From Starvation to Neurological Crisis: A Case of Wernicke’s Encephalopathy Triggered by Laxative Abuse
Maryana Stryelkina, Britney Constans, Josh Alger, Kendahl Lyle, Aneesh George

TL;DR
A 56-year-old woman with anorexia and laxative abuse developed Wernicke's encephalopathy due to thiamine deficiency, but fully recovered after timely treatment.
Contribution
Highlights a rare nonalcoholic cause of Wernicke's encephalopathy linked to laxative abuse and malnutrition.
Findings
Chronic laxative misuse and severe malnutrition led to thiamine deficiency and WE.
MRI confirmed typical WE brain abnormalities in the medial thalamic and periaqueductal regions.
High-dose thiamine and nutritional support led to full neurological recovery within five days.
Abstract
Wernicke's encephalopathy (WE) is an acute neuropsychiatric disorder resulting from thiamine deficiency, most commonly associated with chronic alcohol use, but it can also arise from rare nonalcoholic etiologies such as anorexia nervosa. This report describes a case of WE in a 56-year-old female patient with anorexia nervosa and chronic laxative misuse, presenting with altered mental status, disorientation, visual disturbances, and ataxia. Clinical evaluation revealed severe malnutrition (BMI 15.0 kg/m²) and multiple electrolyte abnormalities, while MRI findings demonstrated signal abnormalities in the bilateral medial thalamic and periaqueductal gray matter, consistent with WE. Chronic laxative abuse exacerbated thiamine depletion, leading to the development of WE. The patient was treated with high-dose intravenous thiamine and nutritional rehabilitation, resulting in complete recovery…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
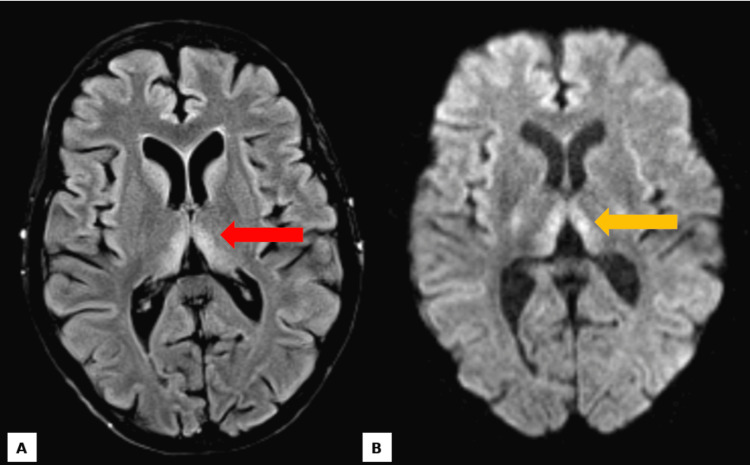 Figure 1
Figure 1| Laboratory Parameters | Patient Values | Status | Reference Ranges | Units |
| Potassium (K⁺) | 2.8 | Low | 3.5 - 5.0 | mmol/L |
| Phosphate (PO₄³⁻) | 1.8 | Low | 2.5 - 4.5 | mg/dL |
| Folate | 1.7 | Low | >4.0 | ng/mL |
| Vitamin B12 | 595.0 | Normal | 200 - 900 | pg/mL |
| Calcium (Ca²⁺) | 8.1 | Low | 8.5 - 10.2 | mg/dL |
| Chloride (Cl⁻) | 105.0 | Normal | 96 - 106 | mmol/L |
| Sodium (Na⁺) | 139.0 | Normal | 135 - 145 | mmol/L |
| Bicarbonate (HCO₃⁻) | 21.0 | Low | 22 - 28 | mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAlcoholism and Thiamine Deficiency · Neurological and metabolic disorders · Infectious Encephalopathies and Encephalitis
Introduction
Wernicke’s encephalopathy (WE) is a potentially fatal neuropsychiatric syndrome caused by thiamine deficiency. While classically associated with chronic alcohol use disorder, nonalcoholic etiologies are increasingly recognized, particularly in conditions associated with malnutrition or impaired thiamine absorption [1-3]. Thiamine is a critical cofactor in enzymatic pathways involved in glucose metabolism and energy production [4]. Its deficiency can lead to cellular energy failure, oxidative stress, and subsequent neuronal injury, particularly in metabolically active brain regions such as the mammillary bodies, medial thalami, and periaqueductal gray matter [5,6].
The clinical presentation of WE is variable and often nonspecific. The classical triad of encephalopathy, oculomotor dysfunction, and ataxia is observed in less than 10% of cases, contributing to frequent delayed diagnosis [7]. In the absence of timely intervention, WE may progress to irreversible neurological deficits, coma, or death [8]. Early recognition and prompt treatment with thiamine are critical to prevent permanent sequelae [9].
