Neurosarcocystosis in Patient with HIV-Induced Immunodeficiency
Tonje Skarpengland, Anders A. Tveita, Christopher F. Berntsen, Erik. E. Christensen, Magnhild E. Macpherson, Birgitte Stiksrud, Nils O. Hermansen, Pitt Niehusmann, Tine S. Oldereid, Espen Stjernstrøm, Hanne Brekke, Henrik V. Nielsen, Frank O.D. Pettersen

TL;DR
This paper reports a rare case of a Sarcocystis infection in the brain of an HIV patient in Norway.
Contribution
The novelty is the documentation of central nervous system infection by S. nesbitti in a human with HIV.
Findings
A human case of central nervous system sarcocystosis was identified in Norway.
The infection was caused by Sarcocystis nesbitti parasites.
The patient had HIV-induced immunodeficiency.
Abstract
Sarcocystis is a genus of protozoan parasites that can infect various vertebrates. In humans, Sarcocystis infection usually is asymptomatic but might manifest as a mild gastroenteritis or extraintestinal myositis. We report a case of human central nervous system infection in Norway caused by S. nesbitti parasites.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
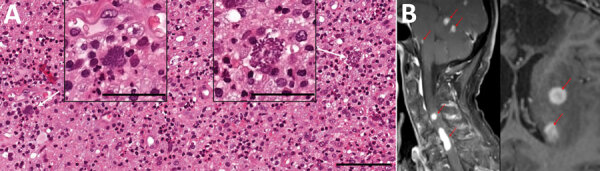 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsToxoplasma gondii Research Studies · Parasitic Infections and Diagnostics · Pneumocystis jirovecii pneumonia detection and treatment
The genus Sarcocystis consists of apicomplexan parasites, ≈200 species of which can infect reptiles, birds, and mammals; however, few species are zoonotic (1). Humans are definitive hosts of S. hominis, S. suihominis, and S. heydorni, shedding oocysts after ingestion of undercooked meat from intermediate hosts containing tissue cysts (1). Gastrointestinal infection is asymptomatic or causes a mild, self-limiting gastroenteritis (2). Human muscular sarcocystosis is a rare clinical syndrome associated with S. nesbitti infection mostly documented in Malaysia (2). The natural reservoirs of S. nesbitti parasites are probably reptiles, particularly snakes in Southeast Asia and Australia (3,4). Intermediate hosts, including humans, might develop tissue sarcocystosis after ingesting S. nesbitti sporocysts from fecally contaminated food or water. In Thailand, the prevalence of intestinal sarcocystosis is 7.0%–23.2% (5,6), but data regarding tissue sarcocystosis and S. nesbitti infection are scarce. We report a human case of S. nesbitti central nervous system infection in Norway.
The patient, a White male in his 70s, had lived in Norway for ≈40 years and visited Thailand for several months a year for 10 years. While in southern Thailand, he experienced increasing back pain and acute diplopia, aphasia, unilateral hemiparesis, and urinary and fecal incontinence. Imaging conducted in a clinic in Thailand revealed multiple brain lesions, and he returned to Norway for further investigations.
Upon the patient’s hospital admission in Norway, initial laboratory workup revealed an undiagnosed HIV infection (viral load 50,000 copies/mL, CD4+ T-cell count 116 cells/mm^3^). Magnetic resonance imaging showed numerous cortical and subcortical contrast-enhancing lesions in both cerebral hemispheres, along with multiple cerebellar, cervical, and thoracic spinal cord lesions (Figure). We noted hemorrhagic components and substantial perilesional edema (Figure). 18F-fluorodeoxyglucose (FDG) positron emission tomography–computed tomography demonstrated intense focal FDG uptake corresponding to areas of contrast enhancement found on magnetic resonance imaging. Apart from a diffusely increased signal in gluteal muscles, we noted no abnormal FDG uptake outside the central nervous system (CNS). The overall assessment suggested metastatic cancer, with opportunistic infection as a differential diagnosis.
Cerebrospinal fluid (CSF) analysis showed an unremarkable leucocyte count (<4 × 10^6^ cells/L), but increased protein level (1.8 g/L) and albumin and IgG indices. Serologic test results were positive for Toxoplasma gondii IgG and negative for IgM. Blood and CSF were negative for T. gondii DNA. We detected asymptomatic reactivation of Epstein-Barr virus (EBV) and cytomegalovirus in blood. Results of additional microbiologic diagnostic analyses of other viruses, bacteria, fungi, and parasites (e.g., tuberculosis interferon-γ release assay and serologic and molecular testing of blood and CSF) were negative.
Histological examination of brain tissue revealed no signs of malignancy but indicated lymphohistiocytic infiltrates and singular structures resembling T. gondii bradyzoites (Figure). However, T. gondii immunohistochemical testing was inconclusive, and results for 2 different T. gondii–specific PCR assays were negative. Brain tissue PCR results were negative for herpes simplex virus 1 and 2, varicella zoster virus, cytomegalovirus, JC virus, 16S rDNA, internal transcribed spacer 2, and D1D2 fungal DNA. EBV PCR results were positive, but in situ hybridization displayed EBV-positive cells in a minute proportion of infiltrating lymphocytes, compatible with unspecific reactivity. We sent brain tissue and CSF to Statens Serum Institut (Copenhagen, Denmark) for metabarcoding analyses based on 16S and 18S DNA PCR combined with next-generation sequencing (7).
