Effects of Deep Sedation With Dexmedetomidine Versus Remifentanil on Postoperative Recovery in Soft Tissue Surgery
Aleksandar M Kishman, Marija V Sholjakova, Andrijan Kartalov, Biljana Kuzmanovska, Albert Lleshi, Marija Jovanovski Srceva, Vesna Durnev

TL;DR
This study compares how two sedatives, dexmedetomidine and remifentanil, affect recovery after soft tissue surgery, finding that dexmedetomidine leads to better outcomes.
Contribution
The study provides new evidence that dexmedetomidine improves postoperative recovery quality compared to remifentanil in soft tissue surgery.
Findings
Dexmedetomidine provides prolonged postoperative sedation and analgesia compared to remifentanil.
Patients with remifentanil required more analgesics immediately after surgery.
Postoperative pain and sedation levels negatively correlate with recovery quality.
Abstract
Background Soft tissue surgery comprises short or medium-duration surgical procedures, with anesthesia consisting of analgesia and sedation. Various quantitative and qualitative recovery scales are used to evaluate the quality of postoperative recovery. The primary objective of this study was to compare the effects of dexmedetomidine versus remifentanil on postoperative recovery using the Quality of Recovery-15 (QoR-15) scale to assess recovery quality in soft tissue surgeries. Methodology This prospective randomized study was conducted at the Clinic of Anesthesia, Reanimation and Intensive Care and University Clinic of Reconstructive and Plastic Surgery, Skopje, Republic of North Macedonia, involving 80 patients. Patients were randomly assigned into two groups, namely, Group 1, sedated with intraoperative dexmedetomidine infusion (Dex, n = 40), and Group 2, sedated with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
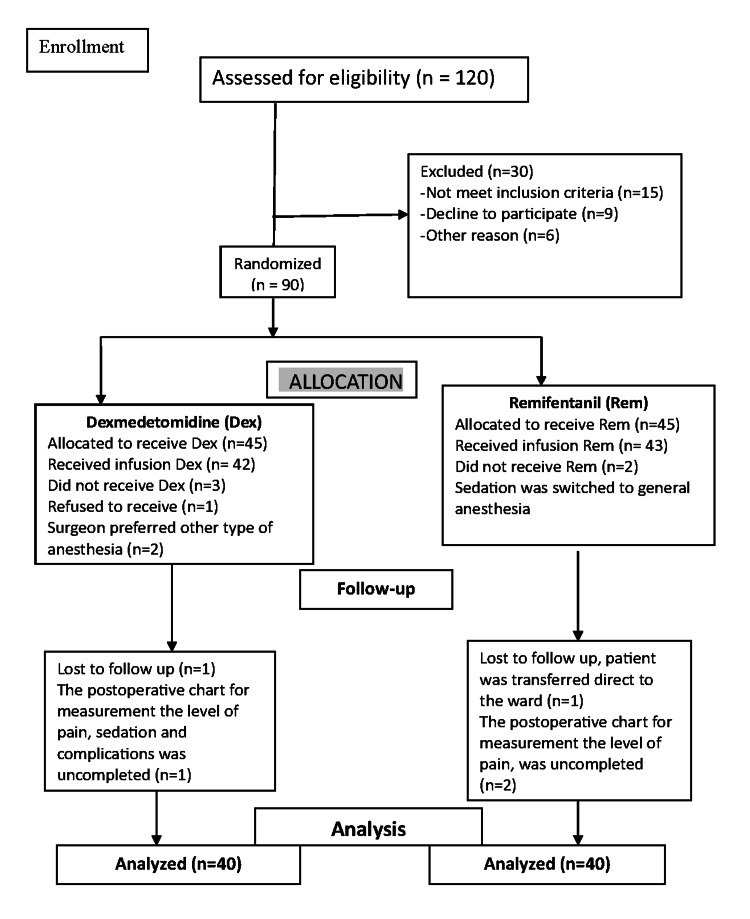 Figure 1
Figure 1| Variables | Dexmedetomidine (n = 40) | Remifentanil (n = 40) | t | P-value |
| Age (years), mean ± SD | 70.633 ± 10.60 | 59.95 ± 12.52 | 0.037923 | 0.969864 |
| Body weight (kg), mean ± SD | 76.85 ± 10.42 | 77.05 ± 11.06 | 0.468141 | 0.641018 |
| Body height (cm), mean ± SD | 170.4 ± 8.59 | 172.825 ± 9.54 | 0.123822 | 0.523395 |
| ASA I, n (%) | 3 (4.5%) | 9 (22.5%) | N/A | N/A |
| ASA II, n (%) | 29 (72.5%) | 25(62.5%) | N/A | N/A |
| ASA III, n (%) | 8 (20%) | 6 (15%) | N/A | N/A |
| Sex, male/female, n (%) | 22/18 (55%/45%) | 18/22 (45%/55%) | N/A | N/A |
| Primary school, n (%) | 2 (5%) | 3 (4.5%) | N/A | N/A |
| Secondary school, n (%) | 19 (47.5%) | 17 (42.5%) | N/A | N/A |
| Higher education, n (%) | 19 (47.5%) | 20 (50%) | N/A | N/A |
| Duration of anesthesia (minutes), mean ± SD | 48.205 ± 11.726 | 50.5 ± 22.3803 | 0.314446 | 0.754057 |
| MAP (mmHg) | Dexmedetomidine (n = 40) | Remifentanil (n = 40) | t- | P-value |
| MAP 0 | 115.47 ± 13.47 | 107.125 ± 12.07 | 0.002 | 0.998409 |
| MAP 1 | 106.77 ± 12.48 | 97.39 ± 10.58 | 0.000343 | 0.999761 |
| MAP 2 | 95.82 ± 14.86 | 88.25 ± 11.72 | 0.007894 | 0.993796 |
| MAP 3 | 88.8 ± 16.19 | 82.65 ± 13.40 | 0.037512 | 0.970182 |
| MAP 4 | 82.95 ± 16.39 | 81.07 ± 12.17 | 0.286392 | 0.775407 |
