Predictors of long-term success after successful explantation of continuous flow left ventricular assist device support
Takayuki Gyoten, Eisuke Amiya, Akihito Saito, Minoru Ono

TL;DR
This study identifies a time interval predictor for successful removal of heart assist devices in patients with heart failure.
Contribution
The study identifies a specific time interval as a predictor for successful cf-LVAD explantation in non-ischaemic dilated cardiomyopathy patients.
Findings
A time interval of 7 months between first heart failure event and cf-LVAD implantation predicts successful explantation.
Patients with successful explantation showed significant improvement in left ventricular function and dimensions.
Survival rate free from rehospitalization after explantation was 100% at a median follow-up of 30 months.
Abstract
Predictors and evaluations of continuous flow left ventricular assist device (cf-LVAD) explantation in recovered patients remain under discussion due to lack of evidence on long-term safety and efficacy. This study summarized our experiences regarding cf-LVAD explantation in non-ischaemic dilated cardiomyopathy patients and estimated a predictor for sufficient myocardial recovery allowing left ventricular assist device explant. We retrospectively identified 135 adult patients with cf-LVAD therapy as bridge to heart transplant due to non-ischaemic dilated cardiomyopathy. Of those, 13 patients underwent device explantation (recovery group) after myocardial recovery. Twelve (92%) of the explanted patients were evaluated using our weaning protocol and underwent surgical explantation. Meanwhile, the remaining 122 continued with cf-LVAD therapy (non-recovery group). Multivariate logistic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
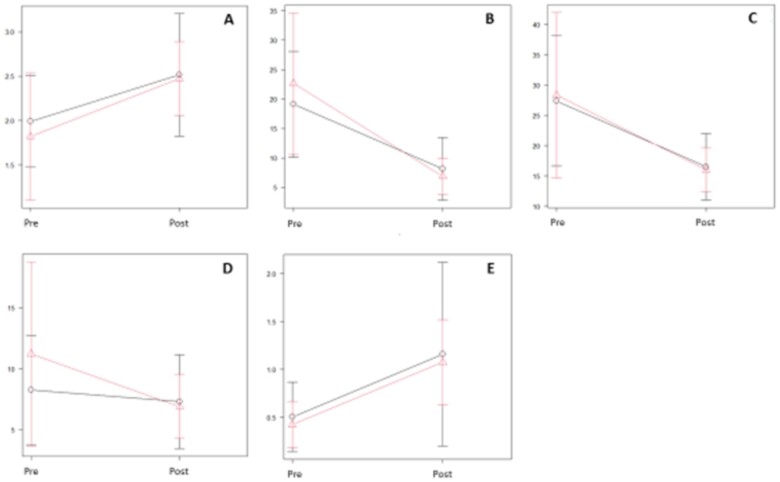 Figure 1
Figure 1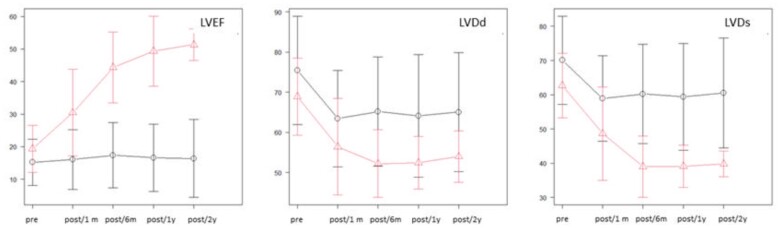 Figure 2
Figure 2| Variables |
|
|---|---|
| Perioperative outcomes | |
| Extubation <24 h | 6 (46%) |
| Intensive care unit stay (days), median (IQR) | 4 (3–4) |
| In-hospital stay (days), median (IQR) | 30 (23–36) |
| Medication at discharge | |
| Beta-blocker | 13 (100%) |
| Angiotensin-converting enzyme inhibitor/angiotensin receptor blocker | 13 (100%) |
| Mineralocorticoid receptor antagonist | 9 (69%) |
| At discharge | |
| Home | 13 (100%) |
| Hospital | 0 (0%) |
| Rehabilitation | 0 (0%) |
| Long-term follow-up | |
| All-cause mortality | 0 (0%) |
| Major adverse cardiovascular events | 0 (0%) |
| Cardiac death | 0 (0%) |
| Cerebrovascular accident | 0 (0%) |
| Re-ventricular assist device implantation | 0 (0%) |
| Heart transplantation | 0 (0%) |
| Re-admission due to heart failure | 0 (0%) |
| Infection (sepsis) | 0 (0%) |
| Variable | All, | Recovery group, | Non-recovery group, |
|
|---|---|---|---|---|
| Age (years), median (IQR) | 42 (35–52) | 37 (34–40) | 43 (35–52) | 0.097 |
| Male gender | 104 (77%) | 10 (77%) | 94 (77%) | 1 |
| Body mass index (kg/m2), median (IQR) | 20 (18–22) | 22 (20–25) | 20 (18–22) | 0.056 |
| Body surface area (m2), median (IQR) | 1.67 (1.53–1.76) | 1.75 (1.57–1.82) | 1.67 (1.53–1.75) | 0.25 |
| Hypertension | 12 (9%) | 3 (23%) | 9 (7%) | 0.084 |
| History of stroke | 23 (17%) | 1 (8%) | 22 (18%) | 0.47 |
| Chronic obstructive lung disease | 2 (1%) | 0 (0%) | 2 (2%) | 1 |
| Diabetes mellitus | 23 (17%) | 4 (31%) | 19 (16%) | 0.24 |
| Hyperlipidemia | 17 (13%) | 5 (38%) | 12 (10%) | 0.012 |
| Chronic atrial fibrillation | 27 (20%) | 0 (0%) | 27 (22%) | 0.07 |
| Prior cardiac resynchronization therapy | 64 (47%) | 0 (0%) | 64 (52%) | <0.005 |