Faced with the presence of multiple space-occupying CNS lesions and evolving neurologic symptoms in the patient, we initiated treatment with dexamethasone pending further diagnostic workup. We started the patient on antiretroviral therapy, and after histologic assessment of the brain biopsy, we commenced treatment with high-dose trimethoprim/sulfamethoxazole (5/25 mg/kg × 2/d), because toxoplasmosis was considered the most probable diagnosis. The metabarcoding analyses of brain tissue (but not CSF) yielded a 380-bp consensus sequence of the 18S rRNA gene with 100% similarity to a published S. nesbitti sequence (genomic DNA containing 18S rRNA gene; GenBank accession no. HF544323.1). On the basis of metabarcoding analyses and histological findings, we made a final diagnosis of neurosarcocystosis. Sarcocystis serologic testing was not obtainable.
The treatment regimen was well-tolerated, and the patient’s clinical and radiologic condition improved substantially without signs of immune reconstitution inflammatory syndrome; however, some neurologic sequelae remained. We tapered glucocorticoids gradually and started secondary prophylaxis of trimethoprim/sulfamethoxazole.
To our knowledge, human neurosarcocystosis is not recognized as an opportunistic infection. Given the phylogenetic relationship of Sarcocystis with Toxoplasma, the patient’s condition might represent reactivation of latent sarcocystis infection resulting from HIV-induced immunodeficiency. Because of limited knowledge about the dynamics of extraintestinal sarcocystosis in immunosuppressed hosts, we cannot determine whether this condition represents a primary infection or reactivation. A detailed travel history revealed no visits to Sarcocystis-endemic hotspots such as the Pangkor or Tioman Islands of Malaysia (8).
We hypothesize that Sarcocystis spp. may cause opportunistic CNS infections in immunocompromised persons. Furthermore, neurosarcocystosis might be misdiagnosed as toxoplasmosis clinically, histopathologically, and radiologically. Because both conditions respond to high-dose trimethoprim/sulfamethoxazole, therapeutic efficacy might inadvertently support such a misdiagnosis. This case illustrates that the true prevalence and disease patterns of opportunistic pathogens are probably underestimated and that routine microbiologic workup might fail to reveal rare and unrecognized opportunistic infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rosenthal BM. Zoonotic Sarcocystis. Res Vet Sci. 2021;136:151–7. 10.1016/j.rvsc.2021.02.00833626441 · doi ↗ · pubmed ↗
- 2Fayer R, Esposito DH, Dubey JP. Human infections with Sarcocystis species. Clin Microbiol Rev. 2015;28:295–311. 10.1128/CMR.00113-1425715644 PMC 4402950 · doi ↗ · pubmed ↗
- 3Shahari S, Tengku-Idris TI, Fong MY, Lau YL. Molecular evidence of Sarcocystis nesbitti in water samples of Tioman Island, Malaysia. Parasit Vectors. 2016;9:598. 10.1186/s 13071-016-1883-927881179 PMC 5120450 · doi ↗ · pubmed ↗
- 4Wassermann M, Raisch L, Lyons JA, Natusch DJD, Richter S, Wirth M, et al. Examination of Sarcocystis spp. of giant snakes from Australia and Southeast Asia confirms presence of a known pathogen - Sarcocystis nesbitti. P Lo S One. 2017;12:e 0187984. 10.1371/journal.pone.018798429131856 PMC 5683627 · doi ↗ · pubmed ↗
- 5Wilairatana P, Radomyos P, Radomyos B, Phraevanich R, Plooksawasdi W, Chanthavanich P, et al. Intestinal sarcocystosis in Thai laborers. Southeast Asian J Trop Med Public Health. 1996;27:43–6.9031398 · pubmed ↗
- 6Tungtrongchitr A, Chiworaporn C, Praewanich R, Radomyos P, Boitano JJ. The potential usefulness of the modified Kato thick smear technique in the detection of intestinal sarcocystosis during field surveys. Southeast Asian J Trop Med Public Health. 2007;38:232–8.17539271 · pubmed ↗
- 7Hartmeyer GN, Stensvold CR, Fabricius T, Marmolin ES, Hoegh SV, Nielsen HV, et al. Plasmodium cynomolgi as cause of malaria in tourist to Southeast Asia, 2018. Emerg Infect Dis. 2019;25:1936–9. 10.3201/eid 2510.19044831538931 PMC 6759256 · doi ↗ · pubmed ↗
- 8Abubakar S, Teoh B-T, Sam S-S, Chang L-Y, Johari J, Hooi P-S, et al. Outbreak of human infection with Sarcocystis nesbitti, Malaysia, 2012. Emerg Infect Dis. 2013;19:1989–91. 10.3201/eid 1912.12053024274071 PMC 3840867 · doi ↗ · pubmed ↗