| MAP 5 | 93.2 ± 14.22 | 85.22 ± 11.64 | 0.004541 | 0.996421 |
| Pulse (beats/minute) | ||||
| Preoperative | 81.22 ± 19.10 | 88.5 ± 16.129 | 0.038281 | 0.969626 |
| 5 minutes after induction | 77.77 ± 1.89 | 82.4 ± 14.134 | 0.090701 | 0.927963 |
| 10 minutes after induction | 73.07 ± 11.89 | 78.3 ± 13.529 | 0.038281 | 0.969626 |
| 15 minutes after induction | 72.6 ± 11.26 | 74.3 ± 12.724 | 0.269492 | 0.788333 |
| 25 minutes after induction | 71.35 ± 11.26 | 73.975 ± 11.591 | 0.148604 | 0.882253 |
| End of surgery | 74.35 ± 12.30 | 75.775 ± 11.419 | 0.301048 | 0.764215 |
| Time | Dexmedetomidine (n = 40) | Remifentanil (n = 40) | t | P-value |
| Preoperative | 14.6 ± 2.747 | 13.7 ± 2.587 | 0.072664 | 0.94231 |
| 5 minutes of surgery | 13.975 ± 1.981 | 13.275 ± 2.368 | 0.082993 | 0.934143 |
| 10 minutes of surgery | 14.15 ± 1.868 | 12.675 ± 2.040 | 0.000757 | 0.999443 |
| 15 minutes of surgery | 13.625 ± 1.870 | 12.3 ± 1.310 | 0.000298 | 0.048981 |
| 25 minutes of surgery | 13.375 ± 1.1776 | 11.9 ± 1.284 | 4.19058E-05 | 0.000073 |
| End of surgery | 13.015 ± 1.969 | 12.175 ± 1.123 | 0.011692 | 0.990774 |
| SpO2 (%) | ||||
| Preoperative | 97.45 ± 1.681 | 99 ± 1.306 | 1.21427E-05 | 0.228335 |
| 5 minutes of surgery | 98.4 ± 1.634 | 98.95 ± 1.146 | 0.046662 | 0.962951 |
| 10 minutes of surgery | 98.55 ± 1.378 | 99.125 ± 0.915 | 0.038281 | 0.969626 |
| 15 minutes of surgery | 98.95 ± 1.324 | 98.925 ± 0.972 | 0.462731 | 0.644868 |
| 25 minutes of surgery | 98.925 ± 1.386 | 98.925 ± 1.021 | 0.5 | 0 .618483 |
| End of surgery | 98.65 ± 1.279 | 98.6 ± 2.173 | 0.451484 | 0.652954 |
| EtCO2 (mmHg) | ||||
| Preoperative | 31.85 ± 2.363 | 33.65 ± 10.31 | 0.14863 | 0.882253 |
| 5 minutes after surgery | 31.725 ± 1.912 | 31.45 ± 2.208 | 0.281564 | 0.779072 |
| 10 minutes after surgery | 31.525 ± 1.912 | 30.9 ± 2.573 | 0.281564 | 0.779072 |
| 15 minutes after surgery | 31.2 ± 1.823 | 30.15 ± 2.504 | 0.281564 | 0.779072 |
| 25 minutes after surgery | 31.722 ± 1.856 | 31.55 ± 2.954 | 0.019909 | 0.984174 |
| End of surgery | 31.625 ± 2.702 | 31.91667 ± 1.331 | 0.385481 | 0.70099 |
| Variable | Preoperative | t-test (p-value) | Postoperative | t-test (p-value) | ||
| Dexmedetomidine (n = 40) | Remifentanil (n = 40) | Dexmedetomidine (n = 40) | Remifentanil (n = 40) | |||
| Leukocytes (×109/L) | 7.43 ± 2.91 | 7.61 ± 2.26 | 0.498091 (p > 0.05) | 7.38 ± 2.861 | 7.61 ± 2.27 | 0.410673 (p < 0.05) |
| Blood glucose (mmol/L) | 5.77 ± 0.90 | 6.15 ± 1.039 | 0.046621 (p > 0.05) | 6.64 ± 0.63 | 7.16 ± 0.73 | 0.002102 (p > 0.05) |
| Blood glucose, dexmedetomidine | 5.77 ± 0.90 | N/A | 6.64 ± 0.63 | 0.0694 (p = 0.94) | ||
| Blood glucose, remifentanil | 6.15 ± 1.039 | N/A | 7.16 ± 0.73 | 3.22422E-06 (p = 0.00184) | ||
| QoR-15 score | 126.41 ± 7.6 | 137.4 ± 3.71 | t = 1.09, p = 0.279 | 92.72 ± 32 | 95.77 ± 32.7 | t = 0.3424, p = 0.7649 |
| Dexmedetomidine (n = 40) | t-test (p-value) | Remifentanil (n = 40) | P-value | t-test (p-value) | |
| Pain scores | |||||
| VAS 0 | 2.475 ± 0.62 | N/A | 1.7 ± 1.328 | N/A | 5.65311E-06 (p < 0.00001) |
| VAS 1 | 2.025 ± 0.71 | 0.069429 (p = 0.944) | 2.25 ± 0.573 | 0.000109 | 2.7558E-11 (p = 0.00728) |
