Disseminated Ureaplasma urealyticum Infection and Hyperammonemic Encephalopathy in a Patient With Activated PI3K Delta Syndrome 2
Yi Wye Lai, Ray Junhao Lin, Matthias Maiwald, Gareth Zigui Lim, Pooja Rao, Tse Hsien Koh, Ser Hon Puah, Teck Choon Tan, Hwee Siew Howe, Xin Rong Lim

TL;DR
A young woman with a rare immune syndrome developed a Ureaplasma infection leading to brain-affecting high ammonia levels, a condition usually seen in transplant patients.
Contribution
This case report expands the understanding of Ureaplasma-associated hyperammonemia beyond transplant recipients.
Findings
Disseminated Ureaplasma urealyticum infection caused hyperammonemic encephalopathy in a non-transplant patient.
The patient had activated PI3K delta syndrome 2, a rare primary immunodeficiency.
Literature review suggests Ureaplasma-associated hyperammonemia can occur in non-transplant individuals.
Abstract
Hyperammonemia syndrome (HS) from Ureaplasma infection is typically reported in posttransplant recipients, particularly lung transplant. We describe a young woman with activated PI3K delta syndrome 2 who presented with HS from disseminated Ureaplasma urealyticum infection with septic arthritis. We also performed a literature review of Ureaplasma-associated HS in nontransplant patients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
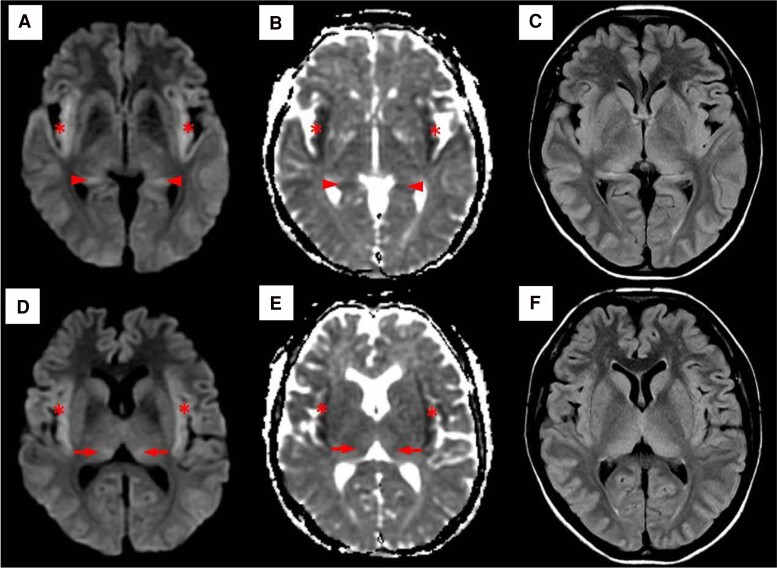 Figure 1
Figure 1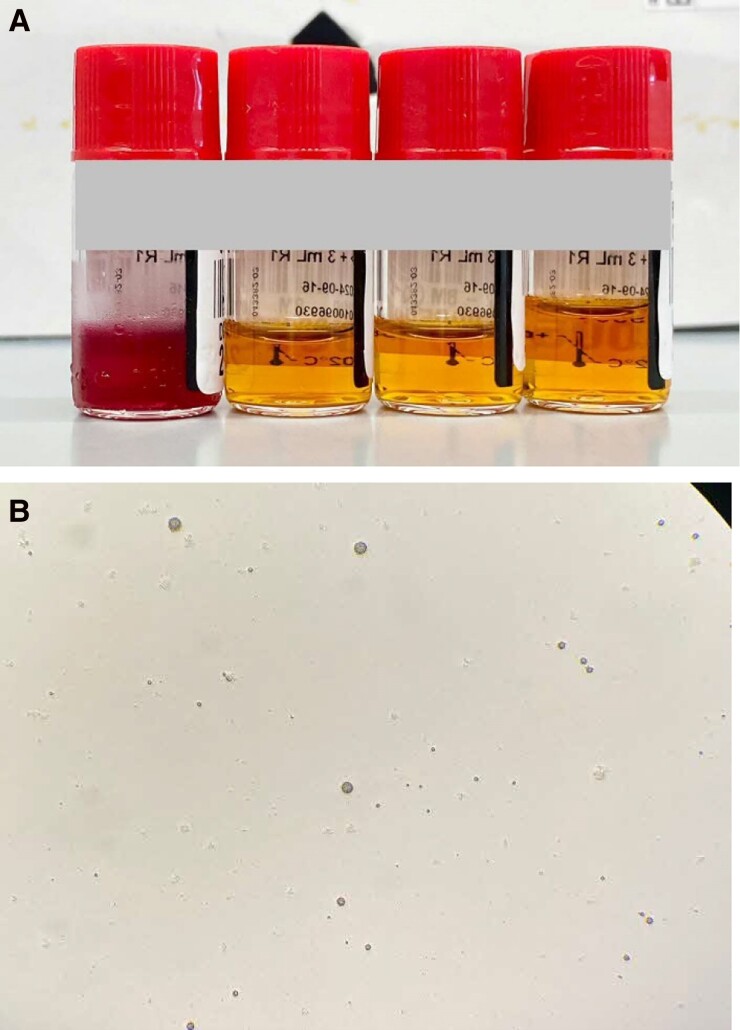 Figure 2
Figure 2| First Author (Year) | Case Presentation | Microbiological Diagnosis |
| Clinical Outcomes | Risk Factors |
|---|---|---|---|---|---|
| Details included in table for reference Present Study | 31-year-old woman with HS (altered mental status, status epilepticus, cerebral edema) and septic arthritis | Blood cultures, bone marrow aspirate, synovial tissue PCR returned positive for | Doxycycline (100 mg 12 h) for 1 wk given 2 mo prior to onset of HS, no | Died | Primary immunodeficiency APDS, hypogammaglobulinemia, rituximab (1 g × 2 doses given 2 mo priora) and low-to-moderate doses (5–20 mg/d) of prednisolone (started 1 y prior |