| Prior intra-aortic balloon pump | 20 (15%) | 0 (0%) | 20 (16%) | 0.22 |
| Prior open cardiac surgery | 39 (29%) | 2 (15%) | 37 (30%) | 0.35 |
| Time between first heart failure event and LVAD implantation (months), median (IQR) | 73 (32–121) | 4 (2.0–7.0) | 77 (43–132) | <0.005 |
| Medication | ||||
| Beta-blocker | 131 (97%) | 12 (92%) | 119 (98%) | 1 |
| Dose (carvedilol) (mg), median (IQR) | 12.5 (5–25) | 6.25 (1.25–10) | 12.5 (5–25) | 0.0105 |
| Angiotensin-converting enzyme inhibitor/angiotensin receptor blocker | 108 (80%) | 8 (62%) | 100 (82%) | 0.25 |
| Mineralocorticoid receptor antagonist | 75 (56%) | 9 (69%) | 66 (54%) | 0.23 |
| Laboratory, median (IQR) | ||||
| Haemoglobin (g/dl) | 11.2 (10.1–12.6) | 11.6 (10.8–12.2) | 11.2 (10.0–12.7) | 0.58 |
| Haematocrit (%) | 34.1 (30.8–37.4) | 34.7 (32.1–37.0) | 34.1 (30.7–37.4) | 0.8 |
| Creatinine (mg/dl) | 0.88 (0.72–1.12) | 0.76 (0.65–1.02) | 0.90 (0.72–1.13) | 0.17 |
| Creatinine clearance (ml/min) | 72 (54–93) | 87 (70–93) | 69 (54–93) | 0.18 |
| Brain natriuretic peptide (pg/ml) | 510 (218–784) | 203 (124–626) | 514 (235–795) | 0.079 |
| Aspartate aminotransferase (IU/l) | 24 (19–33) | 18 (15–24) | 26 (20–34) | 0.0083 |
| Alanine aminotransferase (IU/l) | 22 (15–35) | 17 (11–27) | 22 (15–36) | 0.21 |
| Total protein (g/dl) | 6.6 (6.1–7.0) | 6.2 (5.8–7.0) | 6.6 (6.1–7.0) | 0.29 |
| Albumin (g/dl) | 3.6 (3.2–4.0) | 3.6 (3.2–3.8) | 3.7 (3.2–4.0) | 0.69 |
| Lactate dehydrogenase (IU/l) | 253 (209–317) | 210 (169–290) | 257 (211–317) | 0.11 |
| Total cholesterol (mg/dl) | 151 (127–180) | 180 (147–210) | 150 (127–177) | 0.044 |
| Total bilirubin (mg/dl) | 0.9 (0.7–1.5) | 0.70 (0.50–1.1) | 1.0 (0.70–1.5) | 0.05 |
| Direct bilirubin (mg/dl) | 0.4 (0.2–0.6) | 0.35 (0.18–0.43) | 0.40 (0.20–0.60) | 0.28 |
| High-density lipoprotein (mg/dl) | 47 (36–58) | 43 (38–52) | 47 (36–60) | 0.68 |
| Low-density lipoprotein (mg/dl) | 85 (69–113) | 100 (75–132) | 84 (69–112) | 0.17 |
| Haemoglobin A1c (%) | 5.7 (5.2–6.1) | 5.9 (5.7–6.0) | 5.6 (5.2–6.1) | 0.41 |
| Fasting blood sugar (mg/dl) | 95 (84–111) | 95 (91–118) | 95 (84–111) | 0.55 |
| Electrocardiogram | ||||
| QRS (s) | 0.12 (0.11–0.15) | 0.11 (0.098–0.12) | 0.13 (0.11–0.16) | 0.043 |
| QRS <0.12 s | 59 (44%) | 9 (69%) | 50 (41%) | 0.023 |
| QTc (ms) | 0.48 (0.45–0.52) | 0.49 (0.48–0.51) | 0.48 (0.45–0.52) | 0.3 |
| Respiratory function, median (IQR) | ||||
| %VC (%) | 84 (70–95) | 84 (78–87) | 84 (70–95) | 0.78 |
| FEV1 (%) | 80 (75–85) | 88 (82–89) | 79 (75–85) | 0.11 |
| DLCO (ml/min/mmHg) | 68 (28–83) | 82 (44–84) | 68 (27–83) | 0.58 |
| INTERMACS level, median (IQR) | 3 (2–3) | 2 (2–3) | 3 (2–3) | 0.139 |
| Level 1 | 2 (1%) | 0 (0%) | 2 (2%) | |
| Level 2 | 64 (47%) | 9 (69%) | 55 (45%) | |
| Level 3 | 66 (49%) | 4 (31%) | 62 (51%) | |
| Level 4 | 3 (2%) | 0 (0%) | 3 (2%) | |
| Temporary MCS | ||||
| Prior IABP | 49 (36%) | 7 (54%) | 42 (34%) | 0.225 |
| Prior ECMO | 5 (4%) | 1 (8%) | 4 (3%) | 0.402 |
| Prior Impella | 3 (2%) | 0 (0%) | 3 (2%) | 1 |
| Prior extra-VAD implantation | 23 (17%) | 1 (8%) | 22 (18%) | 0.697 |
| Redo-surgery | 39 (29%) | 2 (15%) | 37 (30%) | 0.346 |
| Operative time (min), median (IQR) | 395 (333–469) | 338 (320–358) | 407 (334–474) | 0.021 |
| Extracorporeal circulation time (min), median (IQR) | 141 (101–167) | 104 (97–116) | 143 (101–173) | 0.0195 |
| Approach | 1 | |||
| Median | 133 (99%) | 13 (100%) | 120 (98%) | |
| Lateral | 2 (1%) | 0 (0%) | 2 (2%) | |
| Outflow position | 1 | |||
| Ascending aorta | 133 (99%) | 13 (100%) | 120 (98%) | |
| Descending aorta | 2 (1%) | 0 (0%) | 2 (2%) | |
| Implanted devices | 0.586 | |||