| VAS 2 | 1.675 ± 0.71 | 0.125184 (0.9) | 2.2 ± 0.395 | 0.000000 | 0.5 (p = 0.61848) |
| VAS 3 | 2.47 ± 0.62 | 0.07553 (0.94) | 4.425 ± 2.66 | 0.000000 | 7.46219E-14 (p < 0.00001) |
| Sedation scores | |||||
| RSS 0 | 1.875 ± 0.45 | N/A | 2.70 ± 0.592 | N/A | 0.001225 (p = 0.9990) |
| RSS 1 | 2.025 ± 0.15 | N/A | 2.37 ± 0.817 | N/A | 0.113825 (p = 0.9096) |
| RSS 2 | 1.975 ± 0.15 | N/A | 2.25 ± 0.757 | N/A | 0.000581 (p = 999602) |
| RSS 3 | 1.95 ± 0.308 | N/A | 1.92 ± 0.972 | N/A | 3.2032E-07 (p = 0.0019) |
| Postoperative complications | Dexmedetomidine (n = 40) | Remifentanil (n = 40) |
| Shivering, n (%) | 0 | 0 |
| Nausea and vomiting, n (%) | 0 | 2 (5%) |
| Need for analgesics, n (%) | 4 (10%) | 32 (80%) |
| QoR-15 | Preoperative | Postoperative | ||||
| Questionnaire | Dexmedetomidine | Remifentanil | t-test (p-value) | Dexmedetomidine | Remifentanil | t-test (p-value) |
| Able to breathe easy | 9.60 ± 0.52 | 9.6 ± 0.61 | 0.5 (0.6184) | 7.13 ± 1.3 | 7.5 ± 2.56 | 2.46934E-06 (p = 0.015) |
| Able to enjoy food | 9.61 ± 1.34 | 9.5 ± 0 | 0.296 (0.7680) | 6.54 ± 1.3 | 9.05 ± 0 | 0.08513 (p = 0.93) |
| Feeling rested | 9.55 ± 1.19 | 9.42 ± 0.30 | 0.161 (p = 0.87) | 5.66 ± 1.95 | 7.875 ± 2.3 | 8.49847E-05 (p < 0.000) |
| Have had a good sleep | 8.82 ± 1.53 | 9.15 ± 0.25 | 0.046 (p = 0.96) | 5.94 ± 1.4 | 6.475 ± 1.78 | 2.68864E-12 (p = 0.008) |
| Able for personal hygiene | 9.75 ± 0.89 | 9.55 ± 0.21 | 0.5 (p = 0.61) | 5.47 ± 2.38 | 6.05 ± 1.004 | 5.85501E-09 (p < 0.00) |
| Communicate with family | 8.35 ± 1.56 | 9.15 ± 0.19 | 1.7E-11 (p = 0.86) | 8.59 ± 0.9 | 6.82 ± 0.93 | 8.46084E-06 (p < 0.00) |
| Need medical support | 9.32 ± 0.87 | 9.6 ± 0.18 | 0.048 (p = 0.09) | 8.35 ± 1.0 | 5.25 ± 0.88 | 2.12104E-18 (p = 0.037) |
| Able to return to work | 7.8 ± 1.21 | 8.88 ± 0.17 | 3.8E-08 (p = 0.00) | 4.47 ± 1.95 | 5.82 ± 0.84 | 4.08349E-07 (p = 0.0001) |
| Feeling comfortable | 7.85 ± 1.13 | 9.02 ± 0.16 | 2.27 p = 0.025) | 6.89 ± 1.2 | 5.52 ± 0.80 | 2.47362E-10 (p = 0.015) |
| Feeling of well-being | 8.15 ± 1.38 | 8.37 ± 0.15 | 0.0007 (p = 0.9) | 5.67 ± 1.67 | 5.625 ± 0.77 | 1.14829E-07 (p = 0.254) |
| Moderate pain | 8.15 ± 1.37 | 9.37 ± 0.15 | 2.1E-06 (p = 0.03) | 3.83 ± 1.06 | 5.55 ± 3.09 | 5.01562E-11 (p < 0.000) |
| Severe pain | 9.2 ± 0.97 | 9.82 ± 0.14 | 0.0005 (p = 0.99) | 6.08 ± 1.59 | 5.5 ± 0 | 1.23139E-17 (p = 0.22) |
| Nausea and vomiting | 9.65 ± 0.69 | 9.67 ± 0.14 | 4.56 (p = 0.00) | 8.94 ± 1.02 | 6.45 ± 1.54 | 3.10133E-11 (p = 0.002) |
| Worried and anxious | 7.55 ± 2.08 | 7.72 ± 0.13 | 1.57 (p = 0.12) | 6.81 ± 1.58 | 6.375 ± 1.26 | 0.00079284 (p = 0.99) |
| Feeling sad/depressed | 9.25 ± 1.23 | 8.62 ± 0.13 | 0.01 (p = 0.99) | 7.72 ± 1.11 | 5.9 ± 1.10 | 2.46934E-06 (p = 0.015) |
| Total | 126.41 ± 7.6 | 137.4 ± 3.71 | 1.09 (p = 0.27) | 92.72 ± 32 | 95.77 ± 32.7 | 0.08513915 (p = 093) |
| Preoperative: postoperative | Dexmedetomidine | Remifentanil | 0.0007 (p = 0.9) | Dexmedetomidine | Remifentanil | N/A |
| Variable | Dexmedetomidine (n = 40) | Remifentanil (n = 40) |
| MAP: QoR-15 | r = -0.03933 | r = 0.25036 |
