Multicenter observational study of patients who underwent cardiac surgery and were hospitalized in an intensive care unit (BraSIS 2): study protocol and statistical analysis plan
Nair Naiara Barros de Vasconcelos, Renato Carneiro de Freitas Chaves, Carolina de Moraes Pellegrino, Guilherme Martins de Souza, Veronica Neves Fialho Queiroz, Carmen Silvia Valente Barbas, Flávio Takaoka, Ricardo Luiz Cordioli, Sandrigo Mangini, Fabio de Vasconcelos Papa

TL;DR
This study aims to understand the risk factors and complications following cardiac surgery by observing patients in Brazilian intensive care units.
Contribution
The study introduces a multicenter observational protocol to assess postoperative complications and mortality in cardiac surgery patients in Brazil.
Findings
The study will identify risk factors for mortality and severe postoperative complications within the first 3 postoperative days.
It will evaluate the incidence of various severe complications like acute myocardial infarction and septic shock.
The research will describe patient demographics and surgical procedures across multiple Brazilian intensive care units.
Abstract
The perioperative management of patients undergoing cardiac surgery is highly complex and involves numerous factors. There is a strong association between cardiac surgery and perioperative complications. The Brazilian Surgical Identification Study (BraSIS 2) aims to assess the incidence of death and early postoperative complications, identify potential risk factors, and examine both the demographic characteristics of patients and the epidemiology of cardiovascular procedures. BraSIS 2 is a multicenter observational study of patients who undergo cardiac surgery and who are admitted to the intensive care unit. The primary objective is to describe the risk factors and incidence of mortality or severe postoperative complications occurring within the first 3 postoperative days of cardiac surgery or until intensive care unit discharge (whichever event occurs first). Severe postoperative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
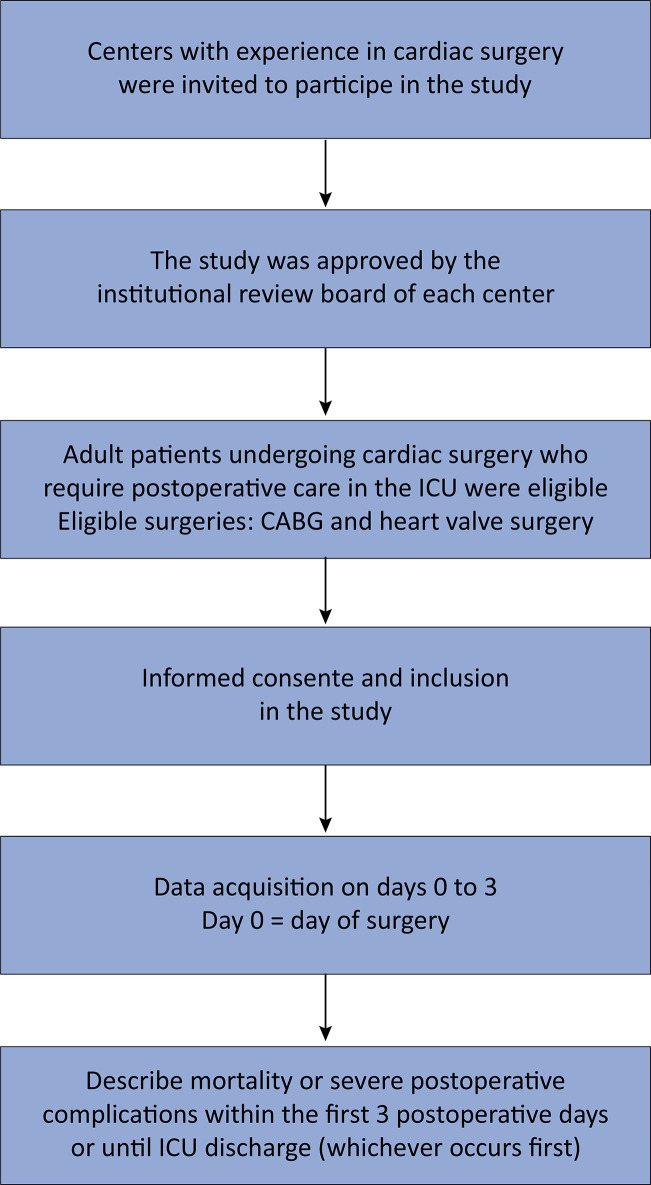 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Hemodynamic Monitoring and Therapy · Sepsis Diagnosis and Treatment
BACKGROUND
Cardiac surgery represents an important therapeutic intervention for patients with various cardiovascular diseases, although it is accompanied by inherent risks and complexities.^(1)^ Both open-heart surgery and percutaneous procedures have become commonplace in contemporary medical practice.^(1,2)^ Despite advancements in surgical and anesthetic techniques, which have contributed to a decreased overall perioperative mortality rate for cardiac procedures, significant challenges continue to persist.^(3-5)^
Whereas cardiac surgery demonstrates potential in improving quality of life and increasing survival rates among patients with cardiovascular disease, it is not without risks and complications.^(4,5)^ The management of patients during the perioperative period is characterized by high complexity and numerous challenges.^(6)^ Factors such as baseline patient conditions, complexities of surgeries, and postoperative complications contribute to elevated in-hospital and postdischarge mortality rates.^(7-9)^ The clinical outcomes of patients undergoing cardiac surgery are closely associated with institutional expertise, thus underscoring the importance of tailored interventions to mitigate the risks of mortality or severe complications.
