No Surprises Act Independent Dispute Resolution Outcomes for Air Ambulances
Erin L. Duffy, Christopher Garmon

TL;DR
A study analyzed air ambulance payment disputes in 2023 under the No Surprises Act, finding that air ambulance companies won most cases and requested higher payments than insurers.
Contribution
The study provides the first detailed analysis of air ambulance dispute resolution outcomes under the No Surprises Act in 2023.
Findings
Air ambulance organizations won 86.4% of disputes, with private equity-backed organizations involved in 61.3% of cases.
Winning offers averaged $32,463, significantly higher than insurers' median contracted rates.
Only 48.4% of cases had full financial data, limiting comprehensive analysis.
Abstract
What were the outcomes of air ambulance cases processed by the No Surprises Act’s independent dispute resolution entities in 2023? In this cross-sectional study of 5678 cases, arbiters decided in favor of air ambulance organizations in 86.4% of the disputes against insurers, and 61.3% of cases involved a private equity–backed organization. Financial measures were reported for only 48.4% cases; among them, the mean qualifying payment amount (a measure of the insurer’s median contracted rate) and winning offers were 32 463, respectively. These findings suggest that more complete public data on air ambulance independent dispute resolution cases is needed to monitor the impacts of the No Surprises Act. This cross-sectional study describes independent dispute resolution cases arbitrated in 2023 for fixed and rotary wing air ambulance services following the No Surprises Act.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
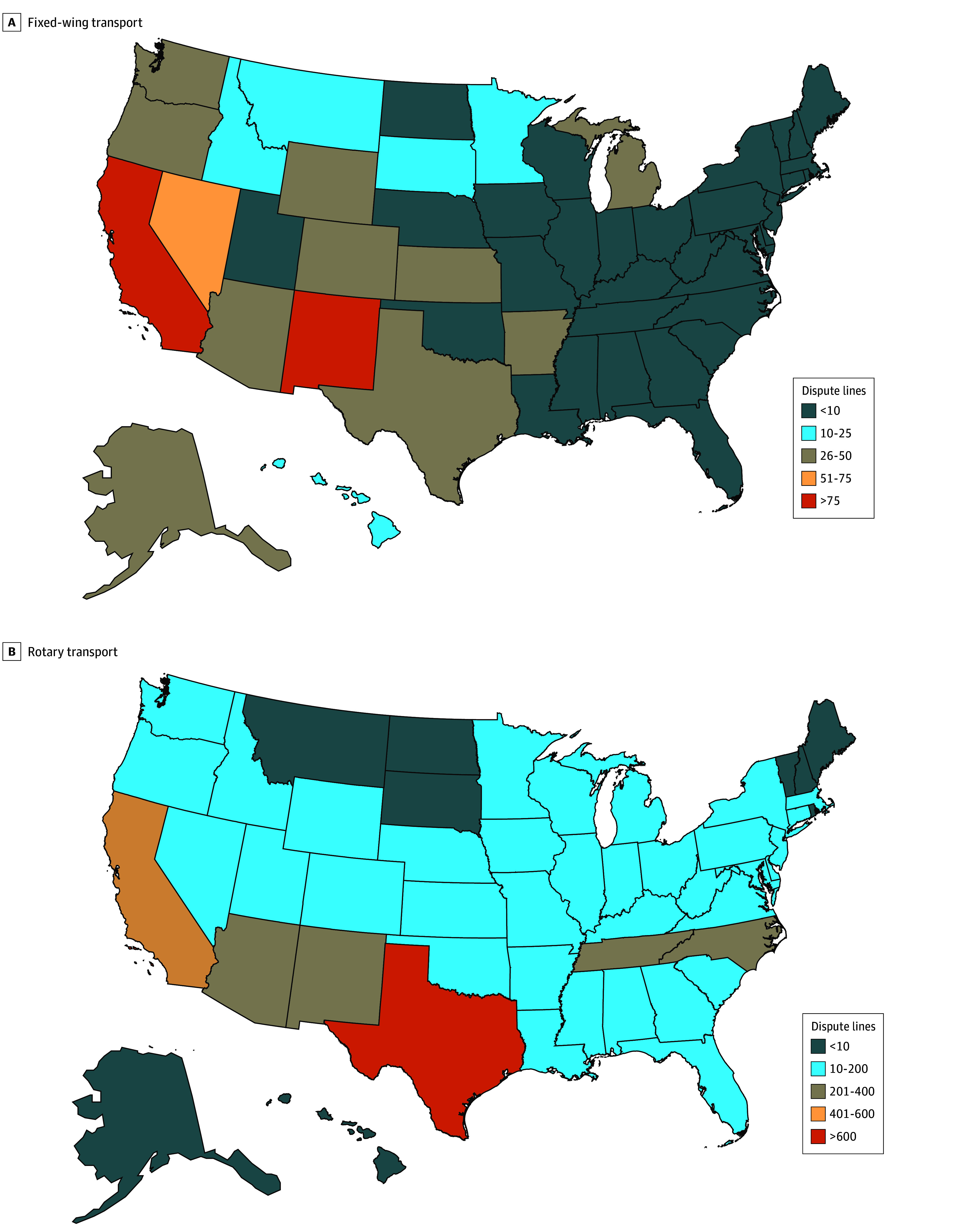 Figure 1
Figure 1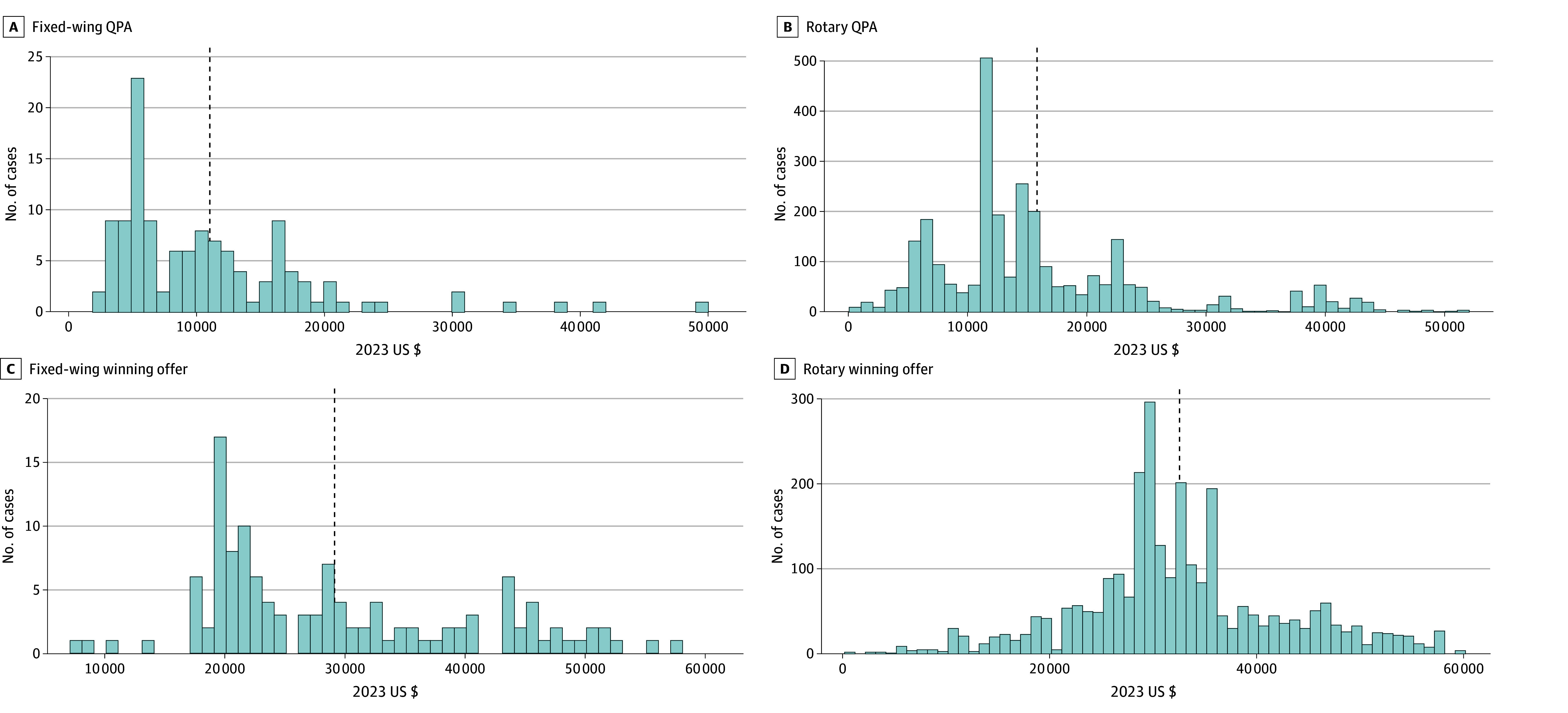 Figure 2
Figure 2| Characteristic | No. (%) of dispute lines | ||
|---|---|---|---|
| Fixed wing (n = 743) | Rotary wing (n = 4935) | All (N = 5678) | |
| Health plan offer >QPA | |||
| No | 331 (44.5) | 2361 (47.8) | 2692 (47.4) |