| RRS 0: QoR-15 | r = -0.12268 | r = -0.00967 |
| RRS 1: QoR-15 | r = -0.11723 | r = -0.01855 |
| RRS 2: QoR-15 | r = 0.02012 | r = 0.04089 |
| RRS 3: QoR-15 | r = -0.00341 | r = 0.10229 |
| VAS 0: QoR-15 | r = 0.26969 | r = -0.07177 |
| VAS 1: QoR-15 | r = 0.20386 | r = -0.04049 |
| VAS 2: QoR-15 | r = -0.07855 | r = -0.01441 |
| VAS 3: QoR-15 | r = -0.21731 | r = -0.01855 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Sedative Agents · Anesthesia and Neurotoxicity Research · Intensive Care Unit Cognitive Disorders
Introduction
Soft tissue surgery encompasses a wide range of procedures performed on the body’s surface and soft tissues (skin, muscles, and subcutaneous fat) without affecting the bones, periosteum, internal linings, or organs. Although classified as minor surgery, it presents its challenges. Pain in these regions is often intense, and patients tend to be anxious, scared, and restless, which can impact the surgical atmosphere. An anesthesiologist should decide between general anesthesia and deep sedation with analgesia, with the latter ensuring a safe postoperative course given the nature of the surgery, which typically requires rapid discharge (day surgery).
For this purpose, drugs for intraoperative sedation and analgesia appear to meet the requirements for a calm, pain-free patient during soft tissue surgery. In practice, several agents used alone or in combination are advised in the literature for intraoperative sedation and analgesia. The most used are midazolam or propofol, often combined with fentanyl for analgesia [1].
The properties of dexmedetomidine as a sedative, anxiolytic, and analgesic and remifentanil’s ability to provide effective analgesia-sedation at low doses suggest that these two agents are suitable for use in soft tissue surgery.
Dexmedetomidine is a highly selective alpha-2 adrenergic receptor agonist in the central nervous system. Its sedative effects result from inhibiting neuronal transmission in the locus coeruleus (LC) in the brainstem, while its analgesic effect is attributed to direct central action on the LC [2]. The sympatholytic effect of dexmedetomidine induces hemodynamic changes [3]. Combined with benzodiazepines, opioids (e.g., remifentanil), or propofol, dexmedetomidine enhances sedation, helps maintain hemodynamic stability, and reduces the need for other sedatives [4]. It also influences the endocrine system by decreasing catecholamine secretion and the sympathetic stress response, resulting in an anti-stress effect. This, along with its associated effects, natural awakening, and patient satisfaction, makes it a captivating agent in anesthesiology [5]. It is administered as a bolus infusion over the first 10 minutes, followed by continuous infusion.
Remifentanil is a synthetic opioid and a mu-receptor agonist. It is a potent analgesic that reduces sympathetic nervous system tone and, similar to all opioids, causes respiratory depression. Its rapid onset and short recovery time make it appealing for use in soft tissue surgery, where it is administered as a low-dose infusion for hypnosis and sedation [6].
