Relentless Headaches and Syncope: A Case of Neuropsychiatric Systemic Lupus Erythematosus in a Pediatric Male Patient
Alaa S Mehair, Dalia Said, Najla Aljaberi

TL;DR
This paper presents a case of a young boy with severe lupus affecting the brain, showing how it can cause confusing symptoms like headaches and fainting.
Contribution
The paper highlights a rare and challenging case of NPSLE in a pediatric male with early-onset neurological symptoms.
Findings
NPSLE can manifest with non-specific symptoms in children, complicating diagnosis.
The case shows early neurological involvement in cSLE, within a month of diagnosis.
Positive radiologic findings supported the NPSLE diagnosis in this patient.
Abstract
Childhood systemic lupus erythematosus (cSLE) is a rare multisystem autoimmune disease with considerable morbidity as it has been typically reported to be more severe than in adults. Neuropsychiatric SLE (NPSLE) is the second leading cause of lupus-related morbidity in the pediatric age group, mostly occurring within the first year of onset, but may develop at any time. It can present with a range of vague specific neurologic manifestations which can be challenging to diagnose. Here, we present a case of NPSLE in an 11-year-old male, presenting less than a month after diagnosis with positive radiologic features.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
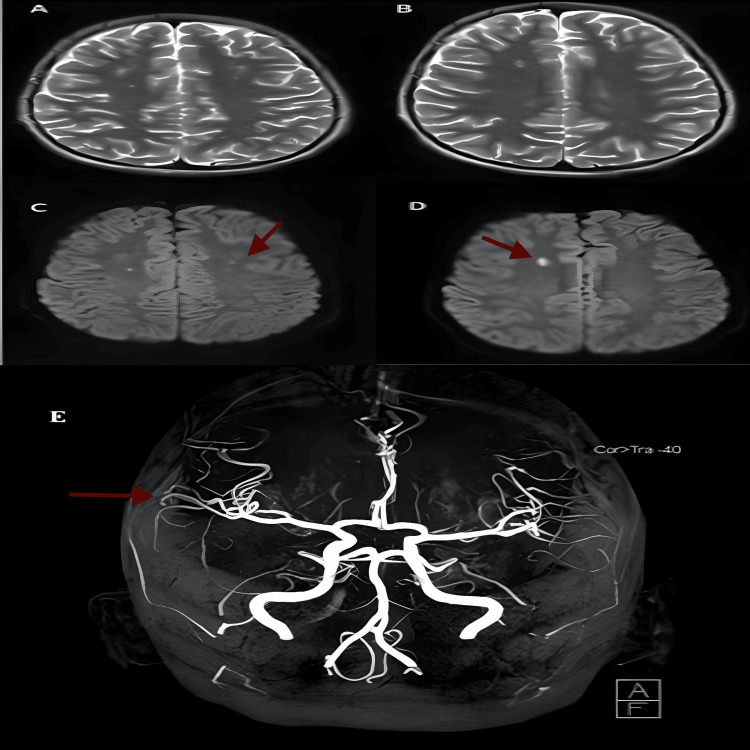 Figure 1
Figure 1| Laboratory test | Value | Reference range |
| White blood cell count | 3.2 x 109/L | 4.5-13.5 x 109/L |
| Hemoglobin | 72 g/L | 11.7-16.6 g/L |
| Platelet count | 232 x 109/L | 140-400 x 109/L |
| Direct antigen test (Coombs) | Positive | - |
| Erythrocyte sedimentation rate | 40 mm/hour | 0-20 mm/hour |
| C-reactive protein | 6.7 mg/L | <=5 mg/L |
| Anti-streptolysin O titer | 74 IU/mL | <=240 |
| Throat culture | Negative | - |
| Serum C3 | 0.17 g/L | 0.9-1.8 g/L |
| Serum C4 | 0.03 g/L | 0.10-0.40 g/L |
| ANA | Positive titer 1:1,280 | - |
| Anti-double-stranded DNA | Positive titer >666.9 IU/mL | - |
| Anti-Smith | Positive | - |
| Anti-SM/RNP | Positive | - |
| Urine protein/creatinine ratio | 2.52 g/g | - |
| 24-hour urine protein | 1.35 g/day | - |
| Urine analysis | No casts; red blood cells: 51 x 106/L; white blood cells: 9 x 106/L | - |
| Laboratory test | Value | Reference range |
| Anti-cardiolipin IgG | 25.5 CU | <=20.0 CU |
| Anti-cardiolipin IgM | 5.7 CU | <=20.0 CU |
| Anti-β2 glycoprotein IgG | 41.7 CU | <=20.0 CU |
| Anti-β2 glycoprotein IgM | 7.4 CU | <=20.0 CU |
| Lupus anticoagulant | Negative | - |
| PT | 10.4 seconds | 12.7-16.1 seconds |
| APTT | 19.5 seconds | 33.9-46.1 seconds |
| INR | 0.94 seconds | 0.97-1.30 seconds |
| D-Dimer | 2.060 mg/L | 0.129-0.523 mg/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Autoimmune Neurological Disorders and Treatments · Peripheral Neuropathies and Disorders
Introduction
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease with considerable morbidity [1]. The worldwide estimated prevalence of SLE is 3.3 to 9.7 per 100,000 children and adolescents [2]. Although the prevalence of SLE in the United Arab Emirates (UAE) is estimated to be relatively high based on the current scarce evidence [3-4], childhood SLE (cSLE) in the UAE is highly underreported and under-investigated. Among the systemic manifestations of SLE, neuropsychiatric SLE (NPSLE) is associated with pediatric presentations and high morbidity [5].