| Yes | 412 (55.5) | 2574 (52.2) | 2986 (52.6) |
| Outcome | |||
| Health plan wins | 125 (16.8) | 644 (13.0) | 769 (13.5) |
| Air ambulance organization wins | 618 (83.2) | 4287 (86.9) | 4905 (86.4) |
| Split decision | 0 | 4 (0.1) | 4 (0.1) |
| Air ambulance parent organization | |||
| Global Medical Response (PE) | 402 (54.1) | 2012 (40.8) | 2414 (42.5) |
| Phi Air Medical (PT) | 10 (1.3) | 1324 (26.8) | 1334 (23.5) |
| Air Methods (PE) | 72 (9.7) | 719 (14.6) | 791 (13.9) |
| Apollo MedFlight (PE) | 50 (6.7) | 223 (4.5) | 273 (4.8) |
| Life Flight | 51 (6.9) | 144 (2.9) | 195 (3.4) |
| Other | 158 (21.3) | 513 (10.4) | 671 (11.8) |
| Health plan parent organization | |||
| Aetna Inc (PT) | 72 (9.7) | 602 (12.2) | 674 (11.9) |
| Anthem Inc (PT) | 88 (11.8) | 279 (5.7) | 367 (6.5) |
| Non-Anthem Blue | 247 (33.2) | 1209 (24.5) | 1456 (25.6) |
| Centene Corporation (PT) | 6 (0.8) | 189 (3.8) | 195 (3.4) |
| Cigna Group (PT) | 27 (3.6) | 227 (4.6) | 254 (4.5) |
| Clear Health Strategies LLC | 52 (7.0) | 308 (6.2) | 360 (6.3) |
| Kaiser Permanente | 17 (2.3) | 280 (5.7) | 297 (5.2) |
| MultiPlan Corporation (PT) | 61 (8.2) | 528 (10.7) | 589 (10.4) |
| UHC (PT) | 25 (3.4) | 449 (9.1) | 474 (8.3) |
| Zelis (PE) | 30 (4.0) | 239 (4.8) | 269 (4.7) |
| Other | 118 (15.9) | 625 (12.7) | 743 (13.1) |
| Air ambulance organization offer as multiple of QPA, mean (SD) | 3.74 (3.00) | 3.09 (4.34) | 3.18 (4.20) |
| Health plan offer as multiple of QPA, mean (SD) | 1.31 (0.83) | 1.40 (4.16) | 1.39 (3.89) |
| Winning offer as multiple of QPA, mean (SD) | 3.33 (2.87) | 2.89 (4.27) | 2.95 (4.12) |
| Characteristic | Dispute lines, No. (%) | ||
|---|---|---|---|
| Non-PE (n = 2200) | PE (n = 3478) | Total (N = 5678) | |
| Health plan offer >QPA | |||
| No | 1190 (54.1) | 1502 (43.2) | 2692 (47.4) |
| Yes | 1010 (45.9) | 1976 (56.8) | 2986 (52.6) |
| Outcome | |||
| Health plan wins | 314 (14.3) | 455 (13.1) | 769 (13.5) |
| Air ambulance organization wins | 1882 (85.5) | 3023 (86.9) | 4905 (86.4) |