| DuraHeart | 20 (15%) | 2 (15%) | 10 (8%) | |
| EVAHEART | 40 (30%) | 2(15%) | 28 (23%) | |
| Jarvik 2000 | 36 (27%) | 1 (8%) | 22 (18%) | |
| HeartMate II | 71 (53%) | 6 (46%) | 50 (41%) | |
| HeartMate 3 | 8 (6%) | 2 (15%) | 6 (5%) | |
| HVAD | 9 (7%) | 0 (0%) | 6 (5%) | |
| Additional valve procedures | 0.96 | |||
| Aortic valve surgery | 8 (6%) | 2 (15%) | 6 (5%) | |
| Mitral valve surgery | 15 (11%) | 2 (15%) | 13 (11%) | |
| Tricuspid valve surgery | 28 (21%) | 5 (38%) | 23 (19%) | |
| Aortic- and tricuspid valve surgery | 2 (1%) | 1 (8%) | 1 (1%) | |
| Mitral- and tricuspid valve surgery | 16 (12%) | 0 (0%) | 16 (13%) | |
| Aortic- and mitral- and tricuspid valve surgery | 2 (1%) | 0 (0%) | 2 (2%) |
| Variable | All | Recovery group, | Non-recovery group, |
|
|---|---|---|---|---|
| Transthoracic echocardiography, median (IQR) | ||||
| LVEF (%) | 15 (11–21) | 21 (13–23) | 15 (11–21) | 0.19 |
| FS (%) | 7 (5–10) | 10 (6.8–11) | 7 (5.0–10) | 0.099 |
| LVDd (mm) | 75 (65–81) | 72 (61–73) | 76 (66–82) | 0.028 |
| LVDs (mm) | 69 (60–76) | 64 (56–67) | 70 (60–76) | 0.021 |
| IVS (mm) | 7 (6–8) | 7 (6–7) | 7 (6–8) | 0.3 |
| LVPW (mm) | 7 (6–8) | 7 (7–8) | 7 (6–8) | 0.8 |
| LVEDV (ml) | 298 (218–362) | 272 (185–281) | 298 (224–364) | 0.039 |
| LVESV (ml) | 243 (180–307) | 213 (143–237) | 255 (182–314) | 0.019 |
| LVSV (ml) | 43 (32–63) | 41(33–65) | 43 (32–60) | 0.89 |
| LA (mm) | 47 (41–55) | 44 (39–46) | 48 (41–56) | 0.027 |
| LVM (g) | 224 (172–313) | 200 (157–230) | 238 (174–322) | 0.096 |
| AR, grade | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.51 |
| MR, grade | 2 (1–2) | 1 (1–2) | 2 (1–2) | 0.36 |
| TR, grade | 1 (1–2) | 1 (1–1) | 1 (1–2) | 0.42 |
| RVSP (mmHg) | 38 (28–51) | 29 (21–42) | 38 (28–52) | 0.047 |
| Swan-ganz catheterization, median (IQR) | ||||
| Mean right atrium (mmHg) | 8 (5–12) | 13 (5–16) | 7 (5–11) | 0.23 |
| Systolic right ventricle (mmHg) | 36 (27–46) | 41 (28–46) | 36 (27–46) | 0.82 |
| Diastolic right ventricle (mmHg) | 9 (6–13) | 9 (3–14) | 9 (6–12) | 0.9 |
| Mean pulmonary capillary wedge pressure (mmHg) | 20 (13–26) | 25 (21–30) | 20 (12–25) | 0.16 |
| Systolic pulmonary artery (mmHg) | 38 (25–48) | 42 (33–45) | 38 (25–50) | 0.9 |
| Diastolic pulmonary artery (mmHg) | 20 (14–26) | 23 (18–31) | 19 (14–25) | 0.35 |
| Mean pulmonary artery (mmHg) | 27 (18–36) | 32 (24–36) | 27 (18–36) | 0.54 |
| Cardiac index (l/min/m2) | 1.9 (1.56–2.24) | 1.8 (1.16–2.45) | 1.9 (1.57–2.21) | 0.5 |
| Cardiac output (l/min) | 3.14 (2.65–3.76) | 3.05 (2.03–4.03) | 3.14 (2.70–3.74) | 0.57 |
| Pulmonary vascular resistance, wood | 2.24 (1.42–3.33) | 2.14 (1.10–2.91) | 2.24 (1.44–3.53) | 0.34 |
| Right ventricular stroke work index (g m/beat/kg) | 6.02 (3.82–8.21) | 3.70 (3.18–5.49) | 6.16 (3.93–8.21) | 0.23 |
| Pulmonary artery pulsatility index | 2.32 (1.27–3.5) | 1.11 (1.02–2.13) | 2.48 (1.44–3.50) | 0.16 |
| Right atrial pressure/pulmonary capillary wedge pressure, ratio | 0.43 (0.29–0.59) | 0.50 (0.25–0.55) | 0.41 (0.29–0.60) | 0.88 |
| Recovery group, mean ± SD | Non-recovery group, mean ± SD |
| |
|---|---|---|---|
| (A) Cardiac index (l/min/m2) | |||
| Pre-LVAD implantation | 1.82 ± 0.72 | 1.98 ± 0.52 | 0.42 |
| Post-LVAD implantation at 1 month | 2.55 ± 0.37 | 2.53 ± 0.65 | 0.93 |
| (B) Mean pulmonary capillary wedge pressure (mmHg) | |||
| Pre-LVAD implantation | 23 ± 12 | 19 ± 9 | 0.20 |
| Post-LVAD implantation at 1 month | 7 ± 3 | 9 ± 5 | 0.23 |
| (C) Mean pulmonary artery pressure (mmHg) | |||
| Pre-LVAD implantation | 29 ± 13 | 28 ± 11 | 0.69 |
| Post-LVAD implantation at 1 month | 16 ± 3 | 17 ± 6 | 0.57 |