| Bharath (2023) [ | 57-year-old man with HS (status epilepticus, cerebral edema) and septic arthritis | Serum PCR positive for | Doxycycline | Died from complications of multiorgan failure, bowel ischemia | Dermatomyositis, seronegative rheumatoid arthritis, and interstitial lung disease on immunosuppression with methotrexate |
| Rahman (2023) [ | 22-year-old woman with HS (encephalopathy, coma), pelvic abscess, serositis, and septic arthritis | Respiratory and urinary PCR positive for | Doxycycline | Recovered after 7 d of antibiotics | Granulomatous polyangiitis on rituximab |
| Pan (2022) [ | 65-year-old man with HS (delirium, slurred speech, and agitation) and septic monoarthritis | Synovial fluid metagenomic sequencing test reported sequences of | NIL, discharged against medical advice | Died | Chronic hepatitis B, alcohol abuse, previous tuberculosis |
| Kok (2022) [ | 67-year-old woman with HS (altered mental status) | Blood culture positive for | Minocycline 100 mg q12h for 1 wk, then azithromycin 500 mg OD for 1 wk; 2 wk | Recovered but eventually died from other nosocomial infections | Pancreatic head adenocarcinoma, completed neoadjuvant chemotherapy 11 mo priora and adjuvant chemotherapy (tegafur, gemeraci, oteracil) given 3 mo prior |
| Tawfik (2021) [ | 53-year-old woman with HS (status epilepticus, cerebral edema) and pneumonia | BAL PCR for | Doxycycline | Withdrawal of care, died | Myeloablative allogeneic hematopoietic cell transplant 11 mo prior, CAR T-cell therapy (lympho-depleting therapy consisting of cyclophosphamide |
| Nowbakht (2019) [ | 32-year-old woman with HS (seizures) | Serum PCR panel positive for | Levofloxacin | Died | B-cell ALL status post methotrexate, vincristine, pegasparaginase, and dexamethasone; diabetes mellitus (glycemic control not specified) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetabolism and Genetic Disorders · Neurological and metabolic disorders · Infectious Encephalopathies and Encephalitis
CASE REPORT
A 31-year-old Chinese woman with activated PI3K delta syndrome (APDS) 2 presented in June 2024 with 4 days of progressive polyarthritis affecting the wrists, elbows, knees, and ankles.