| Split decision | 4 (0.2) | 0 | 4 (0.1) |
| Air ambulance organization offer as multiple of QPA, mean (SD) | 2.18 (1.99) | 3.80 (5.02) | 3.18 (4.20) |
| Health plan offer as multiple of QPA, mean (SD) | 1.12 (1.01) | 1.58 (4.96) | 1.39 (3.89) |
| Winning offer as multiple of QPA, mean (SD) | 2.04 (1.96) | 3.52 (4.94) | 2.95 (4.12) |
| Variable | Transport, Mean (SD) | ||
|---|---|---|---|
| Fixed-wing (n = 126) | Rotary (n = 2929) | All (n = 3055) | |
| QPA, US $ | 11 080.62 (8078.10) | 15 755.40 (9751.05) | 15 561.08 (9730.97) |
| Offer, US $ | |||
| Air ambulance organization | 29 676.08 (11 326.36) | 34 499.24 (8810.12) | 34 290.54 (8985.03) |
| Health plan | 9038.34 (5323.46) | 16 788.00 (15 116.26) | 16 742.90 (15 088.73) |
| Prevailing | 29 115.42 (11 292.36) | 32 610.97 (9902.10) | 32 463.70 (9987.17) |
| Ratio of QPA to Medicare urban rate, mean (SD) | 3.09 (2.24) | 3.77 (2.31) | 3.74 (2.31) |
| Ratio of offer to Medicare urban rate, mean (SD) | |||
| Air ambulance organization | 8.32 (3.22) | 8.26 (2.07) | 8.26 (2.14) |
| Health plan | 2.70 (1.59) | 4.03 (3.75) | 4.02 (3.74) |
| Prevailing | 8.15 (3.20) | 7.81 (2.35) | 7.82 (2.39) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Malpractice and Liability Issues · Healthcare Policy and Management · Healthcare cost, quality, practices
Introduction
Air ambulance transportation comprises travel by fixed-wing and rotary (helicopter) aircraft and is used to transport patients from scenes of an emergency or between facilities when time or travel conditions prohibit use of a ground ambulance. These services are used annually by 1 in 4000 commercially insured people and 1 in 350 Medicare beneficiaries.^1^ Patients do not typically choose the air transportation organization serving them due to the nature of emergencies, geography, and logistics involved. Air transport availability for emergency scenarios requires pilots, clinicians, and aircraft to be prepared for flight at all times. Air ambulance organizations make significant investment in infrastructure, maintenance, and staff to maintain readiness and comply with Federal Aviation Administration regulations, and they face uncertain expected utilization.