| (D) Mean right atrial pressure (mmHg) | |||
| Pre-LVAD implantation | 11 ± 7 | 8 ± 5 | 0.12 |
| Post-LVAD implantation at 1 month | 7 ± 3 | 7 ± 4 | 0.86 |
| (E) Right atrial pressure/pulmonary capillary wedge pressure ratio | |||
| Pre-LVAD implantation | 0.42 ± 0.24 | 0.52 ± 0.41 | 0.48 |
| Post-LVAD implantation at 1 month | 1.11 ± 0.44 | 1.10 ± 0.93 | 0.95 |
| LVEF (%) | Recovery group, | Non-recovery group, |
| LVDd (mm) | Recovery group, | Non-recovery group, |
| LVDs (mm) | Recovery group, | Non-Recovery group, |
| |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-LVAD support | 18 ± 6 | 16 ± 7 | 0.32 | 67 ± 9 | 75 ± 13 | 0.044 | 61 ± 9 | 69 ± 13 | 0.030 | |||
| Post-LVAD support at 1 month | 27 ± 13 | 16 ± 9 | <0.005 | 55 ± 11 | 63 ± 12 | 0.024 | 48 ± 12 | 59 ± 12 | <0.005 | |||
| Post-LVAD support at 6 months | 43 ± 10 | 18 ± 10 | <0.005 | 52 ± 10 | 64 ± 14 | <0.005 | 39 ± 10 | 59 ± 15 | <0.005 | |||
| Post-LVAD support at 1 year | 49 ± 10 | 16 ± 10 | <0.005 | 53 ± 6 | 64 ± 14 | 0.016 | 39 ± 6 | 59 ± 15 | <0.005 | |||
| Post-LVAD support at 2 years | 51 ± 5 | 16 ± 12 | <0.005 | 54 ± 6 | 65 ± 15 | 0.030 | 40 ± 4 | 61 ± 16 | <0.005 |
| Variables | OR | 95% CI |
| OR | 95% CI |
|
|---|---|---|---|---|---|---|
| Age at LVAD implantation (years) | 0.97 | 0.92–1.02 | 0.204 | |||
| Male gender | 0.99 | 0.26–3.86 | 0.99 | |||
| Body mass index (kg/m2) | 1.24 | 1.04–1.48 | 0.016 | |||
| QRS before LVAD implantation <0.12 s | 6.12 | 1.27–29.60 | 0.024 | |||
| Brain natriuretic peptide (pg/ml) | 0.998 | 0.99–1.00 | 0.0083 | |||
| Left ventricular diastolic diameter before LVAD implantation (mm) | 0.95 | 0.90–0.99 | 0.043 | |||
| INTERMACS level | 0.48 | 0.17–1.36 | 0.166 | |||
| Time between first HF and LVAD implantation (months) | 0.97 | 0.95–0.99 | 0.0024 | 0.97 | 0.95–0.99 | 0.0075 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Cardiac Structural Anomalies and Repair · Cardiac Arrest and Resuscitation
INTRODUCTION
Continuous flow left ventricular assist device (cf-LVAD) therapy successfully improves survival, symptoms, exercise tolerance and quality of life in patients with advanced heart failure (HF) and long-term mechanical circulatory support (MCS) using left ventricular assist device (LVAD) has increasingly become a treatment option, especially as life-saving procedure for drug-refractory end-stage HF with severe LV dysfunction [1, 2]. The latest Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) report shows an overall survival rate of 84% at 1 year after isolated LVAD implantation [3]. The EUROMACS data show a lower 1-year survival rate of only 70% [4]. LVAD support reduces rehospitalization due to HF, but in some cases may lead to ventricular assist device (VAD)-related complications, including infection, stroke, intestinal bleeding, right HF and VAD thrombosis, which may require intensive care treatment and invasive surgical therapy [2, 5, 6]. Treatment strategies using LVAD support are complex and associated with adverse effects that impose a significant burden on patients and caregivers and negatively affect resource utilization and overall public health [3–6].
cf-LVAD is used either as bridge to transplantation or destination therapy; it is well-known that some patients (1–2%) reach a bridge to recovery phase allowing cf-LVAD explantation [7]. The pathophysiology and mechanisms of LV myocardial recovery secondary to cf-LVAD support are neither well understood nor thoroughly explored; however, it is reported that LV unloading can boost LV reverse remodelling and lead to improvement of LV function in bridge to recovery patients [8–13].