In 2017, at 24 years of age, she was diagnosed with PIK3R1 mutation (c.1425 + 1G > A) and had recurrent sinopulmonary infections, herpes zoster, maxillary sinus fungal mycetoma, bronchiectasis, hypogammaglobulinemia, chronic lymphoproliferation (persistent lymphadenopathy, development of mucosa-associated lymphoid tissue [MALT] lymphoma of the parotid glands in 2014, with recurrence in 2017), and autoimmunity. She displayed signs of systemic lupus erythematosus and Sjögren syndrome such as a malar rash, oral ulcers, Raynaud phenomenon, keratoconjunctivitis, arthralgia, cutaneous vasculitis, hypocomplementemia, positive anti-double-stranded DNA, and anti-Ro antibodies. She was on monthly replacement intravenous immunoglobulin (IVIG) and prednisolone at doses of 5–10 mg per day and had previously been treated with azathioprine, sirolimus, and multiple courses of rituximab.
She developed arthritis of the right elbow in June 2023, followed by arthritis of the right midfoot in December 2023 and right knee in April 2024. Repeated arthrocentesis of the right elbow joint was negative on Gram stain examinations and aerobic, anaerobic, mycobacterial, and fungal cultures. From November 2023 to April 2024, she missed medical appointments and treatment, including IVIG replacement. She was sexually active with her male partner and developed per-vaginal discharge in September 2023, which was treated with an antifungal vaginal pessary. In early 2024, she was diagnosed and treated for bacterial vaginosis in another facility. She was admitted for right corneal melt and arthritis of the right elbow in April 2024. As the ophthalmologist opined that the corneal melt was related to corticosteroid use, cultures from the right cornea were not obtained, and treatment involved application of corneal glue. Debridement and washout of the right knee and elbow under anesthesia was performed; no pus was seen intraoperatively. Chronic inflammation was found on synovial histology; stains for fungi and acid-fast bacteria were negative. Empiric treatment for septic arthritis with intravenous (IV) ceftriaxone and oral doxycycline therapy was stopped after a week, as synovial fluid cultures for bacteria, fungi, and mycobacteria, as well as polymerase chain reaction (PCR) tests for gonococcus and chlamydia, were all negative. As all microbiology was negative, she was treated for inflammatory arthritis with IV rituximab 1 g for 2 doses and prednisolone up to 20 mg/day and was reinstituted on monthly replacement IVIG. She responded clinically to treatment; however, approximately a month later, her symptoms recurred, prompting another admission in June 2024.
On examination, she was afebrile, with normal vital signs. There were multiple tender and swollen elbow, wrist, hand, knee, and ankle joints. Cardiovascular, respiratory, abdominal, and integumentary examinations were normal. Investigations revealed anemia with hemoglobin (Hb) 7.7 (11.8–14.6) g/dL, leukocytosis with white blood cell (WBC) count 14.7 (4.0–9.6) × 10^9^ cells/L, reactive thrombocytosis with platelet count 409 (15–360) × 10^9^/L, and C-reactive protein (CRP) of 299.3 (0.0–5.0) mg/L. Magnetic resonance imaging (MRI) of her right ankle showed tenosynovitis of the extensor tendons anterior to the ankle joint, with no evidence of abscess or osteomyelitis.
On day 5 of admission, she developed a single febrile episode of 38.6°C without any localizing symptoms. Blood cultures were negative and computed tomographic scan of the abdomen and pelvis revealed no occult source of infection. Urine cultures grew extended-spectrum β-lactamase–producing Klebsiella pneumoniae and Escherichia coli, which were treated with a 10-day course of ertapenem.
