Mature Mediastinal Teratoma Complicated with Spontaneous Rupture into the Pleural Cavity: A Report of a Pediatric Case
Filipa Lima Coelho, Mário Rui Correia, Fátima Carvalho

TL;DR
A pediatric case of a rare mature mediastinal teratoma that spontaneously ruptured into the pleural cavity is reported and reviewed.
Contribution
The paper highlights the rare presentation of spontaneous pleural rupture in a mature mediastinal teratoma.
Findings
The case demonstrates typical radiological features of a mature mediastinal teratoma.
Spontaneous rupture into the pleural cavity is a rare complication of such tumors.
Abstract
Teaching point: This is a review of the typical radiological features of a mature mediastinal teratoma with a rare presentation of spontaneous pleural rupture.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
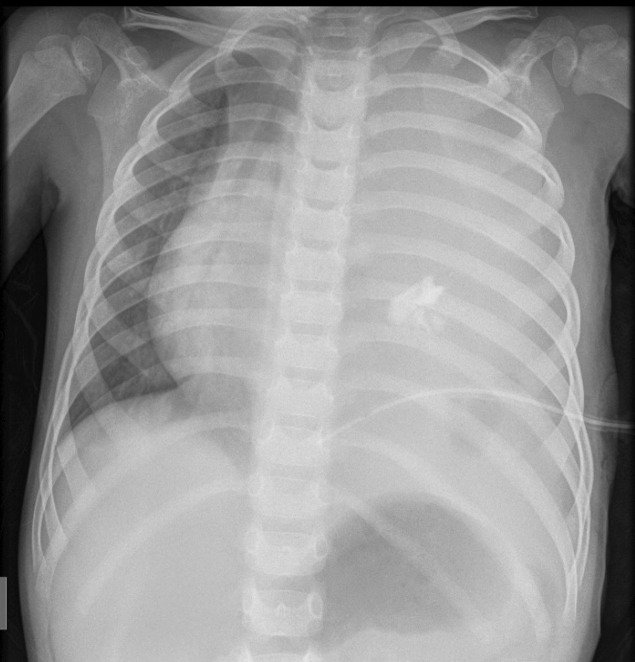 Figure 1
Figure 1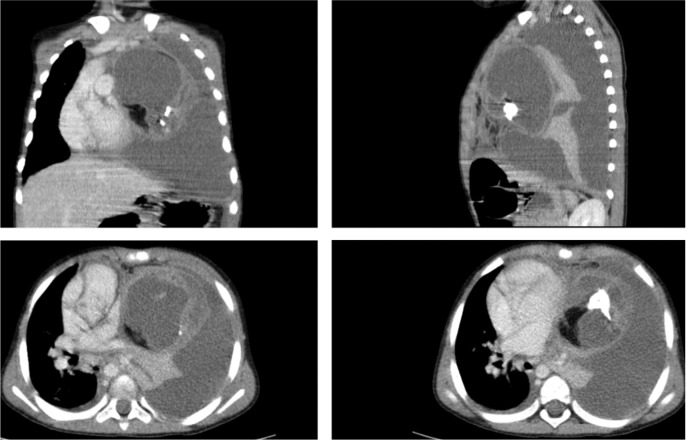 Figure 2
Figure 2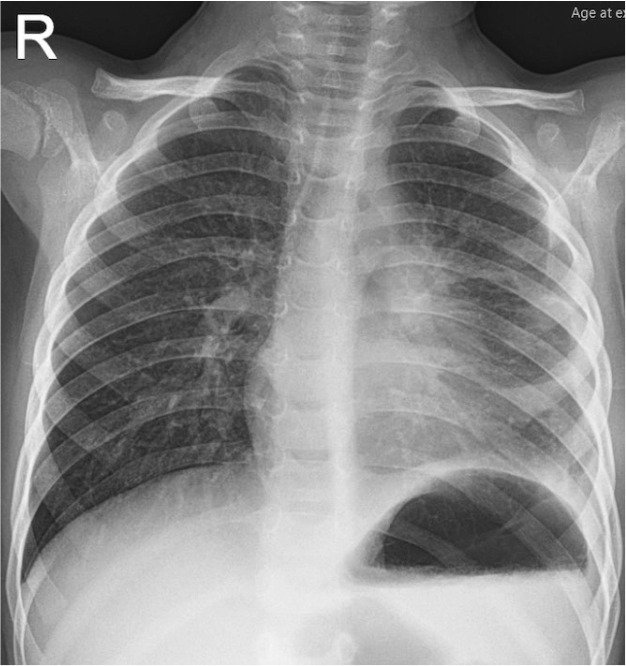 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAppendicitis Diagnosis and Management · Myasthenia Gravis and Thymoma · Teratomas and Epidermoid Cysts
Case History
A 3‑year‑old boy presented with a sudden onset of cough and dyspnea. There was no history of fever, hemoptysis, chest pain, or trauma. Chest radiograph (CXR) showed an opaque left hemithorax, with a significant pleural effusion, loss of the left cardiac border silhouette, and shifting of the mediastinum to the right. Coarse calcifications were visible in the left hemithorax (Figure 1).
Preoperative CXR.
Chest computed tomography (CT) revealed a heterogeneous anterior mediastinal cystic mass, with areas of calcification, soft tissue, and fat density. Also, left‑side pleural effusion and obliteration of the left main bronchus were noted, with left lung collapse (Figure 2).
Multiplanar contrast‑enhanced CT scan.
The imaging features and acute onset of symptoms suggested the diagnosis of a mediastinal teratoma with spontaneous rupture into the pleural cavity.
During hospitalization, a left thoracentesis was performed, with the removal of 100 cc of yellowish fluid, and with clinical improvement. Cultures of the pleural fluid were sterile. Preoperative serum levels of alpha‑fetoprotein were normal.