The decision to be safe for patient discharge following analgesia-sedation is significant. Therefore, the level of recovery after anesthesia and surgery must be evaluated. In practice, various scales are used to assess pain, sedation, or satisfaction levels, such as the Visual Analog Scale (VAS) for pain, the Ramsay Sedation Scale (RSS) for sedation, and scales for anesthesia satisfaction, among others [7,8]. The Quality of Recovery Score-40 (QoR-40) and the modified version QoR-15 measure the quality of recovery following anesthesia or analgesia-sedation [9,10]. These are comprehensive scales assessing the outcomes of sedation, anesthesia, and surgery.
The original QoR-40 postoperative recovery quality scale is a multidimensional tool developed by Myles et al. in 2000 [9,11]. It includes a specific questionnaire with 40 items measuring the following five dimensions: physical comfort (12 items), emotional state (nine items), physical independence (five items), psychological support (seven items), and pain (seven items) [12,13]. While this scale provides detailed measurement of postoperative conditions, its modified version, the QoR-15 scale, developed by Stark et al. (2013), is increasingly preferred for its practicality, requiring just a few minutes to administer [10,14,15]. This questionnaire is divided into the following two parts: section 1 provides the evaluation of physical condition of the patient (10 questions scored from 0 to 10; 0 = very poor, and 10 = excellent postoperative recovery quality); and section 2 presents the mental condition of the patient including pain evaluation. It has five questions scored from 10 to 0 (10 = feeling much, and 0 = not at all). The usefulness and value of this scale has been proven by multiple studies confirming that it represents a comprehensive, patient-oriented measure for recovery after surgery [14-16].
The absence of studies evaluating how and to what extent sedative-analgesic agents contribute to post-anesthetic and surgical recovery, as well as questions regarding their effect on outcomes, present a challenge for every anesthesiologist. The need to address these questions led to this study. To assess the quality of postoperative recovery with the use of dexmedetomidine or remifentanil for sedation/analgesia and to determine which perioperative and postoperative factors influence recovery, a comparative analysis was conducted to correlate these variables with the outcome measure QoR-15.
Materials and methods
This prospective, randomized clinical study was conducted at the University Clinic for Anesthesia, Reanimation, and Intensive Care (CARIC), part of the University Clinic for Traumatology, Orthopedics, Anesthesia and Intensive Care and Emergency Center at the University Clinical Center “Mother Theresa” at the Faculty of Medicine in Skopje, in collaboration with the University Clinic for Plastic and Reconstructive Surgery (UC PRS), from May to October 2024.
This prospective study received approval from the Institutional Ethics Committee. After obtaining written consent, 80 patients who met the inclusion criteria were enrolled in the study. The inclusion criteria were as follows: patients admitted for soft tissue surgical procedures, aged >25 years, with a body mass index (BMI) <35 kg/m², classified as American Society of Anesthesiologists (ASA) Physical Status I-III, who were alert, oriented, and communicative, and who provided written consent to participate in the study. We excluded patients who did not meet the inclusion criteria, had severe cardiovascular diseases (serious heart disease, heart block or atrioventricular block, cardiac arrhythmias, low arterial blood pressure due to dehydration or bleeding, or very high blood pressure), or declined to participate in the study.
Patients were randomly divided into two groups. Group 1 consisted of patients who received a perioperative infusion of dexmedetomidine (Dex) (n = 40), while Group 2 received a remifentanil (Rem) infusion (n = 40). All participants were prepared as outpatients and informed about the study methods for pain assessment (VAS scale) and postoperative recovery evaluation (QoR-15 scale). Additionally, a full blood sample was collected for routine laboratory tests, leukocytes, and blood glucose analysis.
One hour before the intervention, patients received oral premedication with either midazolam 1 mg or diazepam 2.5 mg. Before entering the operating room, they were surveyed using the QoR-15 questionnaire, and continuous hemodynamic and respiratory monitoring was initiated.
For the randomized group receiving dexmedetomidine (n = 40), sedation was induced with an initial bolus dose of 0.9 µg/kg of dexmedetomidine administered for 10 minutes, followed by a maintenance dose of 0.5 µg/kg/hour. In the remifentanil group (n = 40), sedation was induced with a dose of 0.09 µg/kg/minute of remifentanil until patients fell asleep, after which the dose was gradually reduced to 0.05 µg/kg/minute to provide an analgesic effect without impairing respiration.
Intraoperatively, all participants in the study were maintained for safe anesthesia with optimal disturbances of perioperative hemodynamic and respiratory values. Non-invasive methods were used for continuous perioperative monitoring, including electrocardiography (ECG), mean arterial pressure (MAP), heart rate at beats per minute (bpm), blood oxygen saturation percentage (SpO_2_), and the amount of end-tidal carbon dioxide (EtCO_2_). These parameters were recorded at five times during the sedation at 5, 10, 15, and 25 minutes after the start of surgery, as well as at the end of the surgery.
Preoperatively and postoperatively, blood samples were taken to monitor basic markers of inflammation and stress (white blood cell (WBC) count, C-reactive protein (CRP), blood glucose), and the quality of postoperative recovery was assessed using the QoR-15 scale.