She was also diagnosed with major depressive disorder during her admission. She refused proposed key diagnostic investigations such as repeat arthrocentesis and washout, orthopedic consultation, and treatment, including antidepressants.
On day 29 of admission, she was found unarousable (Glasgow Coma Scale E1V1M1) with right gaze deviation and was intubated and transferred to the intensive care unit. Investigations showed anemia (Hb 9.6 g/dL), marked leukocytosis with neutrophilic predominance (WBC count 31.4 × 10^9^ cells/L), thrombocytosis (platelet count 800 × 10^9^/L), CRP 345.3 mg/L, marked hyperammonemia of >600 (16–52) μmol/L, hypogammaglobulinemia (immunoglobulin G, 4.3 g/L; immunoglobulin A, <0.4 g/L; immunoglobulin M, <0.3 g/L), with normal renal and liver function tests. Symmetrical areas of restricted diffusion and fluid-attenuated inversion recovery hyperintensities in bilateral insular regions and thalami (Figure 1) were seen on brain MRI, raising concerns for herpes simplex encephalitis. Lumbar puncture showed mild lymphocytic pleocytosis on cerebrospinal fluid (CSF) analysis (nucleated cells 11 [0–5] cells/μL, 85% lymphocytes) and negative results for all microbiological studies (aerobic, anaerobic, mycobacteria, and fungal culture; cryptococcus antigen; and PCR for herpes simplex virus, varicella zoster virus, cytomegalovirus, and Toxoplasma gondii). She subsequently developed status epilepticus (electroencephalography confirmed) that required 4 anti-epileptic agents for control. Bone marrow aspiration and biopsy was done due to previous history of MALT lymphoma and consideration of primary central nervous system (CNS) lymphoma and paraneoplastic encephalitis; this returned negative. She was empirically treated with IV acyclovir, ampicillin, ceftriaxone, and vancomycin for infective meningoencephalitis. She was also initiated on IV sodium benzoate and continuous renal replacement therapy (CRRT) for hyperammonemia, but CRRT was terminated when she developed hypotension and cardiac arrest. She eventually died on day 31 of admission. In a postmortem review, the clinical suspicion for Ureaplasma- or Mycoplasma-associated hyperammonemia prompted further investigations using her antemortem samples. Blood culture samples transferred to specialized medium grew Ureaplasma species (Figure 2). Five-plex PCR for Trichomonas vaginalis, Mycoplasma genitalium, Mycoplasma hominis, Ureaplasma urealyticum, and Ureaplasma parvum performed on residual bone marrow aspirate and synovial tissue from the knee obtained during surgical washout in April 2024 were also positive for U urealyticum, with all showing a cycle threshold value of approximately 32 (Figures 1 and 2).
Axial brain magnetic resonance imaging showed bilateral symmetrical diffusion-weighted imaging hyperintense (A and D) and apparent diffusion coefficient hypointense (B and E) signal abnormalities in the bilateral insula (), medial thalami (arrows), and hippocampi (arrowheads), consistent with restricted diffusion in these areas. These regions also showed corresponding symmetrical T2 fluid-attenuated inversion recovery hyperintensities (C and F).*
A, R2 medium from Urée-Arginine LYO 2 kit (bioMérieux SA, Marcy-l’Etoile, France). From left, uninoculated bottle and inoculated bottles at neat, 1:10, and 1:100 showing a color change indicating hydrolysis of urea. B, Small dark colonies of variable size seen on A7 agar (ELITech Microbio, Signes, France).
LITERATURE REVIEW
We searched PubMed and Embase from January 1990 to August 2024 for reports of hyperammonemia syndrome (HS) and Ureaplasma infection in nontransplant recipients (see details in the Supplementary material). We found 6 such cases; their clinical presentation, risk factors, and treatment are summarized in Table 1.