A left thoracotomy was performed four months later, after pulmonary stabilization with conservative treatment. The anterior mediastinal mass was successfully dissected, measuring 10 cm in its largest diameter.
Pathologic examination showed a unilocular tumor, composed of a variety of tissues from all three germ cell layers, confirming the diagnosis of mature teratoma.
The postoperative CXR showed resolution of pleural effusion and mediastinal mass (Figure 3). The patient fully recovered.
Postoperative CXR.
Comment
Mature teratoma is the mediastinum’s most frequent primary germ cell tumor, containing derivatives of all three germ layers [1].
Complications developing from these tumors are uncommon, and reports of spontaneous rupture of mediastinal teratomas into the adjacent structures, such as the pleural cavity, tracheal tree, pericardium, or lung parenchyma, among pediatric populations, are even rare [1].
The symptoms of a rupture teratoma include acute onset of severe chest pain, dyspnea, and hemoptysis. CXR shows typical findings of a mediastinal mass associated with unilateral pleural effusion [1].
The majority of unruptured mediastinal teratomas appear as a homogeneous encapsulated mass on CT, containing fat, calcifications, soft tissue, fluid, or any combination of these. In contrast, ruptured teratomas demonstrate heterogeneous densities of internal components. Other imaging findings of mediastinal teratoma rupture include pleural effusion, consolidation, or compressive atelectasis of the adjacent lung [1].
CT imaging largely contributes to detection and characterization, appropriate delineation of the mass to the adjacent tissue, such as the lung and pleural cavity, and to the surgical planning of this rare complication of mediastinal teratoma.
Magnetic resonance imaging (MRI) is a valuable alternative to CT for characterizing and delineation of teratomas since fat components are promptly identified as high signal intensity areas on T1‑weighted images that become suppressed with fat saturation.
Surgical management is the optimal treatment for ruptured mediastinal teratoma. Surgery may be complicated due to the leakage of the ruptured components into the thoracic cavity, causing adhesions in the adjacent anatomical structures [1].
The reference list from the paper itself. Each links out to its DOI / PubMed record.