Although the management of cf-LVAD explantation is still a debatable topic, cf-LVAD explantation should be positively considered when the haemodynamic status allows to do so after cf-LVD implantation. LVAD explantation seems meaningful in recovered patients, because it allows for the elimination of VAD-associated adverse events. Previously published case series supported cf-LVAD explantation in patients with myocardial recovery and showed excellent survival and outcomes at short-term follow-up [14, 15]. However, cf-VAD explantation in recovered patients is still controversial since it remains unclear whether recovery of heart function will be maintained [16].
This study aimed to summarize our cf-LVAD experiences and analyse the predictors for successful device explantation in patients with non-ischaemic dilated cardiomyopathy (DCM) with cf-LVAD.
MATERIALS AND METHODS
Data collection and follow-up
This single-centre study was approved by the institutional Ethics Committee of the University of Tokyo [3031-(4)]. We included all the patients from our institutional database qualifying for cf-LVAD implantation. All patients entered in the study period were offered participation in the study. Clinical decisions were made during interdisciplinary heart team conferences consisting of cardiologists, cardiac surgeons, perfusionists, cardio-anesthesiologists and VAD coordinators. As a bridge to transplant, a total of 191 patients were implanted with durable LVADs at our centre between November 2007 and April 2020 (Supplementary Material 1). Patients younger than 18 years of age (n = 7) and those with destination therapy strategy (n = 2) were excluded. Finally, a total of 135 non-ischaemic DCM patients were retrospectively included; all of whom were diagnosed with end-stage HF based on haemodynamic examination. A diagnosis of non-ischaemic DCM was obtained by myocardial biopsy histology. The devices included DuraHeart (Terumo Heart, Ann Arbor, MI, USA), EVAHEART (Sun Medical Technology Research Corp, Nagano, Japan), Jarvik 2000 (Jarvik Heart, New York, NY), HVAD (Medtronic, Minneapolis, USA), HeartMate II (Abbott Medical, Abbott Park, USA) and HeartMate 3 (Abbott Medical, Abbott Park, USA) devices. Demographics and clinical data before LVAD implantation included invasive pressures examination by right heart catheterization (RHC). As our standard strategy, clinical status was classified by INTERMACS levels, and patients with a diagnosis of level 1 (cardiogenic shock requiring temporary MCS) underwent Nipro paracorporeal pulsatile LVAD (Nipro-LVAD; Nipro, Osaka, Japan) implantation or Impella (Abiomed, Danvers, MA, USA) as a bridge to long-term MCS. We also collected imaging, laboratory values and cardiopulmonary exercise testing and surgical data. Transthoracic echocardiography (TTE) was regularly performed at 1, 6 and 12 months after LVAD implantation, and subsequently every 6 months. The clinical follow-up was closed on 31 May 2021, when the last enrolled patient had completed 1 year of follow-up.
Standardized weaning protocol in our institution to evaluate ventricular assist device explant candidates
All potential candidates for VAD explantation were examined according to our three-phased institutional weaning protocol: selection of weaning candidates at clinic visit (first phase), LVAD speed reduction and saline loading test (second phase) and intraoperative outflow graft occlusion test (third phase). Workflow and details of this protocol are depicted in Supplementary Material 2 [17].
Left ventricular assist device explantation surgery approach
Our standardized surgical LVAD explantation strategy consists of complete device removal (a remaining short segment of the outflow graft is oversewn) and LV apical linear closure. Our surgical strategy is summarized in a previously published case series [17].
Follow-up
In the follow-up period, daily quality of life and functional status were assessed thoroughly. Finally, TTE and RHC were repeated to ensure sustained myocardial recovery. After cf-LVAD explantation, clinical follow-up and TTE were performed at 1, 6 and 12 months and yearly thereafter. Anti-coagulation was used during the first 6 months after LVAD explantation, and only aspirin was continued for life in patients after LVAD removal. A ‘successful’ cf-LVAD explantation was defined as the freedom from rehospitalization for HF and cardiovascular death during the follow-up period. Re-hospitalization for HF was defined as new-onset or worsening signs and symptoms of HF that require urgent therapy and hospitalization. The first HF event was defined as exacerbation of HF requiring intensive treatment by hospitalization.
Statistical analysis
Results are expressed as a mean ± standard deviation or as median plus 25th–75th percentile interquartile range for continuous variables, and frequency and percentage for categorical variables where appropriate. Univariable comparisons were performed with Student’s unpaired t-test for continuous normally distributed data. Mann–Whitney U-test was used for comparisons of non-parametric data and Fisher’s exact test for categorical variables. The data in paired 2 groups were analysed using the signed Wilcoxon test. The paired Freedman test was used for comparisons of non-parametric data among paired 3 groups. Predictors of success following cf-LVAD explantation was evaluated using logistic regression analysis, and the results were expressed as odds ratios with 95% confidence intervals. Candidate covariates were chosen based on previous medical knowledge. Covariates were included via stepwise regression analysis using a probability for stepwise entry of 0.05. Receiver operating characteristic curves were plotted, and the area under the curves calculated to assess the optimal cutoff values for factors that predicted cf-LVAD explanation during LVAD support. The sensitivity and specificity values also were calculated.
