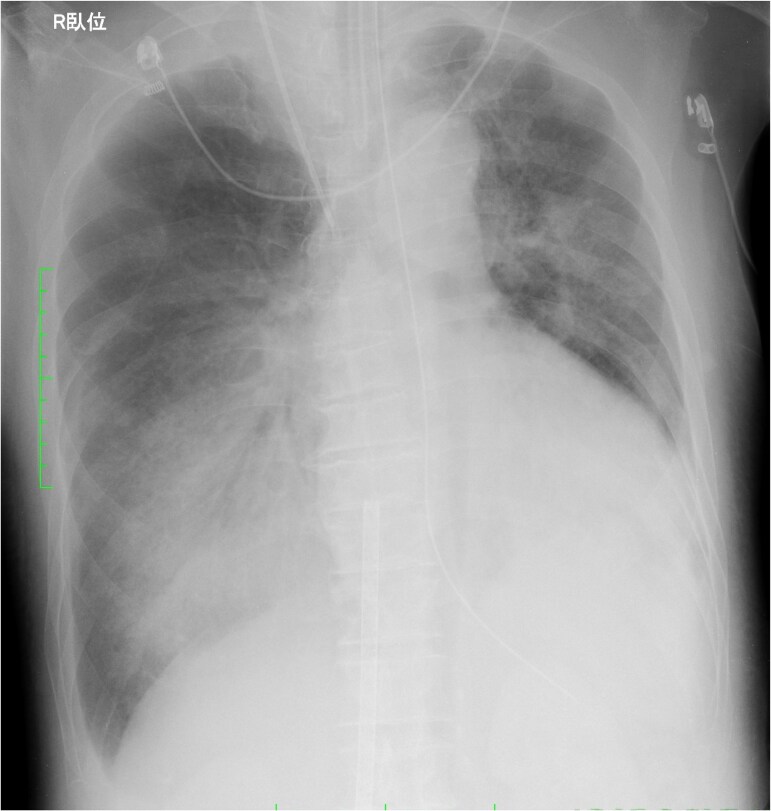 Figure 4
Figure 4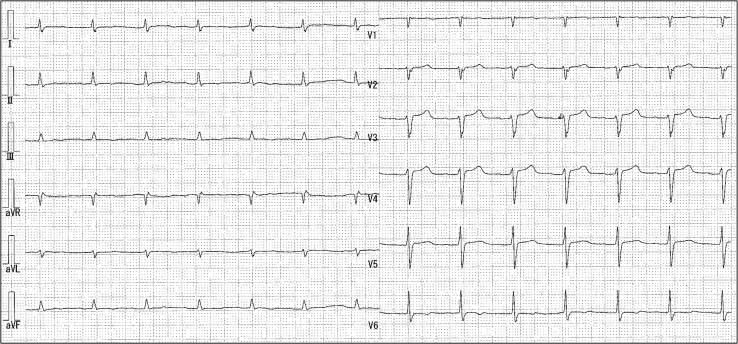 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Atrial Fibrillation Management and Outcomes · Cardiac Arrhythmias and Treatments
Introduction
Veno-venous extracorporeal membrane oxygenation (VV-ECMO) is a treatment option for patients with acute respiratory distress syndrome (ARDS) refractory to medical therapy.^1^ Conversely, veno-arterial extracorporeal membrane oxygenation (VA-ECMO), a crucial intervention for acute cardio-respiratory failure, is used as extracorporeal cardiopulmonary resuscitation (ECPR) for critical conditions such as lethal ventricular arrhythmias.^2^ Improvement of both circulatory and respiratory status is essential for successful weaning from VA-ECMO, but not sufficient in some patients. While prone positioning has been employed to respiratory support for refractory to medical therapy in VV-ECMO patients, it is generally avoided in VA-ECMO patients because of the associated risks such as bleeding from the catheter insertion site and dislodging of the shorter (∼20 cm) arterial cannula inserted via the femoral artery than the venous cannula.
