Exploring the effect of sequential antibiotic exposure in resistant Escherichia coli causing urinary tract infections: a proof of principle study
Lisa Göpel, Laura Kirchhoff, Olivia Gopleac, Leif Tüeffers, Susanne Hauswaldt, Sébastien Boutin, Jan Rupp, Dennis Nurjadi

TL;DR
This study explores if using two antibiotics in sequence can reduce resistance in E. coli causing urinary tract infections.
Contribution
The study demonstrates that sequential antibiotic exposure may improve treatment efficacy against resistant E. coli.
Findings
Sequential exposure to mecillinam followed by ciprofloxacin significantly inhibited E. coli growth.
No synergistic effect was observed between ciprofloxacin and mecillinam in checkerboard assays.
Phenotypic resistance to antibiotics was reduced through sequential treatment.
Abstract
Antimicrobial resistance development, particularly in infections such as urinary tract infections (UTIs), is a global clinical concern. The objective of this study was to determine if sequential antibiotic exposure with ciprofloxacin and mecillinam can reduce the growth of resistant clinical Escherichia coli strains, thus improving the effectiveness of antibiotic therapy. Six E. coli isolates with heterogeneous resistance to ciprofloxacin and/or mecillinam obtained from patients with UTIs were exposed to one of the antibiotics (0.75 × minimum inhibitory concentration, MIC) for 1 h. This was followed by treatment with the second antibiotic at different concentrations (0.0375/0.075/0.375/0.75 × MIC). Continuous growth measurements were conducted in order to assess the impact of sequential exposure. One representative strain was selected for intact cell counting. In addition, a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
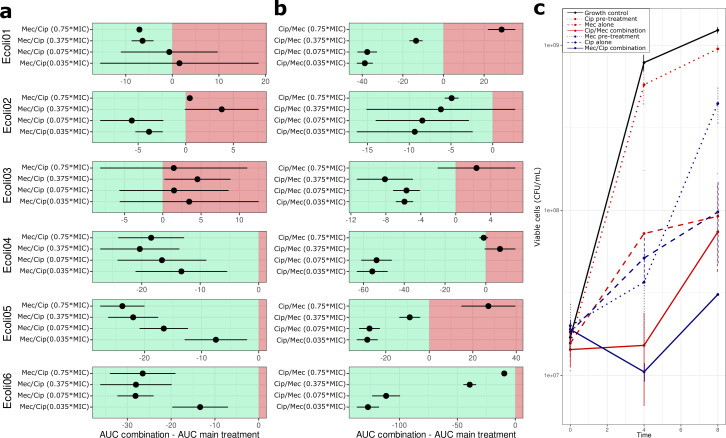 Fig 1
Fig 1| ID | MLST | Phylogroup | Serogroup | Ciprofloxacin | Mecillinam | Synergy testing | |||
|---|---|---|---|---|---|---|---|---|---|
| MIC (mg/L) | Int. | MIC (mg/L) | Int. | FICI | Int. | ||||
| Ecoli01 | ST1193 | B2 | O75:H5 | 16 | R | 1 | S | 0.553 | n. i. |
| Ecoli02 | ST162 | B1 | O76:H27 | 8 | R | 0.5 | S | 0.651 | n. i. |
| Ecoli03 | ST131 | B2 | O25:H4 | 16 | R | 1 | S | 0.999 | n. i. |
| Ecoli04 | ST127 | B2 | O6:H31 | 0.015 | S | 64 | R | 0.874 | n. i. |
| Ecoli05 | ST453 | B1 | O23:H16 | 0.25 | S | 16 | R | 0.842 | n. i. |
| Ecoli06 | ST4981 | A | O8:H17 | 32 | R | 32 | R | 0.782 | i. |
- —Deutsche Forschungsgemeinschaft (DFG)
- —Bundesministerium für Bildung und Forschung (BMBF)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Pediatric Urology and Nephrology Studies · Escherichia coli research studies
OBSERVATION
Escherichia coli is the most common pathogen responsible for both uncomplicated and complicated urinary tract infections (UTIs), which are one of the most frequent bacterial infections worldwide (1). Increasing levels of antimicrobial resistance in uropathogenic E. coli have been reported. Due to the hurdles and challenges in developing new antimicrobial agents in both the pharmaceutical industry and academia, alternative methods and strategies for preserving the efficacy of existing antibiotics are needed to anticipate the problem of antibiotic resistance (2). One such strategy is to employ an evolution-informed therapeutic approach by exposing bacterial pathogens to two antibiotics in rapid succession. This evolution-informed approach to optimized bacterial treatment is based on the assumption that selective pressure from a given substance (with or without direct antimicrobial effects) can increase susceptibility to another antibiotic substance to which the organism is resistant in conventional antimicrobial susceptibility testing. Such an approach has been described by Roemhild et al. for Pseudomonas aeruginosa to improve antibiotic efficacy and reduce resistance selection (3). However, the use of sequential antibiotic exposure as a therapeutic strategy in resistant E. coli remains largely unexplored. In this study, we sought to test our hypothesis that sequential antibiotic exposure can achieve a similar effect in E. coli, thus providing experimental evidence as a proof of concept for further clinical validation.