An understanding of major preoperative risk factors is crucial for optimizing perioperative management and improving patient outcomes.^(10)^ However, there is a notable scarcity of Brazilian data regarding patients undergoing cardiac surgery, thereby highlighting the need for comprehensive studies to enhance the understanding of cardiac surgery risks in this population.
The Brazilian Surgical Identification Study (BraSIS 2) aims to investigate the incidence of death and early severe postoperative complications, identify potential risk factors, and examine both the demographic characteristics of patients and the epidemiology of cardiovascular procedures.
METHODS
Study design and setting
This multicenter prospective observational study was designed according to the guidelines for Good Clinical Practice and the Declaration of Helsinki and was registered at www.clinicaltrials.gov (trial identification number: NCT06154473). The main characteristics of the BraSIS 2 study are summarized in the Synopsis table (Table 1).
Table 1. Synopsis (ClinicalTrials.gov registration, as originally submitted)Data categoryInformationPrimary registration and identification numberClinicalTrials.gov – NCT06154473Date of first registration2023-07-25Financial supportNoneGeneral and academic contactRCFC, MD, PhD, MBA Phone: +55 (11) 2151-1500 E-mail: [email protected] sponsorHospital Israelita Albert EinsteinPublic titleAssessment of patients undergoing cardiac surgery and admitted to the intensive care unit (BraSIS-2)Academic titleAssessment of patients undergoing cardiac surgery and admitted to the intensive care unit: an observational, prospective, multicenter studyCountries involved in recruitmentBrazilHealth conditions/investigated problemsCardiac surgery, intensive care unit care, postoperative complicationsMain inclusion criteriaAdult patients undergoing cardiac surgery requiring postoperative care in the intensive care unit will be included Age: ≥ 18-years-old Sex: both Accepts volunteers: noMain exclusion criteriaExclusive palliative care, advance directive expressing desire for limitation of life support, patients previously included in this study, surgery for implantation of cardiac implantable electronic device and moribund patientType of studyObservational, prospective and multicenter studyExpected date of first inclusionSeptember 2023Sample size500 patientsRecruitment statusNot initiated (expected for 2023)Primary outcomeMortality or serious postoperative complications within the first 3 postoperative days or until ICU discharge (whichever event occurs first)Secondary outcomes− Evaluate patient characteristics − Describe the performed surgeries and anesthesia − Assess intraoperative and postoperative complications − Assess risk factors associated with postoperative complications and mortality
Patient and public involvement
Patients or the public were not involved in the study design.
Patient eligibility
Consecutive patients who meet the inclusion criteria and none of the exclusion criteria will be enrolled in this study. Patients who undergo cardiac surgery and who are hospitalized in an intensive care unit (ICU) will be consecutively included by each of the participating centers during the study period. The patients will be eligible for inclusion in the study during the ICU stay and until the third postoperative day. After the third day following surgery or after discharge from the ICU, the patients will no longer be eligible for inclusion.
Sites and recruitment
Centers with experience in cardiac surgery were invited to participate in this study (Figure 1). At least 10 Brazilian ICUs will be included. The expected recruitment rate is 5 patients/month/site, with a planned study duration estimated at 1.5 years.
Figure 1. Study flowchart.CABG - coronary artery bypass grafting; ICU - intensive care unit.