Data for survival and freedom from cardiac events were derived using a Kaplan–Meier method; comparisons were made by a log-rank test. A P-value of <0.05 was considered statistically significant, and all reported P-values are two-sided. All statistical analyses were performed using R software (The R Project for Statistical Computing; The R Foundation).
RESULTS
Enrolled patients—cardiac recovery versus non-recovery
After the exclusion of non-DCM patients (ischaemic cardiomyopathy, n = 17; dilated hypertrophic cardiomyopathy, n = 16; drug-induced cardiomyopathy, n = 5; arrhythmogenic right ventricular cardiomyopathy, n = 3; sarcoidosis, n = 3; Endocardial fibrosis, n = 2, adult congenital, n = 2; valvular cardiomyopathy, n = 1), a total of 135 non-ischaemic DCM patients (n = 133, implantation in our hospital, and n = 2, in other institutions) were finally enrolled in this study (Supplementary Material 1). Of those, 13 patients (recovery group) underwent cf-LVAD explantation following myocardial recovery after a median of 10 months [interquartile range (IQR); 4–15 months] of cf-LVAD support. Twelve patients completed our standardized study protocol to test LVAD system explantation and proceeded to elective cf-LVAD explantation (Supplementary Material 2). One patient had thrombosis-related pump dysfunction 2 months after cf-LVAD implantation. Fortunately, left ventricular ejection fraction (LVEF) improved to within normal range, and urgent cf-LVAD explantation was performed without the evaluation.
Perioperative, mid-term outcomes in cf-LVAD explanted patients
Perioperative outcomes are summarized in Table 1. None of the patients required temporary MCS such as extracorporeal membrane oxygenation (ECMO) or intra-aortic balloon pump (IABP) after cf-LVAD explanation, except 1 patient, who used IABP for potential haemodynamic deterioration.
In the perioperative period, no complications, including cerebrovascular accident, HF, bleeding and infection, occurred and all 13 patients survived and were discharged home. The median stay in the intensive care unit was 4 days (IQR; 3–4 days) and median total hospital stay was 30 days (IQR; 23–36 days).
During a median follow-up of 30 months (IQR; 18–56 months, range; 10–106 months), there was no cardiac- or non-cardiac-related death (Table 1). None of the patients required rehospitalization for recurrent left or new onset right HF, or for invasive treatment such as MCS and heart transplantation. Anti-coagulation therapy was stopped 6 months after cf-LVAD explantation in the absence of a specific medical indication to continue it, and no anticoagulation-associated complication occurred during the follow-up in our study cohort (Table 1). Overall survival after cf-LVAD explantation was 100% during the study period (a median follow-up of 30 months). Patients remained in NYHA functional class I with ongoing medical management (i.e. β-blocker and angiotensin-converting enzyme inhibitor or angiotensin receptor blocker).
Baseline characteristics and outcomes at continuous flow left ventricular assist device implantation
Demographic and clinical features are shown in Table 2. Baseline characteristics were similar between the recovery group and the non-recovery group, except that the recovery group was more likely to have a higher body mass index (BMI) and a shorter time between first HF event and cf-LVAD implantation. None of the recovery group had cardiac resynchronization therapy with defibrillator (CRTD) before cf-LVAD implantation (P < 0.005). Beta-blocker dose at cf-LVAD implantation was significantly lower in the recovery group than in the non-recovery group (P = 0.011).
The median time from the first HF diagnosis to cf-LVAD implantation was 4 months (IQR; 2–7 months) in the recovery group and 77 months (IQR; 43–132 months) in the non-recovery group (P < 0.005). On ECG, QRS duration was shorter in the recovery group than in the non-recovery group (P = 0.043), and QRS <0.12 s was noted in 9 (69%) recovery patients. At the time of cf-LVAD implantation, distribution of INTERMACS status, the use of prior MCS, types of implanted cf-LVAD and concomitant surgical procedures were not significantly different between the 2 groups. TTE and RHC were performed to assess haemodynamic status before cf-LVAD implantation (Table 3). The parameters representing left ventricular dimension, including left ventricular end-diastolic diameter (LVDd), left ventricular end-systolic diameter (LVDs), left ventricular end-diastolic volume and LVEDS, were significantly larger in the non-recovery group than in the recovery group, resulting in the stroke volume not being statistically different. In addition, left atrial diameter was significantly larger in the non-recovery group. Other variables, such as LVEF and the grade of aortic regurgitation, mitral regurgitation and tricuspid regurgitation, were not significantly different between the 2 groups.
Haemodynamic response following LV unloading
Haemodynamic parameters using RHC were compared between pre- and 1-month post-LVAD implantation. The differences in all parameters related to intracardiac pressure and cardiac output between the 2 groups before cf-LVAD implantation did not show statistical significance. Data are shown in Table 3. These values including pulmonary artery pressure, right atrial pressure, pulmonary capillary wedge pressure and cardiac index demonstrated a trend to improve 1-month post-LVAD implantation compared to pre-LVAD implantation (Fig. 1 and Table 4). This trend was observed in both the recovery group and the non-recovery group, and the values post-LVAD implantation were not significantly different between the 2 groups (Fig. 1 and Table 4).