Postoperative complications such as shivering, nausea, vomiting, postoperative pain (VAS), and sedation level (RSS) were recorded in four postoperative time intervals, namely, T0 (immediately after awakening), T1 (30 minutes after awakening), T2 (60 minutes after awakening), and T3 (120 minutes after awakening). These findings were compared with the QoR-15 scores obtained for assessing the quality of postoperative recovery.
The results were statistically processed using Microsoft Excel 2011 (Microsoft Corp., Redmond, WA, USA). Average and standard deviation were calculated, and statistically significant differences were assessed using the t-test. Statistical analysis of the correlation between postoperative parameters and the quality of recovery scale was performed using Pearson’s correlation test.
Results
The study included 80 hospitalized patients who underwent soft tissue surgery (Figure 1). Patients were randomly assigned into two groups, each consisting of 40 patients.
CONSORT flow diagram.
To determine the homogeneity between the groups, an analysis of the demographic data of all participants was performed (age, gender, body weight, height, ASA classification, education level, and duration of anesthesia) (Table 1). The average age of the patients in the dexmedetomidine group was 70.633 ± 10.60 years, while the average age of the patients in the remifentanil group was 59.95 ± 12.52 years. The difference in the average age between the two groups was found to be statistically significant (p < 0.05), while no significant differences were observed in the other parameters (p > 0.05) (Table 1).
Table 1: Demographic characteristics of the participants in both groups.Data are presented as mean ± SD and N (%); t = Student’s t-test; p-values <0.05 were considered significant.ASA = American Society of Anesthesiologists
Table 2 presents the values of the perioperative hemodynamic variables, MAP and pulse, measured at the following four time points: MAP 0 pre-operation, MAP 1-5 minutes post-incision, MAP 2-10 minutes post- incision, MAP 3-15 minutes post-incision, MAP 4-25 minutes post-incision, and MAP 5 end of operation.
A significant decrease in MAP compared to preoperative pressure (MAP 0:MAP 1) was noted in both the dexmedetomidine and remifentanil groups (p = 0.00035 and p = 0.004567, respectively), as well as a significant difference in MAP 1, 2, and 5 between the groups (p < 0.05) and no significant difference at 15 and 25 minutes after surgery (p > 0.05). Regarding pulse frequency (bpm), a decrease was observed with a significant difference between preoperative pulse values and after five minutes of administration (p < 0.05), with no significant intergroup differences (p > 0.05).
The perioperative respiratory rate (breaths per minute), blood oxygen saturation (SpO_2_) (%), and end-tidal carbon dioxide (EtCO_2_) values (mmHg) are presented in Table 3. During the measurement times, the respiratory frequency in the remifentanil group decreased, reaching the lower limit of normal values. A significant difference in frequency between the groups was noted at 10, 15, and 25 minutes, and up to the end of the surgery (p = 0.000757, p = 0.000298, p = 4.19058E-05, and p = 0.011692, respectively). Perioperatively, blood oxygen saturation in both groups remained within the normal range. Significant differences between the groups were noted in the preoperative values and five minutes after the start of the surgery. No intergroup differences in EtCO_2_ values were observed at any measurement time.
Table 3: Perioperative respiratory variables in the studied groups.Data are presented as mean ± SD. P-values <0.05 are considered significant.SpO2 = blood oxygen saturation; EtCO2 = end-tidal CO2
As shown in Table 4, there was no significant difference in the preoperative leukocyte count between the dexmedetomidine and remifentanil groups (p = 0.498091), as well as in the postoperative count (p = 0.410673). Blood glucose showed a significant difference between the groups in both preoperative and postoperative periods (p = 0.046 and p = 0.002, respectively). This increase was statistically insignificant in the dexmedetomidine group (p = 0.069), and highly significant in the remifentanil group (p < 0.05).
Table 4: Preoperative and postoperative values for basic markers of inflammation, stress, and recovery score (QoR-15).P-values <0.05 are considered significant.QoR-15 = Quality of Recovery-15
The results of preoperative and postoperative values for recovery score (QoR-15), level of pain (VAS), and sedation scores (RSS) are presented in Table 5. Postoperative pain was measured using the VAS at the following four time points: VAS 0 (immediately after awakening), VAS 1 (30 minutes after awakening), VAS 2 (60 minutes after awakening), and VAS 3 (120 minutes after awakening). The values are displayed in Table 5, along with the sedation scores measured on the RSS at the same time points. The comparison between the two groups showed significantly lower pain scores in the remifentanil group at VAS 0 and VAS 1 (1.7 ± 1.328 and 2.25 ± 0.573, respectively), and significantly higher pain scores at VAS 3 (4.425 ± 2.667). No significant changes in the VAS score were observed in the dexmedetomidine group between the different time points (p = 0.069429, p = 0.125184, and p = 0.075539, respectively). In the remifentanil group, a highly significant difference in pain levels was found across different time points. The measurements of the sedation level showed a statistically significant intergroup difference in RSS 0, RSS 2, and RSS 3 (p < 0.05) (Table 5).