Inclusion and exclusion criteria
Adult patients aged ≥ 18 years who are undergoing cardiac surgery and who require postoperative care in the ICU will be included. Eligible surgeries include coronary artery bypass grafting and heart valve surgery (both open and percutaneous surgeries/procedures). Patients receiving exclusive palliative care before surgery, patients with advance directives expressing a desire for limitation of life support before surgery, patients who were previously included in the BraSIS 2 study, patients undergoing surgery for the implantation of cardiac implantable electronic devices, and patients in a moribund state will be excluded.
Follow-up
Patients will be followed up until discharge from the ICU or until the third postoperative day (whichever event occurs first) by the health care worker responsible for data collection.
Objectives
The primary objective of this study is to describe the risk factors and incidence of mortality or severe postoperative complications within the first 3 postoperative days or until ICU discharge (whichever event occurs first). Severe postoperative complications include acute myocardial infarction, acute respiratory distress syndrome (ARDS) with partial pressure of oxygen (PaO_2_)/fraction of inspired oxygen (FiO_2_) ≤ 250 (refractory to rescue maneuvers and ventilatory adjustments that persist for more than 1 hour), cardiorespiratory arrest with the return of spontaneous circulation, Kidney Disease Improving Global Outcomes stage (KDIGO) ≥ 2,^(11)^ a new surgical approach being used in an unscheduled event of urgency or emergency, renal replacement therapy, septic shock, severe bleeding, severe hemodynamic instability, stroke, unplanned reintubation, and unplanned use of a circulatory assistance device. The clinical outcomes are presented in mock table 2.
Table 2. Clinical outcomes All patients (n =)Open-heart surgery (n =)Percutaneous surgery (n =)Primary outcomes ICU mortality or severe postoperative complicationsn/Total (%)n/Total (%)n/Total (%)ICU mortalityn/Total (%)n/Total (%)n/Total (%)Severe postoperative complicationsn/Total (%)n/Total (%)n/Total (%)Acute myocardial infarctionn/Total (%)n/Total (%)n/Total (%)ARDSn/Total (%)n/Total (%)n/Total (%)Cardiorespiratory arrest with return of spontaneous circulationn/Total (%)n/Total (%)n/Total (%)KDIGO ≥ 2n/Total (%)n/Total (%)n/Total (%)New surgical approach in an unscheduled event of urgency or emergencyn/Total (%)n/Total (%)n/Total (%)Renal replacement therapyn/Total (%)n/Total (%)n/Total (%)Septic shockn/Total (%)n/Total (%)n/Total (%)Severe bleedingn/Total (%)n/Total (%)n/Total (%)Severe hemodynamic instabilityn/Total (%)n/Total (%)n/Total (%)Stroken/Total (%)n/Total (%)n/Total (%)Unplanned reintubationn/Total (%)n/Total (%)n/Total (%)Unplanned use of a circulatory assistance devicen/Total (%)n/Total (%)n/Total (%)Secondary outcomes Intraoperative complicationsn/Total (%)n/Total (%)n/Total (%)Bronchospasm or difficulties in respiratory supportn/Total (%)n/Total (%)n/Total (%)Extracorporeal circulation output failuren/Total (%)n/Total (%)n/Total (%)Cardiac arrest with return of spontaneous circulationn/Total (%)n/Total (%)n/Total (%)Excessive blood transfusionn/Total (%)n/Total (%)n/Total (%)Length of stay in the ICUn/Total (%)n/Total (%)n/Total (%)Postoperative complicationsn/Total (%)n/Total (%)n/Total (%)Cardiac tamponaden/Total (%)n/Total (%)n/Total (%)Dysrhythmiasn/Total (%)n/Total (%)n/Total (%)Postoperative nausea and vomitingn/Total (%)n/Total (%)n/Total (%)Paralytic ileusn/Total (%)n/Total (%)n/Total (%)Pneumonian/Total (%)n/Total (%)n/Total (%)Pneumothoraxn/Total (%)n/Total (%)n/Total (%)Psychomotor agitationn/Total (%)n/Total (%)n/Total (%)Sustained diarrhean/Total (%)n/Total (%)n/Total (%)Unplanned need for oxygen supplementationn/Total (%)n/Total (%)n/Total (%)ARDS - acute respiratory distress syndrome; KDIGO - Kidney Disease Improving Global Outcomes stage; ICU - intensive care unit.