Herein, we present a patient with tachycardic atrial fibrillation (AF) with cardio-respiratory failure requiring VA-ECMO. Restoration of sinus rhythm by radiofrequency catheter ablation (RFCA) of AF greatly facilitated to wean from VA-ECMO. Furthermore, this case represents prone positioning as an effective adjunctive therapy under VA-ECMO support.
Summary figure
**
Case presentation
A 71-year-old Asian man with a history of hypertension and paroxysmal AF presented to our emergency department with anorexia and dyspnoea. Upon admission, his presentation included a heart rate of 178 b.p.m., a blood pressure reading of 86/40 mmHg, and an oxygen saturation level of 78% (10L reservoir mask). Physical examination demonstrated coarse crackles in both lower lung fields. A 12-lead electrocardiogram showed tachycardic AF with ST elevation in aVR lead and ST depression in V3–V6 leads (Figure 1).
Initial electrocardiogram showed tachycardic atrial fibrillation and ST elevation in aVR lead and ST depression in V3–V6 leads.
Blood tests revealed significant abnormalities, including a white cell count of 13 140/μL (reference 4000–9000), C-reactive protein 6.27 mg/L (reference 0–0.3), N-terminal pro-B-type natriuretic peptide 15 494 pg/mL (reference < 125), and troponin T 0.173 ng/mL (reference < 0.014). Chest radiograph and computed tomography (CT) showed bilateral consolidation (Figure 2). The echocardiography revealed impaired left ventricular ejection fraction (LVEF) at 20%. The patient was diagnosed with heart failure complicated by severe pneumonia. He developed pulseless electrical activity due to hypoxia and had return of spontaneous circulation within a few minutes by cardiopulmonary resuscitation. However, his respiratory and circulatory status gradually worsened. Thus, we introduced a VA-ECMO via the right femoral artery and vein with a flow of 3.0 L/min, and norepinephrine (0.15 μg/kg/min) was used to maintain stable haemodynamics.
Massive bilateral consolidation was revealed by chest computed tomography.
Antibiotic administration and a lung protective ventilation strategy were initiated. Nevertheless, it was difficult of ventilator weaning. Despite maintaining systemic oxygenation with VA-ECMO, there was minimal air content in the bilateral lung fields on chest X-ray (Figure 3). Although respiratory physical therapy was performed with adjusting the ventilator setting, chest CT showed collapsed lungs, especially on the dorsal side. Thus, we introduced prone positioning under VA-ECMO to improve respiratory status with attention to potential complications associated with the postural change. Following 8-h prone positioning, his respiratory status and chest X-ray findings (Figure 4) improved dramatically with an increase in air content and an increase in P/F ratio from 263 to 910. The settings of ventilator could be reduced from mode PC, PEEP 12 cmH_2_O, peak pressure 34 cmH_2_O, FiO_2_ 80% to mode PC, PEEP 12 cmH_2_O, peak pressure 26 cmH_2_O, and FiO_2_ 60%.
Chest radiograph revealed minimal air content in the bilateral lung fields.
Following prone positioning, chest radiograph findings improved with an increase in air content.