An initial experiment with E. coli ATCC25922 and GM2163 was conducted to investigate the effects of sequential antibiotic combinations on the growth behavior of susceptible E. coli. The antibiotic panel was selected based on commonly prescribed antibiotics for UTI, including ciprofloxacin, fosfomycin, mecillinam, and trimethoprim-sulfamethoxazole. The experiments were performed using all substances against each other in both directions as a pretreatment and main treatment resulting in 12 potential combinations (the same substance for both pretreatment and main treatment was not performed) in each direction. As illustrated in Fig. S1, sequential exposure to first mecillinam followed by ciprofloxacin resulted in enhanced bacterial growth in ATCC25922, whereas bacterial growth was reduced under the reverse drug order. The GM2163 strain demonstrated the most pronounced effect on growth behaviour when exposed to mecillinam/ciprofloxacin or ciprofloxacin/mecillinam, in comparison with all other tested combinations (Fig. S1).
Based on these initial observations, we then repeated the assay with ciprofloxacin and mecillinam for 20 randomly selected UTI-causing E. coli strains from routine microbiological diagnostics, collected in March 2023 and June 2023. Of these, six strains were chosen based on their phenotypic resistance determined by broth microdilution in M9 medium to either ciprofloxacin (minimum inhibitory concentration, MIC >0.5 mg/L; Ecoli01-03) or mecillinam (MIC >8 mg/L; Ecoli04 and 05) or both (Ecoli06) (Table 1). Isolates were further characterized using short-read genome sequencing (Methodology, see Supplementary Material), and genomic analysis revealed that all isolates were phylogenetically diverse (Table 1). Ciprofloxacin resistance was associated with non-synonymous substitution in the gyrA, parC, and parE genes, and the mecillinam resistance was associated with blaTEM-1. The presence of additional mecillinam resistance-encoding genes or mutations that have previously been identified as conferring resistance to mecillinam in E. coli was not observed (Data set S1). To rule out a synergistic effect of ciprofloxacin and mecillinam, a checkerboard assay was performed. None of the E. coli isolates tested in this study exhibited a synergistic effect for ciprofloxacin and mecillinam (Table 1).
The pretreatment duration was kept constant at 0.75 MIC for 1 h for all experiments. Based on the standard dosing intervals for pivmecillinam (200–400 mg thrice daily) and for ciprofloxacin (250–500 mg twice daily), we chose 8 h for mecillinam and 12 h for ciprofloxacin as a meaningful time course to study the growth behavior after the addition of the main treatment at 0.0375, 0.075, 0.375, and 0.75 MIC (Fig. S2). To quantify and compare the effect of sequential antibiotic exposure in E. coli strains, the growth curve data were analyzed using the Growthcurver package for R (Methodology, see Supplemental material). The area under the curve was calculated for each growth curve, and the difference in AUC (ΔAUC) between the sequential exposure and single antibiotic exposure was determined in order to summarize and compare the effect on bacterial growth (Fig. 1).
Area under the curve (AUC) analysis of sequential antibiotic exposure for six E. coli strains and BactoBox measurement for one selected E. coli strain. (a) Isolates were incubated with mecillinam (0.75 × MIC) for 1 h, followed by ciprofloxacin exposure (0.0375 × MIC; 0.075 × MIC; 0.375 × MIC; 0.75 × MIC) for 12 h. The ΔAUC was calculated for sequential exposure with antibiotics in comparison with the AUC of exposure with ciprofloxacin alone. While Ecoli01–03 exhibited considerable variation in growth, Ecoli04–06 showed an overall decrease in growth. (b) Isolates were incubated with ciprofloxacin (0.75 × MIC) for 1 h, followed by mecillinam treatment (0.0375 × MIC; 0.075 × MIC; 0.375 × MIC; 0.75 × MIC) for 8 h. The ΔAUC was calculated for sequential exposure with antibiotics with the AUC of exposure with mecillinam alone. Only Ecoli06 exhibited reduced growth under sequential exposure in all used antibiotic concentrations compared to single exposure. (c) Viable cells were quantified over an 8-h period for E. coli06 using impedance flow cytometry. A reduction in the number of viable bacteria cells was observed following sequential exposure compared with single exposure, with a notable decline occurring after 4 h. The changes in the number of viable cells at timepoints 4 h and 8 h following combined treatment were not statistically significant when compared to those observed following single exposure (P-value = 0.7 for CIP_MEC exposure, P-value = 0.12 for MEC_CIP exposure).
The exposure of mecillinam, followed by ciprofloxacin, was able to reduce the growth capacity of a ciprofloxacin-resistant and mecillinam-resistant strain Ecoli06 compared with single exposure ciprofloxacin in a dose-dependent manner (Fig. 1a). Determination of viable cells by impedance flow cytometry (BactoBox, SBT Instruments; Methodology, see Supplemental material) showed a reduction in viable bacterial cells under sequential exposure (both ciprofloxacin/mecillinam and mecillinam/ciprofloxacin combination) compared to single exposure after 4 h of incubation (Fig. 1c). Overall, exposure to mecillinam prior to ciprofloxacin exposure was able to reduce the growth capacity in 3 of 6 (50%) E. coli strains (Ecoli04, Ecoli05, and Ecoli06) in a dose-dependent manner compared to the exposure to ciprofloxacin alone. The exposure to ciprofloxacin was able to reduce the growth capacity in only two strains (Ecoli02 and Ecoli06) without dose dependency.
