Frailty and loneliness among community-dwelling older adults: examining reciprocal associations within a measurement burst design
Anna Schultz, Hannes Mayerl, Wolfgang Freidl, Erwin Stolz

TL;DR
This study examines how frailty and loneliness are related in older adults, finding that they tend to increase together but not in a direct cause-and-effect way.
Contribution
The study uses a measurement burst design to disentangle within- and between-person effects in the relationship between frailty and loneliness.
Findings
No causal reciprocal relationship was found between frailty and loneliness over short time periods.
Higher levels of frailty were weakly associated with higher levels of loneliness at the within-person level.
Frailty and loneliness were significantly correlated at the between-person level in each measurement burst.
Abstract
Previous research indicates that frailty and loneliness are interrelated. The aim of this study is to analyze their possible reciprocal relationship while disentangling between- and within-person effects. The separation of these sources of variance is vital for a better understanding of potential causal mechanisms. Within the FRequent health Assessment In Later life (FRAIL70+) project, participants aged 70 and over completed two measurement bursts spread one year apart with seven biweekly assessments each. The final sample consisted of 426 individuals at baseline (Mage=77.0; SD = 5.4; 64.6% female). A latent curve model with structured residuals was used to examine the potential reciprocal relationship between frailty (37-item deficit accumulation approach) and loneliness (3-item UCLA scale). No relevant cross-lagged effects over repeated 2-week periods were found between frailty and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
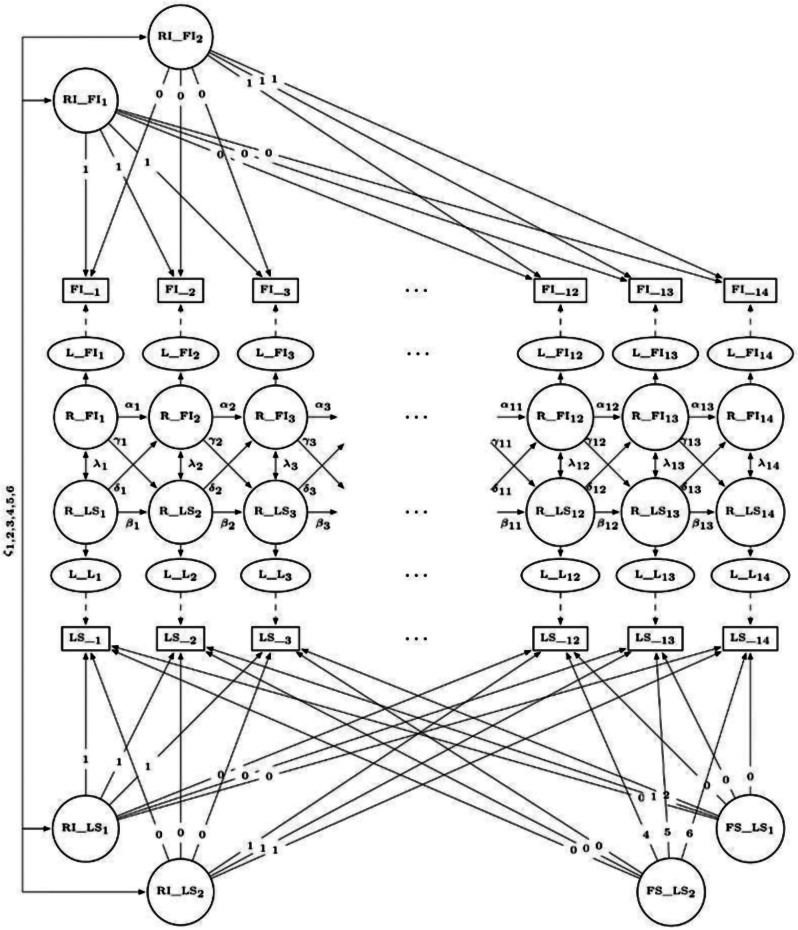 Figure 1
Figure 1- —http://dx.doi.org/10.13039/501100002428Austrian Science Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFrailty in Older Adults · Health disparities and outcomes · Geriatric Care and Nursing Homes
Background
Throughout their lives, people may experience different levels of loneliness, characterized by an imbalance between their current and ideal level of emotional closeness in social relationships [1, 2]. Reviews highlight loneliness’s detrimental effects on mental and physical health, including depressive symptoms, sleep quality, decreased immunity, cognitive decline, and mortality [3–5], emphasizing its public health significance [6]. Older adults seem to be especially susceptible to loneliness [7], with levels often increasing in later life [1], due to the loss of spouses or health problems [8].