Table 5: Postoperative values of pain (VAS) and sedation scores (RSS).Data are presented as mean ± SD; t = Student’s t-test values; p-values <0.05 are considered significant.VAS = Visual Analog Scale; RSS = Ramsay Sedation Scale
The incidence of postoperative complications, such as shivering, nausea, and vomiting, and the need for analgesics are presented in Table 6. None of the participants experienced shivering. Nausea and vomiting were observed in two participants in the remifentanil group, and the need for postoperative analgesics was recorded in four (10%) patients in the dexmedetomidine group and 32 (80%) patients in the remifentanil group.
The summarized results obtained from the preoperative and postoperative surveys of the participants regarding the quality of recovery are presented in Table 7. There was a small statistically significant difference between the two groups in the preoperative responses (p = 0.09) and a highly significant statistical difference in the postoperative responses (p < 0.05) in almost all responses.
To determine which postoperative factors played a key role in the quality of postoperative recovery, a comparison was made between QoR-15 and MAP, degree of postoperative sedation and pain, and respiratory variables. Pearson’s correlation coefficient was statistically calculated, and the results are shown in Table 8. In the dexmedetomidine group, a positive correlation was found between QoR-15 and RRS 2, the SatO_2_:EtCO_2_ ratio, and VAS 0 and VAS 1 with QoR-15, while in the remifentanil group, a positive correlation was observed between SAP:QoR-15, RRS 2:QoR-15, RRS 3:QoR-15, Sat:EtCO_2_, Sat:QoR-15, EtCO_2_:QoR-15, and VAS 0:QoR-15.
Discussion
The results obtained in this study confirmed the research goals. Dexmedetomidine is a potent analgesic and sedative agent, which, owing to its analgesic properties, rarely requires additional analgesics, as confirmed by this study, making it an ideal agent for use in soft tissue surgery [17]. However, as a sympatholytic agent, it reduces the release of norepinephrine from sympathetic nerve endings; therefore, its effect on the cardiovascular system is dose dependent. At low doses, the central action predominates, manifesting as hypotension and bradycardia, while at higher doses, the peripheral vasoconstrictive effect predominates, which increases vascular resistance during systole, causing hypertension and bradycardia. In this study, the perioperative hemodynamic and respiratory effects of dexmedetomidine and remifentanil were compared. When used at therapeutic doses, both caused a significant drop in systolic arterial pressure (MAP) (p < 0.005), which has also been described by other studies [18]. A significant difference was observed in respiratory effects. Dexmedetomidine does not cause respiratory depression, while remifentanil reduces the respiratory rate, which falls to the lower limit of normal values, as reported by other studies [19]. Perioperative blood saturation in both study groups remained within the normal range. Significant differences between the groups were noted in the preoperative values and five minutes after the start of the surgery (p < 0.005). Safe anesthesia was maintained for all participants in the study, with optimal perioperative hemodynamic and respiratory values.
When analyzing the postoperative values of inflammation markers (leukocytes) and stress markers (blood glucose level), the leukocyte count did not change compared to the preoperative values in both groups. This is explained by the short duration of the interventions and the type of surgical procedures, as well as the need for time for changes in leukocyte count to occur. In contrast, an increase in interleukin 6 (IL-6) was noted in the remifentanil group, but not in the dexmedetomidine group, indicating that IL-6 is a faster marker of inflammation, which confirms that dexmedetomidine has an anti-inflammatory effect. This is consistent with previous studies suggesting the anti-inflammatory properties of dexmedetomidine [20-23].
Preoperative and postoperative quality of recovery was assessed in all patients using the QoR-15 questionnaire, which showed a significant decrease in the immediate postoperative period in both groups. Postoperative complications after general anesthesia and procedural sedation have been intensively researched by many studies. Among the most common are postoperative nausea and vomiting (PONV), shivering, and postoperative pain. Shivering occurs in 20-70% of cases after general anesthesia and is a result of intraoperative cooling during long surgical interventions [24,25]. According to the study by de Boer et al., postoperative occurrence of PONV is associated with the use of opioids during anesthesia and sedation [26]. The results of this study showed that the use of dexmedetomidine and remifentanil in soft tissue surgery with relatively short duration did not cause shivering, while postoperative nausea was noted in two patients in the remifentanil group. This is explained by the opioid properties of the drug, which were successfully managed with the use of antiemetics. Huang et al. (2024) reported a dose-dependent initiation of PONV when using remifentanil [27], which explains the results of our study where a low dose of remifentanil was used.
Postoperative pain, measured using the VAS scale at four time points (T0-T3), showed significantly better analgesia immediately after awakening in patients treated with remifentanil (p < 0.005), which is a result of the analgesic effect of opioids. However, two hours after awakening, patients receiving remifentanil showed a higher level of pain compared to those treated with dexmedetomidine (4.425 ± 2.667 vs. 2.47 ± 0.62). This confirmed the prolonged analgesic effect of dexmedetomidine due to its direct central action on the LC [28].
