Pregnant Woman With Lower Abdominal Pain
Yi-Hsuan Hsieh, Siou-Ting Lee, Chen-Yu Wang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
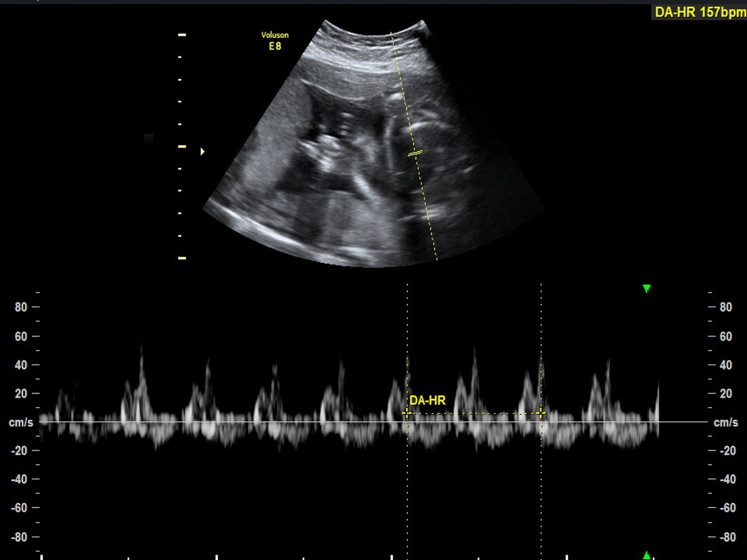 Figure 1
Figure 1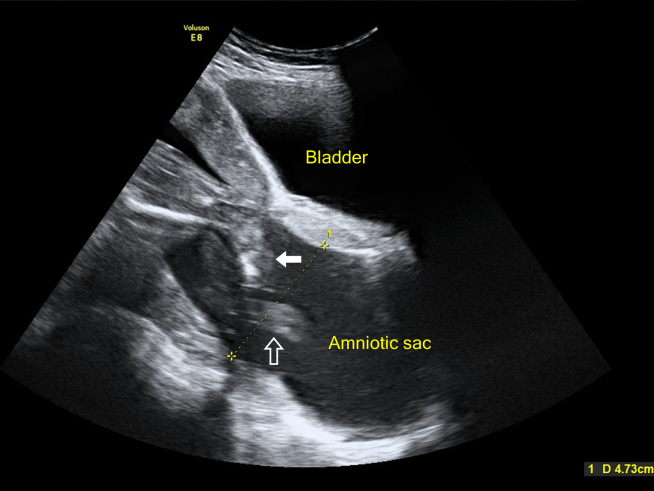 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAppendicitis Diagnosis and Management · Hernia repair and management · Cardiovascular Issues in Pregnancy
Patient Presentation
1
A 39-year-old nulligravid woman at 21 weeks gestation presented to the emergency department with a 1-day history of lower abdominal pain. Physical examination revealed lower pelvic tenderness and occasional uterine contractions. There was no active bleeding or rupture of membranes. The pregnancy was conceived naturally, with prior prenatal checkups being normal. Abdominal ultrasonography showed a protruding amniotic sac, with the fetal legs and umbilical cord extending into the vagina.
Diagnosis: Cervical Insufficiency with Prolapsed Amniotic Sac
2
Abdominal ultrasonography revealed a fetal heart rate of 157 beats per minute (Fig 1). The amniotic sac was bulging through the cervix, creating a classic "hourglass appearance," with the fetal legs (Fig 2, arrow) and umbilical cord (Fig 2, hollow arrow) protruding. The cervix was dilated to approximately 4.73 cm (Fig 2), with an amniotic fluid index of 12.1 cm and no signs of membrane rupture. These findings were consistent with cervical insufficiency, a primary cause of amniotic sac prolapse.1 An emergent cerclage was performed uneventfully.2^,^3Figure 1. The fetal heart rate was 157 beats per minute.Figure 2. Abdominal ultrasonography revealed the amniotic sac bulging through the cervix, creating a classic “hourglass appearance,” with the fetal legs (Fig 2, arrow) and umbilical cord (Fig 2, hollow arrow) protruding. The cervix dilated to approximately 4.73 cm.
Emergency physicians and obstetricians should prioritize abdominal ultrasonography over pelvic examination in pregnant women at or beyond 20 weeks of gestation. Unlike the common emergency department practice of performing a pelvic examination first, ultrasonography can identify critical conditions such as placenta previa or a protruding sac, where a pelvic examination could risk massive hemorrhage,4 sac rupture, preterm labor, or infection. Abdominal ultrasonography offers more valuable information to guide appropriate management.
Conflict of Interest
All authors have affirmed they have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American College of Obstetrics and Gynecologist ACOG practice bulletin. Cervical insufficiency Int J Gynaecol Obstet 8512004818910.1016/s 0020-7292(04)00035-915124633 · doi ↗ · pubmed ↗
- 2Ehsanipoor R.M.Seligman N.S.Saccone G.Physical examination-indicated cerclage: a systematic review and meta-analysis Obstet Gynecol 1261201512513510.1097/AOG.000000000000085026241265 · doi ↗ · pubmed ↗
- 3Ozgur Akkurt M.Yavuz A.Sezik M.Okan Ozkaya M.Infant outcomes following midtrimester emergency cerclage in the presence of fully dilated cervix and prolapsing amniotic membranes into the vagina J Matern Fetal Neonatal Med 291520162438244210.3109/14767058.2015.108749526414335 · doi ↗ · pubmed ↗
- 4Cunningham F.G.Leveno K.J.Dashe J.S.Hoffman B.L.Spong C.Y.Casey B.M.Williams Obstetrics 26e 2022 Mc Graw Hill Professional