Frailty, an indicator of overall health in older adults [9], increases with age [10], and predicts disability, falls, hospitalization, and mortality [11–13] among older adults. Frailty is common among older adults [14], observed in 12–26% [15], and has increased in more recent birth cohorts [16], highlighting it as a grand challenge [10].
Longitudinal studies showed that high levels of loneliness, on the one hand, increase the risk of developing frailty among older adults [17, 18] and on the other, suppress the reversion from (pre-)frailty to robustness [19, 20]. By contrast, research has also demonstrated that frailty and related health outcomes exert an influence on loneliness. In a sample of N = 552 Spanish older adults, frailty domains (physical, psychological, and social) predicted loneliness longitudinally [21]. Likewise, Hoogendijk et al. [22] found a moderate to large effect (Cohen’s d = 0.54) of frailty on loneliness in a sample of N = 856 older adults in the Netherlands.
While previous research has suggested loneliness as a risk factor for frailty, and frailty as a risk factor for loneliness; a single longitudinal study using cross-lagged panel models also suggested a bidirectional relationship between frailty and loneliness. Using three waves of the China Health and Retirement Longitudinal Study, with a time span of 2 years between waves, Shah and colleagues [23] found among N = 2,412 Chinese older adults that frailty and loneliness influence each other, with frailty having a stronger effect on subsequent loneliness than the reverse.
Previous studies have focused on long-term dynamics between loneliness and frailty over multiple years owing to sparse annual or biannual assessment schedules in most health and ageing studies. However, changes likely happen on a much shorter time scale, that is, over weeks and months. For instance, if social contacts of an older adult are severely reduced due to acute or chronic health problems, e.g., an injury that limits mobility or a disability that limits communication, loneliness may follow within weeks or months rather than years. Conversely, a lack of social contacts that usually encourage physical activity, e.g., going for a walk or grocery shopping, could lead to a decline in stamina or muscle strength over the same short-term period. Studies suggest that disability [24, 25], frailty [26] and loneliness [27–30] can exhibit indeed variability over shorter time frames, such as days, weeks or months, for instance, in response to temporary health challenges [24, 25] or social circumstances [27, 30].
In the present study, we use data gathered within a measurement burst design to examine the bidirectional relationship between frailty and loneliness over a couple of weeks and months. Understanding these dynamics is crucial, as lonely older adults living with frailty have a higher mortality risk compared to those who are only frail or lonely [31]. We attempt to shed light onto the frailty-loneliness interplay by distinguishing associations existing at the within-person level (i.e., whether a person experiencing lower health than usual also reports higher loneliness at the same or adjacent point in time) from those at the between-person level (i.e., whether individuals with greater health declines than others are also more likely to experience greater loneliness). This distinction is important, as within- and between-person associations can differ considerably in magnitude or direction [32], highlighting its significance for understanding cause-effect relationships in longitudinal observational data [33].
Methods
Design and data
In the FRequent health Assessment In Later life (FRAIL70+) project, nationwide health data of Austrian community-dwelling older adults aged 70 and above were collected between August 2021 and April 2023 (Supplementary Methods 1; Supplementary Fig. 1) using a measurement burst design [34]. This design involves conducting several assessments (e.g., performance tests, standardized questionnaires) within a relatively short time span (biweekly), which are then repeated at longer intervals (annually). In the first burst, 426 participants (response rate: 44%) completed up to seven biweekly interviews (retention rate = 95.3–98.5%). One year later, 378 participants returned for a second burst (retention rate between bursts = 88.7%), consisting again of seven biweekly assessments (retention rate = 76.7–94.2%; last interview = 53.5%). The study was approved by the Ethics Committee of the Medical University of Graz (EK-number: 33–243 ex 20/21). All participants provided informed consent.
Measures
Frailty
Frailty was operationalized using the Frailty Index (FI; 35), one of the primary methods for assessing frailty [10], through various self-reported health items and cognitive performance tests [36]. A FI was computed from 37 items (see Supplementary Table 1 for more details). No item had > 1.7% missing values. Each item was first mapped to the interval of 0–1 (i.e., dichotomous items were scored 0 or 1, categorical items had, for instance, scores of 0, 0.25, 0.5, 0.75, or 1.0) and then, provided that at least 80% of data were valid, summed up and divided by the number of valid health deficits (e.g., 11/37 = 0.30), resulting in a score ranging (theoretically) between 0 and 1, whereby higher values indicate higher frailty levels. Internal consistency in the current study was ω = 0.89 and is in line with previous studies (ω = 0.89-0.93 [37]; ω = 0.81 [38]). The within-person reliability (ω^w^ [39]) was 0.70 (95% CI = 0.68, 0.71).