DISCUSSION
Ureaplasma species reside in the urogenital and respiratory tracts as part of the normal bacterial flora, but immunosuppression or instrumentation predisposes to penetration of the organism into the submucosa [7]. The unique characteristic of Ureaplasma species that metabolize urea for adenosine triphosphate production is typically inconsequential to the immunocompetent host, but when there is systemic infection, particularly in an immunocompromised host, this may pose a significant threat to ammonia clearance, leading to HS [8]. HS, characterized by excessive serum concentration of ammonia and resultant progressive neurologic dysfunction, is well-recognized in posttransplant patients [8]. There is a disproportionately increased incidence in lung transplant patients, in part contributed by donor respiratory tract colonization [8]. Our literature review of Ureaplasma-induced HS in nontransplant patients revealed risk factors of secondary humoral immunodeficiency, such as prolonged steroid use, rituximab use, B-cell acute lymphoblastic leukemia, myeloablation, chimeric antigen receptor T-cell therapy, malnutrition from chronic alcoholism, and chemotherapy [1–6]. In our patient, the primary site of infection appeared to be septic arthritis, probably arising from a urogenital source, with subsequent intensification of immunosuppression contributing to the development of HS.
Mortality is extremely high in nontransplant cases, even with appropriate treatment (∼83%, all cases died except 1), possibly contributed to in part by delays in diagnosis [1–6]. In comparison, the mortality of HS posttransplant is about 50%–70% [9].
Ureaplasma detection requires specialized PCR tests or media for culture, and infections respond poorly to commonly used empirical antibiotic regimens (eg, β-lactam antibiotics) [7, 10]. PCR assays for Ureaplasma performed on serum are not widely available and their performance characteristics are not well described. However, our review revealed several cases in which PCR on serum samples was used for diagnosis [1, 4, 6]. This seems to suggest that bacteremia is not uncommon in Ureaplasma-associated HS.
Ureaplasma is innately resistant to β-lactams, displaying susceptibility to mainly tetracyclines, macrolides, and fluoroquinolones [7]. We observed from our literature review that the 2 cases who recovered were treated with minocycline and doxycycline, as compared to the 2 cases treated with levofloxacin who died [2, 4–6]. This observation may be explained by naturally occurring mutations in the parC and parE regions of the Ureaplasma chromosome that confers resistance to fluroquinolones [11]. In the United States, the estimated prevalence of such mutations is 5%–6% [11].
Our patient continued to deteriorate despite 1 week of doxycycline treatment. Possible reasons for this may be due to the increased immunosuppression from treatment of possible reactive inflammatory arthritis, the bacteriostatic nature of doxycycline (compared to the bactericidal action of fluoroquinolones), and possibly an inadequate duration of treatment, considering that the literature review suggested that most cases of septic arthritis had treatment ranging several weeks up to months [12–15]. It may also be possible that the isolate had a high doxycycline minimum inhibitory concentration, but unfortunately antibiotic susceptibility testing was not available for us to test this hypothesis. Considerations of these aforementioned factors may influence the initial choice of antibiotics for empirical treatment of Ureaplasma infections and decisions for treatment duration.
In our patient, the diagnostic challenge was contributed to by the absence of fever; intermittent adherence to treatment, which hindered clinical assessment of treatment response; her refusal to cooperate with medical care and treatment; and the difficulty in differentiating infective arthritis from inflammatory arthritis. Existing literature on presentation of Ureaplasma septic arthritis in immunocompetent patients reports fever and suppurative arthritis [3, 15]. Conversely, immunocompromised patients may remain afebrile or only develop fever later on in the disease course, manifesting only with severe debilitating oligo-polyarthritis [1, 2, 14]. It is possible that our patient's underlying immunodeficiency with subsequent additional immunosuppression may have blunted her ability to mount a febrile response.
In retrospect, risk factors of severe hypogammaglobulinemia from underlying primary immunodeficiency, recent rituximab use, persistently raised CRP despite antibiotics, presence of HS without any liver pathology, and requirement of moderate to high doses of steroids for arthritis control should raise suspicion for an atypical infection. When her initial cultures returned negative, a referral to infectious diseases and extended microbial testing should have been considered.