Anorexia nervosa, a severe psychiatric disorder characterized by self-imposed caloric restriction, an intense fear of weight gain, and a distorted body image, is a significant risk factor for malnutrition and its complications [10]. Chronic laxative abuse, a common behavior in individuals with eating disorders, further exacerbates nutritional deficiencies by inducing fluid and electrolyte imbalances, impaired nutrient absorption, and depletion of essential vitamins, including thiamine [11]. Despite these known risks, the incidence of Wernicke’s encephalopathy in the context of anorexia nervosa and laxative abuse remains a rare but underreported phenomenon, with limited representation in the medical literature. A systematic review by Oudman et al. analyzed 586 cases of nonalcoholic Wernicke-Korsakoff syndrome and found that approximately 2% were associated with anorexia nervosa, highlighting the rarity of WE in this population [2].
This case report describes a 56-year-old female with a history of anorexia nervosa who developed WE due to acute-on-chronic laxative abuse and severe malnutrition. This case underscores the importance of considering WE in malnourished patients presenting with altered mental status, even in nonalcoholic settings. We aim to emphasize the need for heightened clinical awareness, early diagnosis, and prompt management of WE in atypical presentations to prevent significant morbidity and mortality.
Case presentation
A 56-year-old female presented to the emergency department with altered mental status, visual disturbances, and difficulty walking. Her family reported progressive confusion and unsteady gait over the preceding week. On initial evaluation, she was disoriented (alert but oriented to person only), with slowed speech and difficulty maintaining attention. Neurological examination revealed impaired smooth pursuit eye movements, horizontal nystagmus, and ataxia, including inability to perform finger-to-nose or heel-to-shin testing. Her gait was wide-based and unsteady, requiring assistance to stand.
Physical examination revealed a cachectic, malnourished female with a weight of 40.9 kg and a body mass index (BMI) of 15.0 kg/m², consistent with severe protein-energy malnutrition. Vital signs revealed sinus tachycardia with a heart rate of 101 bpm and a blood pressure of 102/67 mmHg, within the low-normal range. Laboratory studies revealed hypokalemia (2.8 mmol/L), hypophosphatemia (1.8 mg/dL), and a reduced folate level (1.7 ng/mL). Vitamin B12 levels were within the normal range (595 pg/mL). A summary of the patient’s laboratory findings is presented in Table 1.
Magnetic resonance imaging (MRI) of the brain demonstrated bilateral and symmetric hyperintensities in the medial thalami and periaqueductal gray matter on T2-weighted and fluid-attenuated inversion recovery (FLAIR) imaging, findings highly suggestive of Wernicke’s encephalopathy (Figure 1). The T2-weighted axial image (Figure 1A) highlights these signal alterations in the medial thalami, a region particularly vulnerable to thiamine deficiency-related damage. Additionally, axial diffusion-weighted imaging (DWI) (Figure 1B) reveals hyperintensities in the bilateral thalami, further reinforcing the diagnosis. Further history revealed a four-year history of anorexia nervosa, characterized by body image distortion, an extreme fear of weight gain, denial of hunger, and chronic laxative abuse. Two weeks prior to admission, she developed acute-on-chronic exacerbation due to excessive Lasix (furosemide) use (40 mg, unknown frequency), leading to a 5-pound weight loss, further exacerbating her nutritional deficiencies.
MRI FindingsT2-weighted axial image (A, red arrow) demonstrating bilateral and symmetric hyperintense signal alterations localized to the medial portions of the thalami. Axial diffusion-weighted imaging (DWI) (B, yellow arrow) illustrating hyperintensities in the bilateral thalami.
The patient was started on high-dose intravenous thiamine, leading to rapid and significant improvement. By the third day of hospitalization, her mental status improved markedly, with disorientation resolved and coordination partially restored. By the fifth day, she was ambulating with minimal assistance and had fully regained her baseline cognitive function.
Discussion
WE is a well-documented neurologic emergency, yet it remains underdiagnosed, particularly in nonalcoholic settings. This case of WE in the context of anorexia nervosa with chronic laxative abuse highlights several important clinical considerations, including atypical etiologies, diagnostic challenges, and the importance of early intervention to prevent irreversible sequelae.
WE is a well-recognized neurologic emergency, yet it remains underdiagnosed, particularly in nonalcoholic contexts. Although chronic alcohol use disorder is the predominant cause, nonalcoholic etiologies, particularly those associated with malnutrition and impaired thiamine absorption, are increasingly identified [1-3]. This case represents a rare presentation, highlighting the need for increased clinical awareness in nontraditional contexts. The likely cause of thiamine deficiency in this patient was driven by inadequate dietary intake due to anorexia nervosa and the multifaceted effects of chronic laxative abuse. Laxative use accelerates gastrointestinal transit, potentially leading to impaired nutrient absorption in the small intestine, where thiamine is primarily absorbed [12-14]. Laxative-induced diarrhea further exacerbates deficiency through significant fluid and electrolyte losses, increasing metabolic stress and thiamine demand [15]. Additionally, chronic laxative use disrupts gut microbiota, reducing thiamine-producing bacteria and further depleting thiamine stores [16]. These effects, along with baseline malnutrition associated with anorexia nervosa, create a cycle of impaired absorption, increased demand, and worsening deficiency, increasing the risk of severe thiamine deficiency and development of WE.