Case presentation
An 11-year-old Arab male presented with a three-week history of intermittent fever, migratory joint pain, and swelling. His history was positive for fatigue and loss of appetite, but negative for skin rashes, mouth ulcers, weight loss, visual changes, or previous infections. On examination, he was pale, febrile, and had tachycardia with normal blood pressure. His weight was below the 3rd percentile. The musculoskeletal exam revealed an antalgic gait, with swelling and tenderness in both the metacarpophalangeal and tibiotarsal joints. Initial laboratory investigations showed a picture of autoimmune hemolytic anemia with leukopenia. An autoimmune rheumatologic disorder was suspected and further labs were requested. These revealed anemia, a positive Coombs test, and positive results for anti-nuclear antibodies (ANA), anti-double stranded DNA, anti-Smith, and anti-small nuclear ribonucleoprotein (anti-SM/RNP) (Table 1).
A clinical diagnosis of SLE was made and the patient met the classification criteria of the 2019 European League Against Rheumatism/American College of Rheumatology (EULAR/ACR). The patient’s Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) scored 32, which indicated a very high activity of SLE. The patient was started on pulse steroids (Methylprednisolone IV) at 30 mg/kg for three days. Afterward, he was continued on oral prednisolone at 15 mg once daily as a starting dose. Lupus nephritis was suspected, and the patient underwent renal biopsy (after three doses of pulse steroids at 30 mg/kg). The biopsy showed diffuse proliferative lupus nephritis, classified as class IV-S (diffuse segmental) and G (diffuse global) of the International Society of Nephrology/Renal Pathology Society classification. Following that, the patient's oral prednisolone dose was increased to 20 mg daily, and mycophenolate mofetil (MMF) was started at 750 mg twice daily (BID), with a target dose of 600 mg/m² BID. As the patient developed hypertension and proteinuria, he was subsequently started on enalapril 5 mg twice daily. Cardiac echocardiogram (ECHO) and chest X-ray were normal. Further labs were sent to test for antiphospholipid antibodies, which revealed positive results for anti-cardiolipin IgG and anti-β2 glycoprotein IgG (Table 2).
The patient was discharged home on oral prednisolone (20 mg) and MMF (750 mg BID). Ten days after diagnosis, he developed multiple intermittent episodes of headache, requiring two emergency room visits, where only supportive treatment was provided. Eventually, his headache became progressive, and he presented to the hospital again, this time experiencing two brief episodes of syncope.
His headache initially started in the frontal area, and within 24 hours, it started to radiate to the occipital region. The headache was mostly in the morning and associated with photophobia and early morning vomiting, which was non-projectile and non-bilious. On the day of the presentation, his pain was so intense that he lost consciousness for about two minutes and was unresponsive. He regained consciousness within two minutes. No abnormal jerky movements were noted.
Upon arrival at the emergency department, his vital signs were unstable and revealed elevated blood pressure of 155/115 mmHg, respiratory rate of 28 breaths per minute, and heart rate of 122 beats per minute. He was fully alert and conscious upon arrival at the hospital. His neurological and fundoscopic examinations were normal. Other systemic examinations were unremarkable, and both the ECHO and electrocardiogram (ECG) were normal. CT brain without contrast, which was done in the emergency department within one hour of the symptoms, ruled out cerebral hemorrhage, edema, or increased intracranial pressure.
In light of his hypertensive urgency, one dose of intravenous hydralazine 0.1 mg/ kg was given. A brain MRI with contrast showed small acute infarcts in the right frontal lobe for which he was diagnosed as a case of cerebral vasculitis as part of NPSLE manifestation. Magnetic resonance angiography (MRA) did not depict significant irregularities suggestive of underlying large-vessel vasculitis (Figure 1).
(A-D) MRI brain axial T2 sequences show high signal intensity foci involving both coronal radiata (bilateral centrum semiovale) (A) and the right frontal lobe (B), with corresponding restricted diffusion on axial diffusion-weighted images (DWI) (C, D), suggestive of neuropsychiatric SLE (arrows indicate the findings); (E) 3D TOF MR angiography in coronal reconstruction of the cerebral and cerebellar arteries demonstrates a normal appearance of the major arteries and their branches (arrow for reference).3D TOF MR, three-dimensional time-of-flight magnetic resonance; SLE, systemic lupus erythematosus
He was started on aspirin and received rituximab for active NPSLE. He received two doses of 375 mg/m^2^ of rituximab (amounting to 500 mg per dose).