Loneliness
Loneliness (LS) was measured using the three-item University of California, Los Angeles loneliness scale (UCLA; [40]; see Supplementary Table 2 for more details). LS scores range from 3 to 9 with higher scores indicating higher levels of LS. Previous research reports satisfactory reliability (α = 0.72) as well as concurrent and discriminant validity [40]. Internal consistency in the current study was ω = 0.76. The within-person reliability (ω^w^ [39]) was 0.63 (95% CI = 0.61, 0.65).
Additional variables
Baseline variables for multiple group analysis, assessed during the first interview in the first burst, included sex (male vs. female), age groups (70–74, 75–79, vs. ≥80 years), living alone (no vs. yes), and social participation (no vs. yes). The FRAIL70 + survey asked participants whether they participated in the following social activities during the past year: (1) volunteer or charitable work, (2) participation in religious institutions (e.g., church, synagogue, or mosque), (3) participation in political organizations or citizens’ initiatives, and (4) participation in educational or training courses. Responses were summed and categorized as 0=“no” and 1=“yes, participation in one or more activities”.
Statistical analysis
Following preliminary descriptive analyses, we employed latent curve modeling with structured residuals (LCM-SR; [41]) using maximum likelihood estimation with robust (Huber-White) standard errors (MLR) and full information maximum likelihood (FIML) estimation to address missing data. In the Supplementary Methods 2, we outline the advantage of the latent curve over the mixed effects modeling framework. Unlike cross-lagged panel models, where between- and within-effects are intermingled, LCM-SR separates between- and within-person effects [42]. This is accomplished by combining the cross-lagged panel model with the latent curve model, and by modeling autoregressive, within-time and cross-lagged effects among the time-specific residuals [41]. Within the LCM-SR, latent growth factors, i.e., intercept and slope are specified to reflect between-person variability. Within-person effects then account for the remaining variability in each observation after modelling the between-person intercept and slope. In other words, within-person cross-lagged effects refer to how individual deviations (represented by the time-specific residuals) from a person’s trajectory (represented by the random intercept and slope) in one domain (e.g., the FI) are related to concurrent and subsequent deviations in another domain (e.g., LS). While between-person effects acknowledge that individuals may differ in both their levels and growth over time due to factors, like sex or educational level, these effects can be confounded with various background characteristics, including genetics, early-life factors, personality, and demographic factors. Within- person effects, on the other hand, control for such stable (un)observable time-invariant confounders [43]. This is a significant advantage of the LCM-SR, addressing a key challenge in non-experimental study designs where controlling for all relevant covariates is not possible, hindering causal effect estimation. Taking a within-person analytical approach can be seen as a step towards uncovering causal effects, as it enables the identification of individual-level dynamics that might otherwise be masked by group-level trends [44].
Statistical analysis comprised three stages. First, we established the optimally fitting model for each outcome variable separately, comparing four models with increasing complexity: (1) a model without any random effects (i.e., only autoregressive effects; e.g., past FI predicts current FI), and subsequently added (2) random intercepts, (3) fixed slopes, and (4) random slopes. Thereby, individuals were allowed to vary around their person-specific levels (model 2) and around their person-specific trajectories (model 4) rather than group-level averages. In all models, we specified the residuals of the observed variables as latent, and added autoregressive paths between adjacent residuals (α, β). To account for the heterogeneous measurement occasions owing to the measurement burst design, we specified one intercept and one slope for each burst (for a similar approach see 45). Model comparison was based on likelihood ratio tests [46].
Second, we combined the best-fitting univariate models to build the bivariate model. This involved adding cross-lagged regression paths from latent residuals in one construct at a specific time to the subsequent latent residuals in the other construct (γ, δ), and allowing latent residuals across constructs to covary within-time (λ). Substantial and statistically significant cross-lagged effects would provide evidence for a causal relationship between the frailty and loneliness, while covarying residuals would instead suggest a common cause of both constructs. A graphical representation of the final model can be found in Fig. 1. Third, we conducted multiple group analysis for sex, age, living alone, and social participation.
Fig. 1. Bivariate latent curve model with structured residuals (LCM-SR) for the frailty index (FI) and loneliness (LS) across waves 1–14. Manifest variables (= computed scores) are represented as rectangles, latent variables as ellipses, and residuals as circles. Single and double headed arrows denote regression paths and covariances, respectively. Paths labeled with numbers index the coding of the intercept and linear slope. Greek symbols indicate that the respective path is estimated freely. RI = random intercept. FS = fixed slope. L = latent variable. R = residual
Model fit was evaluated using robust variants of several fit indices: Tucker-Lewis index (TLI), comparative fit index (CFI), standardized root mean square residual (SRMR), and root mean square error of approximation (RMSEA) with 90% confidence interval. Adequate fit was defined as CFI and TLI ≥ 0.95, and RMSEA and SRMR ≤ 0.05 [47, 48]. Statistical analyses were carried out in R 4.2.3 [49] using the lavaan [50, version 0.6–15] and semTools [51, version 0.5-6] packages.