Our in vitro data suggested that fast sequential exposure to subinhibitory concentrations of mecillinam and ciprofloxacin on resistant clinical E. coli isolates obtained from patients with UTIs could reduce the bacterial growth of three (50%) mecillinam-resistant E. coli strains. Interestingly, the growth of bacteria was reduced only during the first 6–10 h of ciprofloxacin exposure when pre-exposed to mecillinam. The concept of sequential therapy is not completely novel and has been shown to minimize the adaption rate and inhibit the evolution of multi-drug resistance in laboratory experiments (4, 5). Recent studies suggested that sequential therapy may be more efficient than monotherapy regimens by exploiting evolutionary trade-offs, such as collateral sensitivity. This phenomenon describes the increased susceptibility to one drug due to the acquisition of resistance to another drug and has been observed in various bacterial species, including E. coli (6, 7). In 2018, it was reported that mutated mecillinam-resistant E. coli strains isolated from patients with UTIs were more likely to have collateral sensitivity toward antibiotic drugs compared with other mutated resistant strains. In contrast, mutated ciprofloxacin-resistant E. coli showed cross-resistance towards other antibiotics, such as chloramphenicol, ceftazidime, and amoxicillin (8). These observations suggest that the phenotypic susceptibility could be modulated by combining different antimicrobial drugs. The identification of robust evolutionary trade-offs may facilitate the identification of drug combinations that are more efficient when used sequentially than when administered individually (9).
Our study has limitations as it is based solely on in vitro observations and focuses only on sequential exposure of two antibiotic substances on a small number of clinical E. coli isolates. We did not include other combinations of antibiotics for sequential therapy or test other pathogenic agents causing UTIs in our study design. The primary readout in our experimental setup was optical density, which was chosen as a proxy to enable higher throughput. This approach allowed us to avoid the time-consuming nature of traditional culture and cell counting methods, thereby increasing experimental capacity. However, additional measurements beyond optical density were also performed for one strain, as shown in Fig. 1c. Despite these limitations, our data suggested that sequential antibiotic exposure can reduce the growth capacity of clinical E. coli isolate even in isolates with phenotypic resistance to either or both substances. Thus, sequential antibiotic treatment may be a promising strategy for treating infections caused by resistant E. coli and warrants further investigation.
Supplementary Material
Reviewer comments
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. 2015. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol 13:269–284. doi:10.1038/nrmicro 343225853778 PMC 4457377 · doi ↗ · pubmed ↗
- 2Paul R. 2018. State of the globe: rising antimicrobial resistance of pathogens in urinary tract infection. J Glob Infect Dis 10:117–118. doi:10.4103/jgid.jgid_104_1730166807 PMC 6100332 · doi ↗ · pubmed ↗
- 3Roemhild R, Gokhale CS, Dirksen P, Blake C, Rosenstiel P, Traulsen A, Andersson DI, Schulenburg H. 2018. Cellular hysteresis as a principle to maximize the efficacy of antibiotic therapy. Proc Natl Acad Sci USA 115:9767–9772. doi:10.1073/pnas.181000411530209218 PMC 6166819 · doi ↗ · pubmed ↗
- 4Kim S, Lieberman TD, Kishony R. 2014. Alternating antibiotic treatments constrain evolutionary paths to multidrug resistance. Proc Natl Acad Sci USA 111:14494–14499. doi:10.1073/pnas.140980011125246554 PMC 4210010 · doi ↗ · pubmed ↗
- 5Batra A, Roemhild R, Rousseau E, Franzenburg S, Niemann S, Schulenburg H. 2021. High potency of sequential therapy with only β-lactam antibiotics. Elife 10:e 68876. doi:10.7554/e Life.6887634318749 PMC 8456660 · doi ↗ · pubmed ↗
- 6Imamovic L, Sommer MOA. 2013. Use of collateral sensitivity networks to design drug cycling protocols that avoid resistance development. Sci Transl Med 5:204ra 132. doi:10.1126/scitranslmed.300660924068739 · doi ↗ · pubmed ↗
- 7Munck C, Gumpert HK, Wallin AIN, Wang HH, Sommer MOA. 2014. Prediction of resistance development against drug combinations by collateral responses to component drugs. Sci Transl Med 6:262ra 156. doi:10.1126/scitranslmed.3009940 PMC 450333125391482 · doi ↗ · pubmed ↗
- 8Podnecky NL, Fredheim EGA, Kloos J, Sørum V, Primicerio R, Roberts AP, Rozen DE, Samuelsen Ø, Johnsen PJ. 2018. Conserved collateral antibiotic susceptibility networks in diverse clinical strains of Escherichia coli. Nat Commun 9:3673. doi:10.1038/s 41467-018-06143-y 30202004 PMC 6131505 · doi ↗ · pubmed ↗