Acute myocardial infarction is defined by the universal classification of type 5 infarction, which is characterized by an elevation of troponin at 10 times the 99th percentile associated with one of the following changes: the development of new pathological Q waves; newly documented angiographic graft occlusion or new native coronary artery occlusion; or imaging evidence of new losses of viable myocardium or new regional wall motion abnormalities in a pattern that is consistent with an ischemic etiology.^(12)^ Acute respiratory distress syndrome is defined according to the Berlin definition, whereby cases explained by heart failure or volume overload are excluded.^(13)^ Severe bleeding is defined as a decrease of ≥ 2g/dL of hemoglobin or transfusion of 2 units of packed red blood cells without an increase in the hemoglobin value, a decrease in the systolic blood pressure ≥ 10mmHg upon standing, a spontaneous decrease in the systolic blood pressure ≥ 20mmHg, or a heart rate increase ≥ 20 beats per minute.^(14,15)^ Severe hemodynamic instability is defined as norepinephrine ≥ 0.1mcg/kg/min or epinephrine ≥ 0.1mcg/kg/min for more than 2 hours, the independent combination of norepinephrine and epinephrine (regardless of the dose) or an independent combination of norepinephrine and vasopressin.^(16,17)^
The secondary objectives include descriptions of anesthesia and surgical procedures, the incidence of intraoperative complications such as bronchospasms or respiratory support difficulties, failure to separate from cardiopulmonary bypass (at least one failure of the first separation attempt or the need for a circulatory assistance device to exit the operating room), cardiac arrest with the return of spontaneous circulation, excessive blood transfusion (greater than 4 units of packed red blood cells), the incidence of postoperative complications that are not included in the primary outcome such as cardiac tamponade, arrhythmias (including atrial fibrillation, atrial flutter, sustained ventricular tachycardia, supraventricular tachycardia, and ventricular fibrillation), length of stay in the ICU, postoperative nausea and vomiting that is difficult to control, paralytic ileus, patient characteristics, pneumonia, pneumothorax, psychomotor agitation (defined as a Richmond Agitation-Sedation Scale [RASS] score ≥ +2),^(18)^ risk factors associated with mortality, risk factors associated with postoperative complications, sustained diarrhea, and the unplanned need for oxygen supplementation.
Steps and data collection
Local investigators at each participating center will screen all patients undergoing cardiac surgery. Mortality and postoperative complications will be recorded on Day 0 (from the end of surgery until 11:59 pm) and on postoperative Days 1, 2, and 3 (each day from 00:00 to 23:59). Data collection will continue until the day of ICU discharge or until Day 3 for patients who remain hospitalized in the ICU. The start date for each participating center is flexible and will be determined collaboratively with the study coordinator, following approval by the Institutional Review Board of each participating center. The characteristics of the included patients are presented in table 3, the intraoperative data and complications are presented in table 4, the types of performed surgery are presented in table 5, and factors related to the risk of mortality or severe postoperative complications are presented in table 6.
Table 3. Characteristics of the included patients All patients (n=)Open-heart Surgery (n=)Percutaneous surgery (n=)Age (years)Mean ± SDMean ± SDMean ± SDASA scoreMean ± SDMean ± SDMean ± SDMale sexn/Total (%)n/Total (%)n/Total (%)BMI (kg/m^2^)Mean ± SDMean ± SDMean ± SDEUROSCOREMean ± SDMean ± SDMean ± SDSOFA scoreMean ± SDMean ± SDMean ± SDComorbidities Active cancern/Total (%)n/Total (%)n/Total (%)Active endocarditis in use of antibiotic therapy at the time of surgeryn/Total (%)n/Total (%)n/Total (%)Acute myocardial infarction less than 90 days prior to studyn/Total (%)n/Total (%)n/Total (%)Anemian/Total (%)n/Total (%)n/Total (%)Asthman/Total (%)n/Total (%)n/Total (%)Atrial