Prior to the implementation of the No Surprises Act (NSA) in 2022, commercially insured patients could be billed for the balance between an out-of-network air transportation organization’s charges and their insurer’s allowed amount (ie, a surprise bill), while Medicare and Medicaid patients were insulated from such bills. A study of commercial insurance claims from 2013 to 2017 found that most air ambulance services were out-of-network, and more than half left patients vulnerable to potential surprise bills averaging approximately $20 000.^2^ Other studies evaluating air ambulance charges found they were highly variable, with higher charges among larger organizations and organizations that are publicly traded and have private equity (PE) ownership.^3,4^ PE-owned air ambulance organizations have been found to receive higher payments and yield more and larger surprise bills than organizations with hospital, nonprofit, and independent ownership arrangements.^5^
The NSA was passed in December 2020 and implemented in January 2022. This federal law banned surprise billing for air ambulance transport as well as for emergency care and out-of-network services at an in-network facility. The NSA also established the independent dispute resolution (IDR) process to resolve payment disagreements between health care providers (eg, physicians, hospitals, air ambulance organizations) and insurers. In this binding final-offer arbitration system, arbiters must choose either the insurer’s offer or the provider’s offer, taking into consideration several factors, including any past contracts between the parties, the details of the service conducted, and the insurer’s computed median contracted rate for the same or similar service in the given market, which is known as the qualifying payment amount (QPA).