While the ventilator settings were successfully reduced, we were not able to stabilize the haemodynamic status probably because of tachycardic AF. Because of coronary angiographic and echocardiographic findings and temporal change of cardiac enzyme, we excluded ischaemic heart disease, myocarditis, or Takotsubo cardiomyopathy. Multiple cardioversions with the intra-venous administration of amiodarone failed to restore sinus rhythm, and heart rate was not adequately controlled pharmacologically. Norepinephrine requirement gradually increased, reaching 0.3 μg/kg/min. Thus, we decided to perform RFCA of tachycardic AF under VA-ECMO on Day 5. A duodecapolar electrode catheter (BeeAT; Japan Lifeline) was inserted into the coronary sinus from the right internal jugular vein. Two long sheaths (Swarts and Agilis; Abbott) were advanced into the left atrium through a single transseptal puncture via the right femoral vein distal to the venous ECMO cannula. A duodecapolar ring catheter (Lasso; Biosense Webster) was used to record the pulmonary vein potentials. Circumferential pulmonary vein isolation and conduction block line in the cavo-tricuspid isthmus were made with an irrigated RF ablation catheter under the guidance of an electroanatomical mapping system (Carto 3; Biosense Webster). Sinus rhythm was successfully restored and maintained after ablation. Using dobutamine (2 μg/kg/min), VA-ECMO flow rate was reduced to 1.8 L/min. The patient was successfully weaned from VA-ECMO on Day 7 with stabilization of his circulatory status in sinus rhythm (Figure 5). A tracheostomy was performed on Day 10, considering the need for several weeks to wean the patient off the ventilator. On Day 27, he was weaned from the ventilator and discharged from the Intensive Care Unit to the general ward. The primary cause of the heart failure was considered to be tachycardia-induced cardiomyopathy (TICM), as the LVEF improved to 55%, 28 days after restoration of sinus rhythm. He was then transferred to a rehabilitation hospital on Day 39. After about 5 months of rehabilitation, he had been independently visiting the outpatient clinic. He has continued to attend our hospital since then and has not had any deterioration of heart failure and recurrence of AF.
Electrocardiogram after radiofrequency catheter ablation showed sinus rhythm.
Discussion
To the best of our knowledge, this is the first case of TICM treated by RFCA under VA-ECMO, along with prone positioning for ARDS. Tachycardia-induced cardiomyopathy due to persistent tachycardic AF and severe pneumonia worsened the cardio-respiratory status, necessitating the VA-ECMO. Veno-arterial extracorporeal membrane oxygenation is commonly utilized for life-threatening arrhythmias such as electrical storms, ventricular tachycardia, and ventricular fibrillation but is rarely used in TICM patients.^3^ In this case, multiple cardioversions and pharmacological therapy for rhythm and rate control of tachycardic AF failed, and RFCA for AF was performed to restore sinus rhythm and facilitate weaning from VA-ECMO. To date, only one case of RFCA on VA-ECMO for supraventricular tachycardia has been reported, with no previous reports of RFCA for AF during VA-ECMO support.^4^ In certain clinical settings such as ECPR, drainage and perfusion cannulas are typically inserted via the femoral artery and vein, as was done in this patient. Consequently, deciding on the approach for additional interventions, including percutaneous coronary intervention (PCI) or further circulatory support like intra-aortic balloon pumping and Impella, can be challenging in VA-ECMO patients. Novel techniques, such as single-stick access for PCI under VA-ECMO and Impella, have been reported, using a Y-connector into the arterial return cannula.^5^ Normally, RFCA for AF is performed through the right femoral vein. However, we chose to insert the ablation catheter through the left femoral vein first because the ECMO cannula (20 Fr) had been placed through the right femoral vein. Finally, controlling the catheter proved to be challenging, we performed to puncture the right femoral vein distal to the venous cannula for better control. Since procedural complications can indeed occur with AF ablation and could be considered common,^6^ we performed RFCA with caution, focusing on catheter technique and haemodynamic monitoring because of the potentially higher risk in patients on ECMO support.