MRI findings in HS typically include symmetrical signal abnormalities in the insula, cingulate cortices, and thalami [16]. In this case, the MRI brain findings were classic of hyperammonemic encephalopathy, necessitating urgent treatment with dialysis and ammonia scavengers (Figure 1) [16]. The presence of mild CSF pleocytosis may have suggested Ureaplasma CNS involvement; however, there were insufficient samples to test for this.
In summary, we present a case of fatal U urealyticum infection with acute and rapid deterioration, emphasizing the need for a heightened clinical suspicion in immunocompromised nontransplant hosts, in order to diagnose and institute management early. Although Ureaplasma infection manifesting as HS is typically associated with transplant recipients, it should also be considered in nontransplant immunocompromised patients with unexplained neurological dysfunction; more so in those with supportive neuro-radiological findings. Ammonia testing may be considered in this setting and, if elevated, should prompt PCR testing and incubation of microbiological samples in specialized culture media. Given that routinely used antibiotics are not active against Ureaplasma species, atypical antibiotic coverage should be added when the clinical suspicion is high.
Supplementary Data
Supplementary materials are available at Open Forum Infectious Diseases online. Consisting of data provided by the authors to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the authors, so questions or comments should be addressed to the corresponding author.
Supplementary Material
ofaf084_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bharath SP, Pang H, Kaderi T, et al Pearls and oy-sters: status epilepticus and cerebral edema from hyperammonemia due to disseminated Ureaplasma and Mycoplasma species. Neurology 2023; 100:727–31.36564204 10.1212/WNL.0000000000206778 PMC 10103116 · doi ↗ · pubmed ↗
- 2Rahman O, Younas Z, Agard A, et al Disseminated Ureaplasma urealyticum infection and life-threatening hyperammoniemia with rituximab use. Crit Care Med 2023; 51:193.
- 3Pan X, Xu J, Pan L, et al Hyperammonemia in a septic patient with Ureaplasma parvum arthritis: a case report. BMC Infect Dis 2022; 22:958.36550469 10.1186/s 12879-022-07953-8PMC 9783457 · doi ↗ · pubmed ↗
- 4Kok EJY, Lee YL. Ureaplasma urealyticum infection presenting as altered mental status in a post-chemotherapy patient: case report and literature review. Front Med (Lausanne) 2022; 9:1057591.36507505 10.3389/fmed.2022.1057591 PMC 9733668 · doi ↗ · pubmed ↗
- 5Tawfik P, Arndt P. Lethal hyperammonemia in a CAR-T cell recipient due to Ureaplasma pneumonia: a case report of a unique severe complication. BMJ Case Rep 2021; 14:e 242513.10.1136/bcr-2021-242513 PMC 827347534244183 · doi ↗ · pubmed ↗
- 6Nowbakht C, Edwards AR, Rodriguez-Buritica DF, et al Two cases of fatal hyperammonemia syndrome due to Mycoplasma hominis and Ureaplasma urealyticum in immunocompromised patients outside lung transplant recipients. Open Forum Infect Dis 2019; 6:ofz 033.30863787 10.1093/ofid/ofz 033PMC 6405933 · doi ↗ · pubmed ↗
- 7Kokkayil P, Dhawan B. Ureaplasma: current perspectives. Indian J Med Microbiol 2015; 33:205–14.25865969 10.4103/0255-0857.154850 · doi ↗ · pubmed ↗
- 8Tantengco OAG, De Jesus FCC 2nd, Gampoy EFS, Ornos EDB, Vidal MS Jr, Abad CLR. Hyperammonemia syndrome associated with Ureaplasma spp. infections in immunocompromised patients and transplant recipients: a systematic review and meta-analysis. Clin Transplant 2021; 35:e 14334.33948993 10.1111/ctr.14334 · doi ↗ · pubmed ↗