Comparison of haemodynamic parameters between pre- and 1-month post-left ventricular assist device implantation.
Comparison of echocardiographic parameters in the recovery group versus the non-recovery group at long-term follow-up
Echocardiographic parameters (LVEF, LVDs and LVDd) of the 2 groups are depicted in Fig. 2 and Table 5. In the recovery group, the echocardiographic values after cf-LVAD explantation were also included in the calculation. LVEF improved within 1 month in the recovery group, compared to the non-recovery group, and the difference was statistically significant (27 ± 13 vs 16 ± 9, respectively, p < 0.005). Furthermore, the LVEF continued to improve over the following months, and the mean LVEF in the recovery group exceeded 40% at 6 months (Fig. 2 and Table 5). During the 2-year follow-up, this statistically significant difference was maintained at any given timepoint. The LV-diastolic and systolic diameters were significantly decreased after LV unloading using cf-LVAD in both 2 groups (Fig. 2 and Table 5). Moreover, the decrease in LVDd and LVDs was maintained in the recovery group compared to the non-recovery group, with a statistically significant difference at 6 months, 1 year and 2 years.
Comparison of echocardiographic parameters between the recovery and non-recovery groups.
Predictors for left ventricular assist device explantation
Univariable and multivariable logistic regression analyses were performed to explore predictors of successful long-term LV reverse remodelling after cf-LVAD explantation. Pronounced associations were found between cf-LVAD explantation and BMI, ECG-QRS <0.12 ms, the value of B-type natriuretic peptide (BNP), LVDd at cf-LVAD implantation and the time interval between the first HF events and cf-LVAD implantation in the univariable logistic regression analysis (all p < 0.005, Table 5). Multivariable logistic regression analysis showed that the time interval between the first HF events and cf-LVAD implantation was an independent predictor for cf-LVAD explantation (odds ratio 0.97; 95% confidence interval 0.95–0.99, p = 0.0087, Table 6) The receiver operating characteristic curve analysis revealed that the optimal cutoff value of the time interval between the first HF events and cf-LVAD implantation to predict cf-LVAD explantation was 7 months, and the area under the curve was 0.859; this cutoff value had a sensitivity of 91.0% and specificity of 84.6% (Supplementary Material 3).
DISCUSSION
In our study, we showed an extremely satisfying long-term survival rate (100% at median 3-year follow-up [IQR; 1–4 years]) and freedom from cardiac events (100% during the same period of follow-up) after cf-LVAD explantation in non-ischaemic DCM patients using our weaning protocol. Previous reports show that cardiac and physical functional capacity in patients with cf-LVAD explantation was well maintained compared to those with cf-LVAD therapy or heart transplantation [14, 17]. In the patients completing weaning protocol successfully, cf-LVAD explantation is feasible and an excellent long-term cardiac event free-survival seems to be achieved [18]. As increased mortality in on-going VAD patients is due to VAD-related complications, we believe that cf-LVAD explantation should be considered if possible.
Pan et al. [19] identified some predictors of myocardial recovery after LVAD implantation, which included younger age, female sex, lower BMI, non-ischaemic cause and short interval of HF before LVAD implantation. In our study, multivariate Cox regression analysis identified short interval between the first HF event and cf-LVAD implantation as the predictor with statistical significance (Table 6). In the present study, the median interval was 4 months (IQR; 2–7 months) in 13 patients with myocardial recovery. In our opinion, LV unloading with cf-LVAD support should be started as soon as possible in the event that HF could not be controlled with guideline direct medical therapy (GDMT) or CRTD implantation. However, currently, it may be difficult to implement this strategy since there is no supporting evidence and LVAD-related complications significantly increase morbidity and mortality.
In our study, 7 patients (54%) needed IABP and 1 patient (7.7%) ECMO before cf-LVAD implantation, who eventually underwent LVAD explantation. The severity of heart failure patients before LVAD implantation seems to be similar to that in other studies (14.15). Although these patients experienced acute haemodynamic deterioration, they may have had myocardial recovery during temporary MCS. This is because LV unloading with MCS is not only effective but allows for patients to be initiated on GDMT. Various temporary MCS strategies, such as IABP, ECMO and Impella, have been introduced. Of those, a percutaneous system with Impella 5.5 (Abiomed, Inc., Danvers, Massachusetts, USA) gained the attention of many physicians after its strong support of the circulatory system was observed [20]. Impella may be used as first choice for bridge to recovery since it can perform optimal LV unloading, reducing LV end-diastolic pressure and wall tension leading to a decrease in LV work and myocardial oxygen demand [20]. Therefore, we believe that successful myocardial recovery requires timeous and sufficient LV unloading and GDMT introduction in non-ischaemic DCM patients.
LVEF, LVEDD and LVESD significantly improved at 30 days compared with pre-LVAD (21 vs 27%, 72 vs 55 mm and 64 vs 46 mm, respectively; all median values, P < 0.05). This improvement in echocardiographic parameters reflecting myocardial recovery emerged in our patients within 30 days after LVAD implantation, compared to non-recovery patients, with the trend of improvement becoming more significant at 6 months (Fig. 2). Therefore, it would be reasonable to consider following up for further evaluation the patient in 6 months of the LVAD implantation as it would be useful to identify the explant candidate. In our study, 1 patient underwent LVAD explantation at 2 months following LVAD dysfunction due to pump thrombosis. Urgent explantation was successfully performed since the patient fortunately achieved some myocardial recovery within 1 month after LVAD implantation. The other 12 patients completed our weaning protocol in a stable condition.