fibrillation or atrial fluttern/Total (%)n/Total (%)n/Total (%)Chronic renal failure on renal replacement therapyn/Total (%)n/Total (%)n/Total (%)COPDn/Total (%)n/Total (%)n/Total (%)Coronary heart diseasen/Total (%)n/Total (%)n/Total (%)Diabetes mellitusn/Total (%)n/Total (%)n/Total (%)Heart failure via the NYHA functional classificationn/Total (%)n/Total (%)n/Total (%)Class In/Total (%)n/Total (%)n/Total (%)Class IIn/Total (%)n/Total (%)n/Total (%)Class IIIn/Total (%)n/Total (%)n/Total (%)Class IVn/Total (%)n/Total (%)n/Total (%)Left ventricular dysfunctionn/Total (%)n/Total (%)n/Total (%)Preserved function (LVEF ≥ 51%)n/Total (%)n/Total (%)n/Total (%)Intermediate function (LVEF 40 - 50%)n/Total (%)n/Total (%)n/Total (%)Reduced function (LVEF 30 - 39%)n/Total (%)n/Total (%)n/Total (%)Very reduced function (LVEF ≤ 29%)n/Total (%)n/Total (%)n/Total (%)Liver cirrhosisn/Total (%)n/Total (%)n/Total (%)Obstructive sleep apnean/Total (%)n/Total (%)n/Total (%)Previous heart surgery (a stay in another hospital)n/Total (%)n/Total (%)n/Total (%)Pulmonary hypertensionn/Total (%)n/Total (%)n/Total (%)Rheumatic fevern/Total (%)n/Total (%)n/Total (%)Systemic arterial @hypertensionn/Total (%)n/Total (%)n/Total (%)Stroken/Total (%)n/Total (%)n/Total (%)Unstable angina for less than 90 daysn/Total (%)n/Total (%)n/Total (%)Laboratory tests before surgery Hemoglobin (g/dL)Mean ± SDMean ± SDMean ± SDCreatinine (mg/dL)Mean ± SDMean ± SDMean ± SDIonic calcium (mg/dL)Mean ± SDMean ± SDMean ± SDGlucose (mg/dL)Mean ± SDMean ± SDMean ± SDBNP (pg/mL)Mean ± SDMean ± SDMean ± SDSD - standard deviation; ASA - American Society of Anesthesiology; BMI - body mass index; EUROSCORE - European System for Cardiac Operative Risk Evaluation; SOFA - Sequential Organ Failure Assessment; COPD - chronic obstructive pulmonary disease; NYHA - New York Heart Association; LVEF - left ventricular ejection fraction; BNP - B-type natriuretic peptide.
Table 4. Intraoperative data and complications All patients (n =)Open-heart surgery (n =)Percutaneous surgery (n =)Anesthesia administeredn/Total (%)n/Total (%)n/Total (%)General anesthesian/Total (%)n/Total (%)n/Total (%)Combined anesthesian/Total (%)n/Total (%)n/Total (%)Total intravenous drugsMean ± SDMean ± SDMean ± SDDuration of the surgical procedure, minutesMean ± SDMean ± SDMean ± SDType of surgery performedn/Total (%)n/Total (%)n/Total (%)Urgent/emergencyn/Total (%)n/Total (%)n/Total (%)Electiven/Total (%)n/Total (%)n/Total (%)Extracorporeal circulationn/Total (%)n/Total (%)n/Total (%)Transfusion of blood productsn/Total (%)n/Total (%)n/Total (%)Red blood cellsn/Total (%)n/Total (%)n/Total (%)Cryoprecipitaten/Total (%)n/Total (%)n/Total (%)Fresh frozen plasman/Total (%)n/Total (%)n/Total (%)PlateletsMean ± SDMean ± SDMean ± SDUrine output (mL)Mean ± SDMean ± SDMean ± SDTotal fluid intake (mL)Mean ± SDMean ± SDMean ± SDCrystalloids (mL)Mean ± SDMean ± SDMean ± SDColloid (mL)Mean ± SDMean ± SDMean ± SDComplications during anesthesian/Total (%)n/Total (%)n/Total (%)Bronchoaspirationn/Total (%)n/Total (%)n/Total (%)Bronchospasm or difficulties in breathing supportn/Total (%)n/Total (%)n/Total (%)Extracorporeal circulation output failuren/Total (%)n/Total (%)n/Total (%)Cardiopulmonary arrest with return to spontaneous circulationn/Total (%)n/Total (%)n/Total (%)Excessive blood transfusionn/Total (%)n/Total (%)n/Total (%)SD - standard deviation.
Table 5. Type of surgery performedOpen surgeryn/Total (%)Valvuloplastyn/Total (%)Aortic valven/Total (%)Pulmonary valven/Total (%)Mitral valven/Total (%)Tricuspid valven/Total (%)Valve replacementn/Total (%)Aortic valven/Total (%)Pulmonary valven/Total (%)Mitral valven/Total (%)Tricuspid valven/Total (%)Type of implanted valven/Total (%)Mechanicaln/Total (%)Biologicaln/Total (%)Revascularization of the myocardiumn/Total (%)Number of bridges performedMean ± SDPercutaneous surgeryn/Total (%)TAVIn/Total (%)ViV-TAVIn/Total (%)Transcatheter treatment of the mitral valven/Total (%)Transcatheter bicaval valves systemn/Total (%)SD - standard deviation; TAVI - transcatheter aortic valve implantation; ViV-TAVI - valve-in-valve TAVI.