Results
Sample characteristics
The average age of participants at baseline was 77.0 years (SD = 5.4), 64.6% were female, and 66.0% were living alone. The majority (54.2%) reported a medium level of education, 19.2% reported a low, and 26.5% a high level of education (i.e., A-levels or a university degree). At baseline, 41.5% of participants indicated to take part in at least one social activity, whereby attending clubs emerged as the most frequently selected activity (26.8%). Mean (SD) and median (IQR) of baseline FI and LS were 0.2 (SD = 0.1) and 0.1 (IQR = 0.2), and 3.5 (SD = 1.1) and 3.0 (IQR = 1.0), respectively. The majority of older adults was not frail (67.1% based on the cut-off of the FI ≤ 0.20 [52]) and not lonely (93.4% based on the cut-off of LS score ≤ 5 used in a previous study [53]). Participants completed a median of 13 (IQR = 3.0, range = 1–14) interviews. Additional descriptive statistics of the FI and LS by measurement occasion are shown in Table 1. Pairwise correlations showed a positive association between the FI and LS (see Supplementary Fig. 2), which on average amounted to r = .38 (range = 0.17–0.50). Within construct mean correlation coefficients across waves were r = .83 (range = 0.71–0.94) and r = .64 (range = 0.44–0.87) for the FI and LS, respectively.
Table 1. Descriptive statistics of frailty and loneliness by waveWave n FILS n FI Mean (SD)Median (IQR) n LS Mean (SD)Median (IQR)14264260.19 (0.14)0.15 (0.16)4233.51 (1.08)3 (1)24194190.18 (0.14)0.14 (0.15)4193.40 (0.96)3 (0)34194190.17 (0.14)0.14 (0.14)4183.36 (0.94)3 (0)44104100.18 (0.14)0.14 (0.16)4103.38 (0.92)3 (0)54064060.17 (0.13)0.14 (0.14)4063.42 (0.95)3 (0)64074070.18 (0.13)0.14 (0.15)4063.49 (1.01)3 (1)74064060.18 (0.13)0.15 (0.15)4043.55 (1.06)3 (1)83783770.20 (0.15)0.15 (0.16)3783.49 (1.01)3 (1)93503500.19 (0.14)0.16 (0.16)3503.44 (0.96)3 (1)103563560.19 (0.14)0.15 (0.16)3553.43 (0.98)3 (0)113343340.19 (0.13)0.15 (0.16)3323.55 (1.12)3 (1)123203200.19 (0.14)0.15 (0.18)3203.37 (0.86)3 (0)132902900.20 (0.14)0.16 (0.18)2893.46 (1.02)3 (0)142022020.19 (0.14)0.16 (0.16)2023.47 (1.15)3 (0)Note. FI = frailty index, LS = loneliness, n = total number of participants per wave, nFI = number of participants with valid FI scores, nLS = number of participants with valid LS scores, SD = standard deviation, IQR = interquartile range
Those who dropped out in any wave (N = 264) were not frailer (M_1_ = 0.18, SD_1_ = 0.12 vs. M_2_ = 0.20, SD_2_ = 0.15; t = -1.602, p = .110) or lonelier (M_1_ = 3.40, SD_1_ = 0.85 vs. M_2_ = 3.57, SD_2_ = 1.19; Mann-Whitney-U = 20412, p = .476) at baseline compared to the remaining sample. No significant differences were found (p <. 05) with regard to socio-demographic characteristics, i.e., sex, age, education, living situation.
Univariate models
Parameters and model fit statistics of univariate models for the FI and LS are displayed in Supplementary Tables 3–6. We followed the model building strategy outlined in the method section, starting with a model without any random effects and gradually increasing complexity by adding random intercept and slope factors. This approach reflects previous findings that baseline levels and rates of change vary between individuals [e.g., 1, 10, 54].