The implementation of the IDR has been punctuated by litigation that has altered rulemaking and triggered closure of the IDR portal from August through December of 2023.^6,7^ Specific to air ambulance services, the *LifeNet, Inc, et al v US Department of Health and Human Services et al *case challenges QPA calculation methodology.^8^ Additionally, ongoing cases Guardian Flight, LLC, v Medical Evaluators of Texas in the Fifth Circuit^9^ and *REACH Air Medical Services LLC v Kaiser Foundation Health Plan Inc et al *in the Eleventh Circuit^10^ both challenge the validity of IDR entities’ arbitration decisions.
Monitoring and analyzing the outcomes of the IDR process can inform evolving rulemaking and shed light on the fiscal impacts of the NSA. This study describes IDR cases arbitrated in 2023 for fixed-wing and rotary air ambulance services. Though there have been other studies of IDR outcomes, to our knowledge this is the first study focusing on air ambulance services.^11,12,13^
Methods
Data Source
This cross-sectional study used public IDR reports published by the Centers for Medicare & Medicaid Services (CMS) for each quarter of 2023.^14^ Although the portal was closed to new IDR cases for part of 2023, the backlog of previously submitted cases continued to be arbitrated during this period. Every air transport generates 2 claims: one for activation (akin to a base fee for the flight) and one for mileage. In the IDR system, activation and mileage services are reported as separate disputes and are unpaired. Mileage disputes do not report the miles traveled in the data released by CMS, limiting the interpretability of these dispute outcomes. With these data limitations, this study focused only on activation disputes for rotary (Current Procedural Terminology [CPT] code A0431) and fixed-wing (CPT code A0430) transports. The institutional review board of the University of Southern California, Los Angeles, determined this study was not human participant research. This report follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Data are provided by CMS in 2 files that cannot be merged, each with strengths and limitations. This data structure was presumably designed by CMS to deidentify insurers’ QPA amounts. The first file contains observations of each air ambulance dispute with disclosed parties and outcomes relative to QPA (nonmonetary file). The advantage of this file is that it enables one to observe which air ambulance organizations and insurers are disputing cases against one another. A limitation of this file is that it expresses magnitudes of offers and decisions as ratios to QPA values, without disclosing the underlying QPA values in dollars. Given that there is variation in QPA values, these ratios cannot be used to reliably interpret the financial magnitude of offers and decisions. The second file contains observations of disputes with monetary measures of offers and decisions without identifying parties involved (monetary file). The advantage of this file is that it discloses dollar values, enabling benchmarking to Medicare and consideration of the financial implication of the NSA. However, this file has missing data for many observations, and it does not disclose the parties involved in disputes. We leverage the strengths of each file to gain insights on the parties involved and outcomes of IDR cases.
Measures
The number of activation components of fixed-wing and rotary transport disputes, the parties involved, and the prevailing party were described using the nonmonetary file. The air ambulance organization offer, insurer offer, and arbiter decisions were reported relative to the QPA. These case attributes were described separately for organizations with and without PE investments (as identified in eTable 1 in Supplement 1), as well as by quarter of the year. Density maps were used to describe the count of disputes from each state.
The QPA, air ambulance organization offer, insurer offer, and arbiter decisions were described in nominal 2023 US dollars using the monetary file. Monetary values were also compared with Medicare urban reimbursement rates. Rural or urban pickup designations are an important element in air ambulance billing, but geographic information in the data released by CMS was not sufficient to determine an urban or a rural pickup location. For comparison with Medicare, we apply the urban pickup rate in the primary analysis.