The level of sedation in the postoperative period, measured using the RSS at four time points, showed a state of unconsciousness such as natural sleep with easy awakening in the dexmedetomidine group. However, a significantly greater sedation was noted in the remifentanil group immediately after the postoperative period and 60 minutes after awakening (p = 0.001225 and p = 0.000581, respectively). The sedative effects of dexmedetomidine are a result of the reduction of neural transmission at the level of the brainstem, leading to a state of unconsciousness like sleep and cooperativeness [29].
To determine which perioperative and postoperative factors influenced recovery during analgesic sedation with dexmedetomidine or remifentanil, a comparative analysis was conducted between the recovery outcomes (QoR-15) and factors such as MAP, blood oxygen saturation percentage, sedation level (RSS), and pain level (VAS). Statistical correlation analysis was performed to determine Pearson’s correlation coefficient. The analysis showed a positive correlation between Sat:EtCO_2_ and RSS 2 in both groups. In the dexmedetomidine group, a negative correlation was observed with MAP at T0, RSS 0, RSS 1, and RSS 3, as well as with VAS 2 and VAS 3. In the remifentanil group, a negative correlation was found with RSS 0 and RSS 1, as well as with all four time points for pain levels from VAS 0 to VAS 3. These findings highlight sedation level and pain level as key factors influencing the quality of postoperative recovery. Specifically, the stronger the pain and the higher the sedation level, the lower the QoR-15 score. This suggests that, for soft tissue surgery, the use of dexmedetomidine allows for same-day discharge after surgery with adequate postoperative observation (around four hours), while patients treated with remifentanil, due to the trend of increasing pain and sedation, should be discharged the following day.
Study limitations
A key limitation of this study was the change from its primary design, leading to the investigation of only the basic markers of inflammation and stress. Furthermore, the study enrolled a small sample, which may hinder the generalization of the results. Future research with larger cohorts and more extensive data will enhance the validity and applicability of our findings.
Conclusions
Based on the results obtained in this study, dexmedetomidine offers a range of pharmacological advantages, providing dose-dependent sedation, sympatholysis, and anxiolysis without a significant respiratory depression. Its side effects are predictable and align with the pharmacological profile of alpha-2 adrenergic receptor agonists. The unique sedative action of dexmedetomidine promises several benefits for anesthesiology practice and can be safely used as a drug for analgesic sedation in short soft tissue surgical procedures. In this study, dexmedetomidine demonstrated a superior performance compared to remifentanil. Hence, in soft tissue surgery, dexmedetomidine ensures hemodynamic stability, shows protective anti-inflammatory and anti-stress effects, provides good postoperative analgesic effects, reduces recovery time, and protects the body from undesirable postoperative complications, such as shivering, severe pain, and PONV.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The effect of low-dose dexmedetomidine on hemodynamics and anesthetic requirement during bis-spectral index-guided total intravenous anesthesia J Clin Monit Comput Park HY Kim JY Cho SH Lee D Kwak HJ 429435302016 https://link.springer.com/article/10.1007/s 10877-015-9735-22616278510.1007/s 10877-015-9735-2 · doi ↗ · pubmed ↗
- 2Short duration large dose dexmedetomidine in a pediatric patient during procedural sedation Anesth Analg Rosen DA Daume JT 686910320061679062810.1213/01.ane.0000216289.52261.5e · doi ↗ · pubmed ↗
- 3Is intraoperative dexmedetomidine a new option for postoperative pain treatment? A meta-analysis of randomized controlled trials Pain Schnabel A Meyer-Frießem CH Reichl SU Zahn PK Pogatzki-Zahn EM 1140114915420132370672610.1016/j.pain.2013.03.029 · doi ↗ · pubmed ↗
- 4Perioperative Applications of Dexmedetomidine Crowe G Dr Atterton B Moran L London World Federation of Societies of Anaesthesiologists 2022 https://resources.wfsahq.org/wp-content/uploads/atow-469-00.pdf
- 5Monitored anesthesia care with dexmedetomidine: a prospective, randomized, double-blind, multicenter trial Anesth Analg Candiotti KA Bergese SD Bokesch PM Feldman MA Wisemandle W Bekker AY 475611020101971325610.1213/ane.0b 013e 3181 ae 0856 · doi ↗ · pubmed ↗
- 6Remifentanil for analgesia-based sedation in the intensive care unit Crit Care Kuhlen R Putensen C 131482003 https://pmc.ncbi.nlm.nih.gov/articles/PMC 420067/1497504010.1186/cc 2421 PMC 420067 · doi ↗ · pubmed ↗
- 7The Canadian four-centre study of anaesthetic outcomes: II. Can outcomes be used to assess the quality of anaesthesia care?Can J Anaesth Cohen MM Duncan PG Pope WD Biehl D Tweed WA Mac William L Merchant RN 430439391992 https://link.springer.com/article/10.1007/BF 03008706159696610.1007/BF 03008706 · doi ↗ · pubmed ↗
- 8Failure of physicians to recognize functional disability in ambulatory patients Ann Intern Med Calkins DR Rubenstein LV Cleary PD 4514541141991 https://www.acpjournals.org/doi/abs/10.7326/0003-4819-114-6-451182526710.7326/0003-4819-114-6-451 · doi ↗ · pubmed ↗