For both constructs, model 1 (i.e., a model without any random effects) fit poorly, but adding random intercepts significantly improved model fit (model 1 vs. model 2). For the FI, model fit did not improve further when fixed slopes were added (model 2 vs. model 3), therefore, we did not increase complexity through the inclusion of a random slope (Supplementary Table 4). In contrast, for LS, adding fixed slopes did significantly improve model fit. However, including a random slope did not result in better model fit (model 3 vs. model 4; Supplementary Table 6). Based on the results of the univariate models, we combined the FI model 2 (i.e., random intercepts) with LS model 3 (i.e., random intercepts and fixed slopes) to create the bivariate model.
For the final FI model, we found mostly positive autoregressive effects of small size (see Supplementary Table 3). The model implied intercepts amounted to 0.18 (95% CI = 0.17, 0.19) and 0.20 (95% CI = 0.19, 0.22) for the first and second burst, respectively. Correlation of intercepts was very high (ζ = 0.94, 95% CI = 0.92, 0.97), indicating that older adults with higher frailty levels in the first burst showed also higher frailty levels in the second burst.
Autoregressive parameters for the final LS model, i.e., the within-person stability of LS, tended to show positive, yet weak effects (see Supplementary Table 5). The model implied intercepts amounted to 3.39 (95% CI = 3.30, 3.48) and 3.51 (95% CI = 3.41, 3.61) for the first and second burst, respectively. Average LS changed minimally within bursts and only little between bursts. Correlation of intercepts was again very high (ζ = 0.92; 95% CI = 0.86, 0.98), indicating that participants who were lonelier in the first burst were also lonelier in the second.
Bivariate model
The final LCM-SR yielded good model fit: χ^2^(324) = 700.39, p < .001; CFI = 0.986, TLI = 0.983; SRMR = 0.049; RMSEA = 0.042, 90% CI = 0.029, 0.053. Parameter estimates are shown in Table 2.
As regards the cross-lagged structure, we found weak and mostly positive effects between the FI and LS. Although cross-lagged effects from the FI to LS were greater in magnitude compared to those from LS to the FI, both these within-person effects were negligible in size and the majority of confidence intervals included zero.
Concerning the within-time associations, we found positive, albeit small effects between the FI and LS. That is, individuals who were frailer than usual tended to be also lonelier than usual.
As regards the between-person effects, model implied intercepts amounted to 0.18 (95% CI = 0.17, 0.19) and 0.20 (95% CI = 0.19, 0.22) for the FI, and to 3.39 (95% CI = 3.30, 3.48) and 3.51 (95% CI = 3.42, 3.61) for LS. Average LS exhibited minimal change within bursts and only little change between bursts. Moreover, random intercepts of the FI and LS share a high positive relationship, indicating that frailer older adults were on average also lonelier.
Table 2. Parameter estimates of the bivariate modelParameterEst. [95%CI]Random effects: Means Intercept FI1^^0.18 [0.17, 0.19] Intercept FI2^^0.20 [0.19, 0.22] Intercept LS1^^3.39 [3.30, 3.48] Intercept LS2^^3.51 [3.42, 3.61]Fixed effects: Means Slope LS1^^0.02 [0.00, 0.03] Slope LS2^^-0.01 [-0.02, 0.00]Random Effects: Correlation ζ_1_: Intercept FI1 ↔ Intercept FI20.94 [0.92, 0.97] ζ_2_: Intercept FI1 ↔ Intercept LS10.57 [0.46, 0.68] ζ_3_: Intercept FI1 ↔ Intercept LS20.58 [0.46, 0.69] ζ_4_: Intercept FI2 ↔ Intercept LS10.52 [0.41, 0.63] ζ_5_: Intercept FI2 ↔ Intercept LS20.53 [0.41, 0.65] ζ_6_: Intercept LS1 ↔ Intercept LS20.92 [0.87, 0.98]Autoregressive (FI → FI) α_1_0.26 [0.11, 0.41] α_2_0.29 [0.15, 0.43] α_3_0.28 [0.04, 0.53] α_4_0.08 [-0.10, 0.26] α_5_0.28 [0.10, 0.45] α_6_0.21 [0.04, 0.38] α_7_0.12 [-0.13, 0.37] α_8_0.23 [0.07, 0.38] α_9_0.17 [-0.02, 0.36] α_10_0.11 [-0.23, 0.45] α_11_0.29 [0.07, 0.52] α_12_0.22 [0.02, 0.41] α_13_0.34 [0.08, 0.59]Autoregressive (LS → LS) β_1_0.24 [0.08, 0.39] β_2_0.16 [-0.07, 0.39] β_3_0.14 [-0.13, 0.40] β_4_0.03 [-0.21, 0.28] β_5_0.14 [-0.09, 0.37] β_6_0.26 [0.09, 0.44] β_7_-0.02 [-0.28, 0.24] β_8_0.07 [-0.16, 0.29] β_9_0.06 [-0.23, 0.35] β_10_0.03 [-0.24, 0.29] β_11_-0.14 [-0.40, 0.12] β_12_0.04 [-0.21, 0.29] β_13_0.34 [0.07, 0.61]Cross-lagged (LS → FI) δ_1_0.00 [-0.16, 0.16] δ_3_0.09 [-0.04, 0.21] δ_3_0.05 [-0.10, 0.20] δ_4_-0.03 [-0.17, 0.12] δ_5_-0.05 [-0.19, 0.10] δ_6_-0.03 [-0.15, 0.09] δ_7_0.08 [-0.05, 0.20] δ_8_0.01 [-0.17, 0.19] δ_9_0.03 [-0.15, 0.22] δ_10_-0.02 [-0.20, 0.16] δ_11_0.09 [-0.06, 0.25] δ_12_0.04 [-0.12, 0.20] δ_13_0.08 [-0.08, 0.25]Cross-lagged (FI → LS) γ_1_0.10 [0.00, 0.20] γ_3_0.16 [-0.01, 0.32] γ_3_0.17 [0.00, 0.34] γ_4_-0.07 [-0.26, 0.12] γ_5_-0.04 [-0.20, 0.13] γ_6_-0.08 [-0.20, 0.04] γ_7_0.05 [-0.07, 0.17] γ_8_0.11 [-0.07, 0.29] γ_9_-0.00 [-0.20, 0.19] γ_10_0.07 [-0.14, 0.28] γ_11_0.23 [0.01, 0.45] γ_12_0.05 [-0.17, 0.27] γ_13_0.14 [-0.04, 0.33]Within-time (FI ↔ LS) λ_1_0.23 [0.12, 0.34] λ_2_0.17 [0.05, 0.28] λ_3_0.18 [0.08, 0.29] λ_4_0.14 [-0.03, 0.31] λ_5_0.16 [-0.04, 0.37] λ_6_0.18 [0.03, 0.34] λ_7_0.19 [0.07, 0.32] λ_8_0.07 [-0.08, 0.22] λ_9_0.05 [-0.13, 0.23] λ_10_0.08 [-0.08, 0.24] λ_11_0.10 [-0.08, 0.28] λ_12_0.10 [-0.18, 0.37] λ_13_0.11 [-0.02, 0.25] λ_14_0.09 [-0.06, 0.24]Note. We report standardized parameter estimates and 95% CI for all variables, except for the means of random and fixed effects. The superscript * indicates that unstandardized estimates are reported instead. FI = frailty index, LS = loneliness
Multiple group analysis
Multiple group analysis in terms of sex (men/women), age (70–74 vs. 75–79 vs. ≥80), living alone (no/yes), and social participation (no/yes) was performed on the final bivariate model. In terms of sex, women showed slightly stronger effects than men in the within-person parameters (see Supplementary Table 7). As regards the between-person effects, we found differences in random intercept factors for both FI and LS: women were both frailer and lonelier at baseline.
Concerning age, living situation, and social participation, within-person effects did not differ notably (see Supplementary Tables 8–10). As anticipated, LS and frailty increased with age: Individuals aged 80 years or older exhibited higher values in the FI and LS compared to younger participants. Between-person effects also differed with regards to living situation: Individuals living alone were frailer and lonelier compared to individuals not living alone. In terms of social participation, between person effects also showed differences: Individuals who participated in at least one activity in the past year were less frail and less lonely.
Discussion
The present study aimed at describing the relationship between frailty and loneliness in older adults. It extends previous research by (1) studying short-term dynamics and (2) disentangling between- from within-person effects (i.e., differences manifesting between individuals from processes happening within individuals). The importance of the latter is already recognized in the literature [55] as it allows for studying how changes in one domain predict changes in another at the level of the individual [44].
Using intensive longitudinal data from community-dwelling Austrian older adults, we found that an increase in frailty within a person at a specific point in time is not associated with an increase in loneliness within that person at a later point in time, and vice versa. Although point estimates of cross-lagged parameters of frailty on later loneliness are higher compared to those of loneliness on frailty, their practical relevance is negligible. Thus, these findings do not support a direct link between frailty and later loneliness or between loneliness and later frailty. The slightly greater influence frailty exerts on subsequent loneliness contrasts with findings from a recent study [56], which suggests that changes in an older adult’s health status contribute only minimally to feelings of loneliness. Still our findings on the within-person cross-lagged effects are comparable to those of another recent study [57], which also found that frailty had a stronger impact on loneliness than the reverse across seven waves of the Longitudinal Ageing Study Amsterdam (LASA), with data collected every three years. However, findings from a study conducted in Japan, covering six years with two-year lags between assessments [58] show that, at the within-person level, increasing levels of frailty were associated with subsequent lower levels of social relationships and vice versa. In contrast, findings from Cachón-Alonso et al. [59] using data from the Survey of Health, Ageing and Retirement in Europe (SHARE) suggest another pattern of within-person effects between loneliness and cognitive performance, a domain included in our frailty index. Specifically, loneliness exerted an effect on cognitive domains two years later in adults aged 65+, while the reverse association was more specific: only lower verbal fluency predicted greater loneliness two years later [59].