Statistical Analysis
Data were analyzed between August 1 and September 1, 2024. Categorical outcomes are described with frequencies and percentages. Continuous outcomes are described with means and SDs. Histograms are also used to assess the distributions of prevailing offers and QPA values. Three ratios of winning value to QPA that exceeded 1000 were excluded as outliers, with the next highest value being 184, strongly suggesting that these 3 outliers are erroneous entries. Three observations with a negative winning value to QPA ratio were also excluded. All statistical analyses were performed using Stata, version 18 (StataCorp LLC). For analyses that combine rotary and fixed-wing services, the descriptive statistics for each wing type are included separately in eTables 2, 3, 5, and 6 and eFigure 2 in Supplement 1.
Results
The analytic sample from the nonmonetary file included 743 fixed-wing and 4935 rotary transports for a total of 5678 disputes (Table 1). Air ambulance organizations won 86.4% of the cases (4905 of 5678) at a mean (SD) magnitude 2.95 (4.12) times the QPA, applying ratios to QPA reported in the nonmonetary file. Plans offered a mean (SD) of 1.39 (3.89) times the QPA, and air ambulance organizations offered 3.18 (4.20) times the QPA. The distributions of ratios of winning offers to QPA are shown in eFigures 1 and 2 in Supplement 1. In 52.6% of cases (2986 of 5678), the health plan offered more than the QPA in arbitration. Most of the 5678 disputes involved the organizations Global Medical Response (2414 [42.5%]), Phi Air Medical (1334 [23.5%]), and Air Methods Corporation (791 [13.9%]). Health plan participation in IDR was spread among many insurance carriers, as well as insurer partners MultiPlan Corporation and Zelis. Rotary transport disputes came from states all across the country, while fixed-wing transport disputes were concentrated in some Western states, particularly California, New Mexico, and Nevada (Figure 1).
Maps of Dispute Case Counts by StateNegative winning values and outliers are excluded.
PE-backed air ambulance organizations represented 61.3% of dispute lines (3478 of 5678) (Table 2). Organizations with and without PE backing won a similar proportion of cases, at 86.9% (3023 of 3478) and 85.5% (1882 of 2200), respectively. Mean (SD) winning offers for PE organizations were 3.52 (4.94) times the QPA, while winning offers for non-PE organizations were 2.04 (1.96) times the QPA. The mean insurer offer and organization offer relative to QPA were greater when the dispute involved a PE-backed organization compared with when the organization was not PE backed. These results are shown disaggregated by fixed-wing and rotary transport in eTables 2 and 3 in Supplement 1, and the disaggregated results are similar to the aggregate results.
Across the 4 quarters of 2023, we observed an increase in the share of disputes won by health plans from 9.1% (114 of 1250) in quarter 1 to 17.1% (200 of 1170) in quarter 4 (eTable 4 in Supplement 1). Accompanying this trend, we observed that health plans increasingly made offers above the QPA—33.8% of the time (422 of 1250 cases) in quarter 1 and 59.1% of the time (692 of 1170 cases) in quarter 4. The mean (SD) number of days for the arbiters to make decisions also extended over the year from 55 (25) days in quarter 1 to 136 (68) days in quarter 4, reflecting the backlog of cases and the pausing of new cases in the latter part of the calendar year. Quarterly results are shown disaggregated by fixed-wing and rotary transport in eTables 5 and 6 in Supplement 1, and the disaggregated results are similar to the aggregate results.