This patient was placed in prone position for ARDS under VA-ECMO on the second day of illness. The efficacy of prone positioning in ARDS patients is well established,^7^ and it is also performed in patients with VV-ECMO. The guideline for Adult Respiratory Failure from the Extracorporeal Life Support Organization recommends prone positioning for ECMO patients exhibiting consolidation in the posterior lung fields with some anterior lung fields open.^1^ In this case, the CT scan showed air in the anterior lung and consolidation in the dorsal lung, indicating a good candidate for prone position. Conversely, complications associated with prone positioning in ECMO patients include bleeding from the cannula site, which is the most common complication,^8^ the cannula or airway dislodgement, and haemodynamic instability. However, previous studies on the efficacy and complications of prone positioning have primarily included VV-ECMO patients, with no reports available for patients on VA-ECMO. Notably, the arterial cannula for VA-ECMO inserted via the femoral artery is typically shorter (∼20 cm) than the venous cannula. Consequently, prone positioning in VA-ECMO cases carries a higher risk of cannula dislodgement, presenting a potentially hazardous scenario due to patient movement compared with VV-ECMO cases. The guideline also recommends to prevent dislodgement of the ECMO cannulas.^1^ The option of switching to VV-ECMO before prone positioning was unavailable due to haemodynamic instability resulting from tachycardic AF. Therefore, prone positioning was introduced under VA-ECMO, with meticulous attention to cannulas, puncture sites, airway, and haemodynamic, eventually respiratory states resulted in a dramatic improvement.
Conclusion
Radiofrequency catheter ablation for AF can be an effective intervention even in case of cardio-respiratory failure necessitating VA-ECMO. Additionally, prone positioning can be performed not only in cases of VV-ECMO, but also under VA-ECMO, provided appropriate care is taken.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tonna JE, Abrams D, Brodie D, Greenwood JC, Rubio Mateo-Sidron JA, Usman A, et al Management of adult patients supported with venovenous extracorporeal membrane oxygenation (VV ECMO): guideline from the extracorporeal life support organization (ELSO). ASAIO J 2021;67:601–610.33965970 10.1097/MAT.0000000000001432 PMC 8315725 · doi ↗ · pubmed ↗
- 2Brunner ME, Siegenthaler N, Shah D, Licker MJ, Cikirikcioglu M, Brochard L, et al Extracorporeal membrane oxygenation support as bridge to recovery in a patient with electrical storm related cardiogenic shock. Am J Emerg Med 2013;31:467.e 1–e 6.10.1016/j.ajem.2012.08.04323158602 · doi ↗ · pubmed ↗
- 3Medi C, Kalman JM, Haqqani H, Vohra JK, Morton JB, Sparks PB, et al Tachycardia-mediated cardiomyopathy secondary to focal atrial tachycardia: long-term outcome after catheter ablation. J Am Coll Cardiol 2009;53:1791–1797.19422986 10.1016/j.jacc.2009.02.014 · doi ↗ · pubmed ↗
- 4Scherrer V, Lasgi C, Hariri S, Dureuil B, Savouré A, Tamion F, et al Radiofrequency ablation under extracorporeal membrane oxygenation for atrial tachycardia in postpartum. J Card Surg 2012;27:647–649.22757636 10.1111/j.1540-8191.2012.01487.x · doi ↗ · pubmed ↗
- 5Kapur NK, Hirst CS, Davila CD, Garcia R. Single stick access using a VA-ECMO arterial return cannula for coronary intervention in cardiogenic shock. Catheter Cardiovasc Interv 2021;97:E 673–E 675.32583917 10.1002/ccd.29073 · doi ↗ · pubmed ↗
- 6Gupta A, Perera T, Ganesan A, Sullivan T, Lau DH, Roberts-Thomson KC, et al Complications of catheter ablation of atrial fibrillation: a systematic review. Circ Arrhythm Electrophysiol 2013;6:1082–1088.24243785 10.1161/CIRCEP.113.000768 · doi ↗ · pubmed ↗
- 7Guérin C, Reignier J, Richard JC. Prone positioning in the acute respiratory distress syndrome. N Engl J Med 2013;369:980–981.10.1056/NEJ Mc 130889524004127 · doi ↗ · pubmed ↗
- 8Culbreth RE, Goodfellow LT. Complications of prone positioning during extracorporeal membrane oxygenation for respiratory failure: a systematic review. Respir Care 2016;61:249–254.26464520 10.4187/respcare.03882 · doi ↗ · pubmed ↗