Second, we found a positive within-time relationship between frailty and loneliness. In other words, we found that within-person increases in frailty coincide with worsening levels of loneliness at the same point in time, again similar to the LASA-study [57]. Additionally, previous studies [58, 59] also found that loneliness and cognitive domains as well as frailty and social relationships share a negative within-person within-time association. While the existence of short-term fluctuations in both frailty and loneliness align with previous studies [27, 38, 60], our findings show that frailty and loneliness go up and down together when measured on a two-week time scale. These fluctuations may be explained by discrete health-related events, such as infections or injuries: For instance, when an older person falls or catches a cold and becomes (temporarily) bedridden or housebound, they are less able to participate in social life; we would expect a decrease in physical health (= increase in frailty) and an increase in loneliness. To examine whether bedrest or falls (serving as proxies for infections and/or injuries) influence the small within-time relationship between frailty and loneliness, we included both proxies separately (as time-varying covariates) in our final model as a supplementary analysis (see Supplementary Tables 11 and 12). This additional analysis revealed that the temporal relationship between frailty and loneliness decreased when these time-varying covariates were included, which suggests that acute health-related events promote both frailty and loneliness, for example via increased pain, fatigue or decreased mobility.
Third, regarding the between-person effects, we found that older adults who show higher levels of frailty also demonstrate higher levels of loneliness at burst one and two, respectively. Taken together, the presence of strong intercept-intercept correlations across constructs along with the absence of cross-lagged within-person relations questions previous findings [23, 61, 62] of a causal bidirectional relationship between frailty and loneliness.
Comparison with previous results proves difficult, however, since the majority of studies conducted in this context either examined the associations separately [e.g., 19], used different health outcomes (e.g., self-rated health [61, 62]), different operationalizations of frailty and loneliness [23, 58], investigated long-term dynamics (over the course of years; e.g., [23, 57–59]), or did not disentangle between-person variability from changes happening within the individual [23, 61–63]. The latter is vital when examining change processes over a period of time as the collected longitudinal data contains information on within- and between-person effects. Traditional cross-lagged panel modeling assumes that individuals vary around the same means as time unfolds and disregards the possibility of trait-like individual differences, hence “it follows that many lagged parameters reported in the literature will not reflect the actual within-person (causal) mechanisms”^(p112)^ [32]. Thus, although previous studies found cross-lagged effects between either frailty or alternative health outcomes and loneliness, we have to keep in mind that these effects intermingled between-person differences and within-person changes, which in turn renders them vulnerable to confounding. Cross-lagged regressions within the LCM-SR, however, separate between- and within-effects, and assess whether higher-than-usual frailty predicts higher-than-usual loneliness (or vice-versa).
Possible reasons for not identifying substantial cross-lagged effects between frailty and loneliness include measurement accuracy. Not directly observable qualities like frailty and loneliness need to be scaled in order to evaluate changes. Yet, the evaluation of changes in frailty and loneliness requires that the scale produces reliable estimates of an individual’s underlying true score. While recent research [37, 38, 64] demonstrates the reliability of the FI and suggests that it is possible to distinguish between frail and robust individuals (between-person effects), one study [38] indicates that the relatively large standard error of measurement (SEM = 0.05) and smallest detectable change (SDC = 0.13) render it difficult to monitor within-person changes reliably. As regards the UCLA loneliness scale employed in the current study, previous studies demonstrated internal consistency [see 65] comparable to our findings (ω = 0.76 vs. α = 0.67–0.88). There is, however, little evidence in terms of test-retest reliability. Although, five studies found adequate test-retest reliability of the full UCLA loneliness scale, no estimates are available for the economic three-item version [66] used in many longitudinal studies on health and ageing (e.g., the English Longitudinal Study of Ageing) and also in the current study.