The monetary analytic file includes 126 fixed-wing and 2929 rotary transport disputes, totaling 3055 cases (Table 3). Notably, this is much lower than the 5678 cases reported in the nonmonetary file. The mean QPA and the air ambulance organization, health plan, and prevailing offers for rotary activation disputes were greater than for fixed-wing activation disputes. Overall, mean (SD) QPA was 9730.97) and prevailing offers were for a mean (SD) of 9987.17). The mean (SD) air ambulance organization and health plan offers were 8985.03) and 15 088.73), respectively. QPAs and prevailing offers were a mean (SD) of 3.74 (2.31) and 7.82 (2.39) times the Medicare urban allowed amounts, respectively. Figure 2 presents the distributions of QPA and prevailing offers for rotary and fixed-wing transport disputes, demonstrating the substantial variation in these values.
Histograms of Qualifying Payment Amounts (QPA) and Winning Offers for Rotary and Fixed-Wing Transport InitiationsThe vertical dashed lines represent the means. Mean (SD) QPA and winning offers are given in Table 3.
Monetary aspects of IDR cases were masked at a far higher rate for air ambulance transport than other services (eTable 7 in Supplement 1). For air ambulance activation dispute lines, 48.4% of dispute lines (2897 of 5983) report the monetary value of both the QPA and winning offer. Thus, analysis of the monetary aspects of disputes was not feasible for more than half of air ambulance disputes. In contrast, 85.0% of emergency services (140 232 of 165 024) and 64.7% of other services (108 999 of 168 481) report both the QPA and winning offer in dollars in the publicly released files.
Discussion
In this cross-sectional study of 2023 NSA IDR outcomes for air ambulance transport disputes, air ambulance organizations won 86.4% of cases at mean (SD) amounts of 2.95 (4.12) times the QPA and 7.82 (2.39) times Medicare reimbursements. These are higher than pre-NSA in-network allowed amounts, which were 3 to 5 times Medicare reimbursements,^15,16^ but roughly consistent with pre-NSA charges, which were 4 to 9 times Medicare reimbursements.^3^
This study also found that PE-backed air ambulance organizations comprised more than half (61.3%) of dispute lines and yielded higher prevailing amounts in the IDR process than organizations without PE investment. A study of 2016-2017 commercial claims data^5^ reported that PE and publicly traded air ambulance organizations had higher allowed amounts for both in-network and out-of-network services than independent, hospital-owned, and nonprofit air ambulance organizations. This same pre-NSA study also reported that PE and publicly traded air ambulances were more often out-of-network and more often generated possible surprise billing scenarios. Air ambulance companies can no longer bill for the balance, but the higher IDR winnings for PE-backed organizations observed in this study suggest that the payment advantage of PE-backed organizations may have persisted after the NSA. The relatively frequent use of IDR by large PE-backed and publicly traded organizations may indicate that the costs and administrative processes of the IDR system are discouraging its use by smaller independent and nonprofit organizations. Composing a compelling case for arbitration may require time and effort from clinicians, drawing them away from treating patients, and this use of expertise may not be feasible for smaller organizations.
At the time of this analysis, only 2023 IDR data were publicly available to researchers, released in quarterly files. The quarter assignments in these data are based on the quarter an arbiter decided the case. There was an increase in the share of IDR cases with insurer offers above the QPA and an increase in the proportion of cases that insurers won during the 4 quarters of 2023. This suggests that insurers may have adapted their strategy in IDR offers over time, perhaps based on their experience with IDR. Important context for interpreting this trend is that the IDR was closed to new submission from August through December 2023 and the system experienced a backlog and processing time lag.^7^ Therefore, the offers we saw in quarters 3 and 4 were actually made much earlier. We saw a snapshot of IDR activity, and the offers and decisions may have changed in the months since then.
The future of the IDR process depends on the outcomes of several ongoing legal cases about the QPA calculation methodology and the validity of arbitration decisions.^8,9,10^ Additionally, the first reported audit of an insurance carrier’s QPA calculation was released in July 2024.^17^ The audit focused on Aetna Inc’s handling of air ambulance cases and identified 3 violations, including the use of paid claims rather than contracts in QPA calculations. The resolution of NSA-related litigation and further auditing of QPA calculations may change future IDR outcomes.