The patient responded well to rituximab. Both his NPSLE and LN went into remission as he continued MMF and stopped steroids. Repeat antiphospholipid antibody testing continued to be negative afterward. He had a follow-up MRI brain after four months, which showed the presence of old right frontal focal infarction; otherwise, no significant abnormality was seen. No further neurologic issues were encountered as he had normal cognitive functioning and no limitations in daily life or school performance. This continued to be the case three years later at follow-up.
Discussion
cSLE is typically more severe in presentation and morbidity than adult SLE [5]. The vast majority of childhood NPSLE cases present with central nervous system (CNS) involvement, with headaches occurring in up to 79% of cases [6]. The high female-to-male ratio of NPSLE was preserved in most pediatric studies [6] but was significantly more equal in one study from India [7]. There could be unique ethnic factors contributing to SLE presentations in male patients around the world. Patients with NPSLE typically present with an overall globally active disease, which should make the diagnosis of SLE easier. In many patients, especially those with renal involvement, posterior reversible encephalopathy syndrome could be suspected. However, it is always a reasonable approach to pursue imaging in patients with cSLE with neurologic signs, particularly at the beginning of their illness. Neuroimaging with MRI and, if needed, MRA is important to rule out focal findings such as acute vascular lesions, ischemia, and hemorrhage. However, non-specific white matter hyperintensities can be seen without correlation to the disease manifestations. White matter hyperintense lesions on MRI are the most encountered findings in patients with SLE. The correlation between these lesions and the neurological presentation is not entirely clear, as there are reports of these lesions in patients without overt NPSLE symptoms [8].
NPSLE can present with headaches, seizures, cerebrovascular events, cognitive dysfunction, and even psychosis, delirium, or depression. Stroke in SLE may be caused by different mechanisms, including antiphospholipid syndrome, cardiogenic embolism, intracranial hemorrhage secondary to hypertension, vasculopathy, and vasculitis. True vasculitis is difficult to detect on angiography unless large vessels become affected, which is rare [9].
Conclusions
SLE is a multifactorial disease that ultimately leads to multisystem involvement. Despite being a rare entity, it is being increasingly recognized as a major pediatric rheumatologic disease. Furthermore, the great gender variation might have contributed to delayed diagnosis in male patients in a few case reports. However, it is very crucial to keep it in mind with such a clinical presentation as a more severe disease course is noted in male patients.
A multidisciplinary approach is key to successful management, as controlling disease progression can be highly challenging and is essential for reducing morbidity and mortality. Management of NPSLE is directed toward controlling the disease and managing its symptoms. Various immunosuppressant medications are used, including MMF and azathioprine. In addition, rituximab is recommended as a biological therapy for managing similar cases. Further research is needed to identify the most effective treatments and improve control of NPSLE.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mortality in systemic lupus erythematosus: an updated review Curr Rheumatol Rep Fors Nieves CE Izmirly PM 211820162698480510.1007/s 11926-016-0571-2 · doi ↗ · pubmed ↗
- 2Systemic lupus erythematosus in children and adolescents Pediatr Clin North Am Levy DM Kamphuis S 3453645920122256057410.1016/j.pcl.2012.03.007PMC 3348509 · doi ↗ · pubmed ↗
- 3Lupus nephritis: a focus on the United Arab Emirates and the potential role of genetics Lupus Tabouni M Ali A Aljaberi N Alblooshi H 141514223120223601760010.1177/09612033221122982 · doi ↗ · pubmed ↗
- 4Global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modelling study Ann Rheum Dis Tian J Zhang D Yao X Huang Y Lu Q 3513568220233624136310.1136/ard-2022-223035 PMC 9933169 · doi ↗ · pubmed ↗
- 5Neuropsychiatric involvement in juvenile-onset systemic lupus erythematosus (j SLE)Mol Cell Pediatr Natoli V Charras A Hahn G Hedrich CM 51020233755602010.1186/s 40348-023-00161-7PMC 10412509 · doi ↗ · pubmed ↗
- 6Neuropsychiatric involvement in juvenile-onset systemic lupus erythematosus: data from the UK juvenile-onset systemic lupus erythematosus cohort study Lupus Giani T Smith EM Al-Abadi E 195519653020213460198910.1177/09612033211045050 PMC 8649437 · doi ↗ · pubmed ↗
- 7Neuropsychiatric manifestations and antiphospholipid antibodies in pediatric onset lupus: 14 years of experience from a tertiary center of North India Rheumatol Int Singh S Gupta MK Ahluwalia J Singh P Malhi P 145514612920091930609710.1007/s 00296-009-0887-6 · doi ↗ · pubmed ↗
- 8Neuropsychiatric systemic lupus erythematosus: magnetic resonance imaging findings and correlation with clinical and immunological features Autoimmun Rev Toledano P Sarbu N Espinosa G BargallóN Cervera R 116611701220132385113910.1016/j.autrev.2013.07.004 · doi ↗ · pubmed ↗