From pericarditis to giant cell arteritis: leveraging FDG PET CT for accurate diagnosis and treatment
Fatima K Alduraibi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
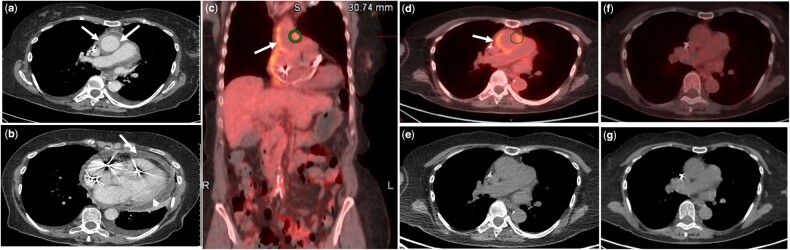 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Myasthenia Gravis and Thymoma · Pericarditis and Cardiac Tamponade
An 81-year-old female with a past medical history of atrial fibrillation and sick sinus syndrome presented with persistent chest pain, low-grade fever and malaise. Initial workup revealed elevated CRP (204), ESR (41) and a moderate pericardial effusion without vegetation on echocardiogram. She was diagnosed with idiopathic pericarditis and treated with ibuprofen and colchicine.
She returned with recurrent fever, persistently high CRP (244), ESR (56) and leucocytosis. Haematologic, autoimmune and infectious studies were unremarkable. Repeat echocardiogram showed a small pericardial effusion, while cardiac MRA ruled out vasculitis. Axial enhanced chest CT revealed circumferential aortic wall thickening with enhancement and mild fat stranding (Fig. 1a, arrows), pericardial wall thickening with mild enhancement (Fig. 1b, arrowhead) and pericardial effusion (Fig. 1b, arrow). Fused coronal FDG PET/CT (Fig. 1c) and fused axial FDG PET/CT (Fig. 1d) demonstrated increased FDG uptake in the walls of the ascending aorta ( arrow), descending aorta and bilateral iliac arteries, confirming vasculitis consistent with giant cell arteritis. An axial non-enhanced chest CT (Fig. 1e) showed circumferential aortic wall thickening with mild fat stranding ( arrow).
She was started on prednisone, leading to clinical improvement. A 4-month follow-up FDG PET/CT showed normal FDG distribution and resolution of the prior findings (Fig. 1f–g).