Monitoring of the IDR outcomes for air ambulance services is constrained by the limited public data for these cases. The separation of activation and mileage claims for the same flight makes it difficult to assess the overall IDR payment outcome for a transport. The lack of mileage and information on pickup location limits the accuracy of benchmarking payments. CMS could make more complete data available for monitoring and consider grouping the activation and mileage components of air transport claims as disputes are processed. This transparency would inform the behavior of insurers and air ambulance organizations, and the clinicians involved, as they engage in the IDR process.
Limitations
The publicly available IDR data have several limitations. Though air ambulance transportation services always comprise paired activation and mileage claims, these claims are not linked in the IDR data. The data do not include mileage or pickup location designation as rural or urban, limiting interpretability and benchmarking accuracy. The file with detailed party information cannot be linked with monetary information, making it infeasible to assess variation in offers and win amounts by party. Nearly half of cases have masked data fields, and it is not possible to determine whether observations about the unmasked cases are generalizable to the masked cases.
This study captures a single year of IDR outcomes, 2023. These are the only IDR data available to the public as of September 1, 2024. Litigation and rulemaking are ongoing, so the observations in the study offer insights to inform that process. Future data releases can be analyzed to build on this study and understand the evolving landscape.
Conclusions
In this cross-sectional study of payment disputes, air ambulance organizations won most disputes against health plans. PE-backed organizations were involved in 3 in 5 disputes, and their cases had higher organization, health plan, and prevailing monetary offers. Continued monitoring of air ambulance IDR cases is needed to assess the impacts of the NSA, particularly in light of ongoing litigation and opportunities to inform evolving rulemaking. However, due to suppression of observations in the monetary file and lack of mileage and urban or rural service information, it was not possible to get a comprehensive picture of the financial aspects of air ambulance transport IDR cases in the publicly released data.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Turrini G, Ruhter J, Chappel AR, De Lew N. Air ambulance use and surprise billing. Dept of Health and Human Services Assistant Secretary of Planning and Evaluation Office of Health Policy. Issue Brief HP-2021-20. September 10, 2021. Accessed September 10, 2024. https://aspe.hhs.gov/sites/default/files/2021-09/aspe-air-ambulance-ib-09-10-2021.pdf
- 2Chhabra KR, Mc Guire K, Sheetz KH, Scott JW, Nuliyalu U, Ryan AM. Most patients undergoing ground and air ambulance transportation receive sizable out-of-network bills. Health Aff (Millwood). 2020;39(5):777-782. doi:10.1377/hlthaff.2019.01484 32293925 · doi ↗ · pubmed ↗
- 3Bai G, Chanmugam A, Suslow VY, Anderson GF. Air ambulances with sky-high charges. Health Aff (Millwood). 2019;38(7):1195-1200. doi:10.1377/hlthaff.2018.05375 31260345 · doi ↗ · pubmed ↗
- 4Adler L, Hannick K, Lee S. High air ambulance charges concentrated in private equity-owned carriers. Brookings Institution. October 13, 2020. Accessed September 10, 2024. https://www.brookings.edu/articles/high-air-ambulance-charges-concentrated-in-private-equity-owned-carriers/
- 5Adler L, Milhaupt C, Ly B, Trish E. Private equity–owned air ambulances receive higher payments, generate larger and more frequent surprise bills. Brookings Institution. November 16, 2021. Accessed September 10, 2024. https://www.brookings.edu/articles/private-equity-owned-air-ambulances-receive-higher-payments/
- 6O’Neill Institute Health Care Litigation Tracker. No Surprises Act. Accessed September 10, 2024. https://litigationtracker.law.georgetown.edu/issues/no-surprises-act/
- 7Centers for Medicare & Medicaid Services. No Surprises Act Notices. Relevant notices published August through December 2023. Accessed September 10, 2024. https://www.cms.gov/nosurprises/notices
- 8Life Net, Inc, et al v US Department of Health and Human Services et al. Docket No. 6:22-cv-00453. District Court of Eastern Texas. Filed December 1, 2022.