Univariate Cox regression analysis showed that QRS duration, LVDd and BNP at LVAD implantation were significant predictors for successful explantation. None of the patients with successful cf-LVAD explantation had CRTD at implantation. In addition to echocardiographic parameters, ECG and the BNP value at LVAD implantation may also indicate a possibility of myocardial recovery. These markers may be associated with the severity of myocardial fibrosis [21]. Future prospective studies are needed to yield reliable markers for myocardial recovery during LVAD support.
There is no consensus on the optimal surgical strategy regarding LVAD explantation and management of postoperative antiplatelet and anticoagulant therapy. Certainly, surgical cf-LVAD removal itself may be associated with a risk of recurrent cardiac failure due to invasive redo open heart surgery. Therefore, as less invasive deactivation techniques, simplified surgical procedures ranging from driveline disruption to partial VAD explantation by thoracotomy with inflow occlusion using mechanical plugs have been reported [22]. In particular, this occlusion method mechanical using plugs seems to preserve cardiac geometry at the time of cf-LVAD removal and make easier the surgical approach [23–26]. However, the long-term safety and efficacy of these procedures are unclear since most studies have focused on short-term outcomes in a small study cohort. Additionally, anticoagulation or antiplatelet therapies may need to be continued since there is a risk of foreign material plug associated thrombosis [22]. Therefore, the life-threating risk of bleeding remains despite of the absence of LVAD support. In our study, among 13 patients performing cf-LVAD explantation, 7 (54%) patients had intracerebral bleeding (n = 3) or thrombosis (n = 4) during cf-LVAD support. However, no further bleeding or thrombotic complications occurred in patients after cf-LVAD explantation during the follow-up period.
Most importantly there is always a risk for recurrent HF, even if primary explantation was successful. Fortunately, myocardial recovery was preserved throughout the complete follow-up period (Fig. 2 and Table 5). All patients were treated with β-blocker and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker during the study period. This GDMT is believed to be mandatory to preserve LV function after myocardial recovery [27]. Recently, sodium glucose cotransport-2 as heart failure therapy has been increasingly used with satisfying results [28]. Therefore, the effect of sodium glucose cotransport-2 use post-LVAD explantation should also be adequately studied.
Limitations
This study has some limitations. This is a retrospective, single-centre observational study with a limited number of patients. Second, only non-ischaemic DCM patients were enrolled and analysed, but some DCM types such as DCM-like phenotypes may be included. Moreover, our TTE data were evaluated by experienced cardiologists, but not adjudicated by an external core lab. Thus, conclusions from our study should be taken with caution until confirmed by the currently ongoing multicentre clinical trial (ClinicalTrials.gov identifier NCT number: NCT03238690).
Supplementary Material
ivae091_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gummert JF , Haverich A, Schmitto JD et al Permanent implantable cardiac support systems. Dtsch Arztebl Int 2019;116:843–8.31931951 10.3238/arztebl.2019.0843 PMC 6970315 · doi ↗ · pubmed ↗
- 2Schramm R , Morshuis M, Schoenbrodt M, Boergermann J, Hakim-Meibodi K, Hata M et al Current perspectives on mechanical circulatory support. Eur J Cardiothorac Surg 2019;55:i 31–i 37.30608535 10.1093/ejcts/ezy 444PMC 6526098 · doi ↗ · pubmed ↗
- 3Kirklin JK , Pagani FD, Kormos RL, Stevenson LW, Blume ED, Myers SL et al Eighth annual INTERMACS report: special focus on framing the impact of adverse events. J Heart Lung Transplant 2017;36:1080–6.28942782 10.1016/j.healun.2017.07.005 · doi ↗ · pubmed ↗
- 4de By TMMH , Schweiger M, Hussain H, Amodeo A, Martens T, Bogers AJJC et al The European Registry for Patients with Mechanical Circulatory Support of the European Association for Cardio-Thoracic Surgery: third report. Eur J Cardiothorac Surg 2022;62:ezac 032.35758622 10.1093/ejcts/ezac 355 · doi ↗ · pubmed ↗
- 5Gyoten T , Rojas SV, Fox H, Deutsch M-A, Ruiz-Cano M, Hakim-Meibodi K et al The Heart Ware Ventricular Assist Device (HVAD): a single institutional 10-year experience. Thorac Cardiovasc Surg 2022;70:482–92.35235989 10.1055/s-0042-1742779 · doi ↗ · pubmed ↗
- 6Börgermann J , Gummert JF, Schramm R. Heart failure in the spotlight. Interact Cardio Vasc Thorac Surg 2018;27:795–6.30496468 10.1093/icvts/ivy 325 · doi ↗ · pubmed ↗
- 7Wever-Pinzon O , Drakos SG, Mc Kellar SH, Horne BD, Caine WT, Kfoury AG et al Cardiac recovery during long-term left ventricular assist device support. J Am Coll Cardiol. 2016;68:1540–53.27687196 10.1016/j.jacc.2016.07.743 · doi ↗ · pubmed ↗
- 8Hall JL , Fermin DR, Birks EJ, Barton PJR, Slaughter M, Eckman P et al Clinical, molecular, and genomic changes in response to a left ventricular assist device. J Am Coll Cardiol 2011;57:641–52.21292124 10.1016/j.jacc.2010.11.010PMC 3381801 · doi ↗ · pubmed ↗