WE frequently remains underdiagnosed due to its nonspecific clinical presentation. The classic triad of encephalopathy, oculomotor dysfunction, and ataxia are uncommon, often resulting in delayed recognition [7,17]. In this case, the patient exhibited two hallmark features: encephalopathy and ataxia-along with nystagmus, a nonspecific but commonly observed finding in WE. The overlap of these symptoms with other conditions, particularly in malnourished individuals with coexisting psychiatric disorders, underscores the necessity of maintaining a high index of clinical suspicion [18]. Neuroimaging is integral to diagnostic confirmation, as evidenced by this case, where MRI demonstrated symmetric hyperintensities in the medial thalami and periaqueductal gray matter, findings characteristic of WE [19]. These imaging findings highlight the critical role of advanced diagnostic modalities in ensuring timely diagnosis and intervention, particularly in atypical or nonalcoholic presentations.
Early recognition and treatment with high-dose intravenous thiamine are essential to prevent irreversible neurological damage in WE. In this case, the patient’s rapid recovery following timely intervention highlights the condition’s reversibility with appropriate management. Intravenous thiamine, with its superior bioavailability, is the preferred treatment for severe deficiency, ensuring effective restoration of thiamine levels [20].
This case highlights the growing recognition of nonalcoholic WE, particularly in the setting of anorexia nervosa and acute-on-chronic laxative abuse, emphasizing the critical importance of early diagnosis and intervention to prevent disease progression and improve outcomes. Given the high risk of delayed diagnosis in such cases, clinicians should maintain a high index of suspicion when evaluating malnourished patients with altered mental status. Future studies should focus on developing standardized screening protocols for early detection in at-risk populations, ultimately enhancing timely recognition and treatment of WE.
Conclusions
This case contributes to the growing body of literature emphasizing the diverse etiologies of WE and the critical need for increased clinical awareness in atypical presentations. Anorexia nervosa remains a significant but underrepresented risk factor for WE, particularly when compounded by behaviors such as chronic laxative abuse. Increased recognition of this association can facilitate earlier diagnosis and intervention, ultimately improving outcomes for this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Malnutrition-induced Wernicke's encephalopathy following a water-only fasting diet Nutr Clin Pract Hutcheon DA 92993020152552488210.1177/0884533614561793 · doi ↗ · pubmed ↗
- 2Wernicke-Korsakoff syndrome despite no alcohol abuse: a summary of systematic reports J Neurol Sci Oudman E Wijnia JW Oey MJ van Dam M Postma A 11748242620213400067910.1016/j.jns.2021.117482 · doi ↗ · pubmed ↗
- 3Beyond alcoholism: Wernicke-Korsakoff syndrome in patients with psychiatric disorders Cogn Behav Neurol Mc Cormick LM Buchanan JR Onwuameze OE Pierson RK Paradiso S 2092162420112213419110.1097/WNN.0b 013e 31823 f 90c 4PMC 3551444 · doi ↗ · pubmed ↗
- 4The importance of thiamine (vitamin B 1) in humans Biosci Rep Mrowicka M Mrowicki J Dragan G Majsterek I 43202310.1042/BSR 20230374 PMC 1056837337389565 · doi ↗ · pubmed ↗
- 5Thiamin deficiency and brain disorders Nutr Res Rev Butterworth RF 2772841620031908739510.1079/NRR 200367 · doi ↗ · pubmed ↗
- 6Role of mitochondrial dysfunction and oxidative stress in the pathogenesis of selective neuronal loss in Wernicke's encephalopathy Mol Neurobiol Desjardins P Butterworth RF 17253120051595380910.1385/MN:31:1-3:017 · doi ↗ · pubmed ↗
- 7Wernicke encephalopathy-clinical pearls Mayo Clin Proc Sinha S Kataria A Kolla BP Thusius N Loukianova LL 106510729420193117111610.1016/j.mayocp.2019.02.018 · doi ↗ · pubmed ↗
- 8Wernicke's encephalopathy with cortical abnormalities: clinicoradiological features: report of 3 new cases and review of the literature Eur Neurol Sakurai K Sasaki S Hara M Yamawaki T Shibamoto Y 2742806220091969042010.1159/000235596 · doi ↗ · pubmed ↗