On the other hand, previous studies reported an association between fatigue, depression, cognitive impairment, and loneliness at an advanced age [67, 68]. Moreover, lonely older adults have been shown to exercise or move less, suffer from malnutrition [69], and experience functional limitations or depressive symptoms [70], characteristics that are closely related to and indeed often included in the frailty index. In the same vein, loneliness has also been cited as a social component frequently included in frailty assessment instruments [71]. In addition to that, recent findings [37, 72] suggest that depression and frailty, and depression and loneliness demonstrate a shared vulnerability. It seems therefore possible that the association between frailty and loneliness may also be due to common causes, e.g., lack of social support or social buffering (e.g., [73–75]). Having found that the random intercepts and the respective correlations, that is, between-person effects, vary by demographic characteristics (i.e., sex, age, living situation, and social involvement), and that frailty and loneliness fluctuate jointly support this assumption. Although our study did not specifically focus on depressive symptoms, their associations with both frailty and loneliness [37, 72], as well as their potential role as a shared vulnerability, warrant further exploration in future studies.
To the best of the authors’ knowledge, this is the first study examining the short-term bidirectional relationship between frailty and loneliness while also disentangling within- and between-person effects. Further strengths of the current study include the data quality and study design. We analyzed intensive longitudinal data of a nation-wide cohort of community-dwelling older adults gathered within a measurement burst design. While the current design is well-suited for capturing short-term fluctuations, it is less effective in assessing long-term developmental trajectories. Nevertheless, this study also has limitations. First, the outcomes used in this study (FI and LS) were based almost exclusively on self-reports. In terms of loneliness, this may have led to an underestimation of its prevalence since loneliness comprises an undesirable and often stigmatized emotional state. We tried to overcome this limitation by using an indirect measurement of loneliness where items do not include the term loneliness. Our FI, on the other hand, included only two objective measures (cognitive tests). As the result of a previous study [76] showed that frailty levels were lower when based solely on self-reports, future research could employ FIs that include more test-based health measures. Second, selection effects and sample attrition were present. In particular, younger, female and well-educated individuals were overrepresented in the sample [38]. Additionally, more than half of the participants were lost during the second burst, although on average, participants provided 13 (out of 14 possible) repeated measurements. We tried to overcome sample attrition by employing FIML, a procedure considering all available information about an individual [77]. Third, a limitation of our analytical approach is that, unlike standard multilevel structural equation frameworks that partition variance into between- and within-group components to compute intraclass correlation (ICC), the LCM-SR decomposes variance into components capturing both systematic individual trajectories and time specific fluctuations [41]. Consequently, the conventional ICC is not applicable.
Conclusion
Disentangling within- and between-person effects is useful when examining the relationship between frailty and LS, and provides the opportunity to explore the potential reciprocal relationship between these two domains in later life. While there was scarce evidence in our study to support such a direct association, it did suggest that frailty and LS may share short- and long-term causes.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vermeiren S, Vella-Azzopardi R, Beckwée D, Habbig AK, Scafoglieri A, Jansen B et al. Frailty and the prediction of negative health outcomes: a meta-analysis. J Am Med Dir Assoc. 2016;17(12):1163.e 1-1163.e 17.10.1016/j.jamda.2016.09.01027886869 · doi ↗ · pubmed ↗
- 2Stolz E, Mayerl H, Godin J, Hoogendijk EO, Theou O, Freidl W et al. Reliability of the frailty index among community-dwelling older adults. Lipsitz LA, editor. J Gerontol Ser A. 2023;glad 227.10.1093/gerona/glad 227PMC 1080905437738215 · doi ↗ · pubmed ↗
- 3R Core Team. R: a language and environment for statistical computing. [Internet]. Vienna, Austria: R Foundation for Statistical Computing; 2023. Available from: https://www.R-project.org/
- 4Jorgensen TD, Pornprasertmanit S, Schoemann AM, Rosseel Y. sem Tools: useful tools for structural equation modeling [Internet]; 2022. Available from: https://CRAN.R-project.org/package=sem Tools
- 5Huxhold O, Henning G. The risks of experiencing severe loneliness across middle and late adulthood. Sneed R, editor. J Gerontol Ser B. 2023;78(10):1668–75.10.1093/geronb/gbad 099PMC 1056188637431978 · doi ↗ · pubmed ↗
- 6Sheftel MG, Margolis R, Verdery AM. Life events and loneliness transitions among middle-aged and older adults around the world. J Gerontol Ser B. 2024;gbad 149.10.1093/geronb/gbad 149PMC 1074526937801643 · doi ↗ · pubmed ↗
- 7Stolz E. F Requent health Assessment In Later life (FRAIL 70+) (SUF edition) [Internet]. AUSSDA; 2024. Available from: https://data.aussda.at/citation?persistent Id=doi:10.11587/DJNOHX