Table 6. Factors related to the risk of mortality or severe postoperative complications All patients (n =)Univariate analysesMultivariate analyses OR (95%CI)p valueOR (95% CI)p valueRisk of mortality or severe postoperative complications Factorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueFactorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueRisk of mortality Factorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueFactorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueRisk of severe postoperative complications Factorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueFactorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valuePatients undergoing open-heart surgery Risk of mortality or severe postoperative complications Factorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueFactorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueRisk of mortality Factorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueFactorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueRisk of severe postoperative complications Factorsn/Total (%)OR (95%CI)P valueOR (95%CI)p valueFactorsn/Total (%)OR (95%CI)P valueOR (95%CI)p valuePatients undergoing percutaneous surgery Risk of mortality or severe postoperative complications Factorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueFactorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueRisk of mortality Factorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueFactorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueRisk of severe postoperative complications Factorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueFactorsn/Total (%)OR (95%CI)p valueOR (95%CI)p valueOR - odds ratio; 95%CI - 95% confidence interval.
Data collection and management
Data will be entered using an electronic case report form in the Research Electronic Data Capture (REDCap®, USA) platform by using the internet, with the platform hosted on a server at the Hospital Israelita Albert Einstein, São Paulo, Brazil.^(19,20)^ This system possesses various functionalities, including patient registration, data entry, data validation, data reporting, data quality evaluation, data resolution workflows, audit trials, and data export for statistical analysis.^(19,20)^ Local investigators will directly input data into the system, with comprehensive usage instructions always being available to the investigators. Electronic files will be securely archived on the Hospital Israelita Albert Einstein server in a controlled and confidential environment, and they will be safeguarded by using password protection protocols following best practices.
Regular remote data monitoring will promptly identify irregular patterns, inconsistencies, credibility concerns, or anomalies using predefined queries within the system. Missing or outlier data values will be individually reviewed, and follow-up reports will be regularly reviewed by the coordinating center to ensure consistency and completeness. Efforts will be made to complete or rectify data whenever possible.
Cleaning and locking of the database
The database will be locked once all of the data have been entered, as well as when all discrepancies or missing data have been addressed. If all attempts to resolve the remaining issues are unsuccessful, the database will be considered for locking. Prior to database locking, a thorough review of the data will be conducted. Subsequently, the study database will be locked and prepared for statistical analysis. At this step, access permissions to the database will be revoked for all of the investigators, and the database will be archived.
Auditing
The BraSIS 2 study is subjected to audit by the Einstein Research Integrity Committee at any time, independent of the Institutional Review Board (IRB) and the research team and following the same procedure as any other study performed at Hospital Israelita Albert Einstein (with the study being randomly selected).
Calculation of sample size
We expect to recruit 500 consecutive patients who are undergoing cardiac surgery. Based on previous findings, the incidence of severe complications in the postoperative period of cardiovascular surgeries within the first 3 postoperative days or until discharge from the ICU is approximately 20%.^(21)^ Therefore, by enrolling 500 patients, we aim to develop a robust regression model with up to 10 independent variables. To increase the representativeness of the findings, the maximum number of patients that a single center could enroll in the study was limited to 100 patients. Additionally, there is no limit on the number of patients who undergo open or percutaneous surgery. Patients will be consecutively enrolled, and this approach aims to capture the typical practices in managing patients undergoing cardiac surgery at the participating centers.
Statistical analysis plan
Data will be collected as part of routine clinical care. Patient characteristics will be compared and described using appropriate methods. Continuous numerical variables will be evaluated for distribution patterns via histograms and the Kolmogorov-Smirnov test. Qualitative variables will be expressed as proportions, and quantitative variables will be expressed as the means ± standard deviations or as medians and 25^th^ and 75^th^ percentiles (interquartile ranges), when appropriate.
The number of patients who die or exhibit severe postoperative complications will be reported in absolute numbers and percentages. The primary outcome will be assessed via a multiple logistic regression model. A multiple logistic regression model will be employed to identify the risk factors associated with postoperative complications and mortality. Separate models will be used to identify the risk factors that are specific to postoperative complications and those associated with mortality. Additionally, separate models will also be employed to identify the risk factors that are specific to patients undergoing open surgery and patients undergoing percutaneous surgery. Given the hierarchical nature of the data, all of the models will consider the center as a random effect in the intercept. The relevant covariates that are included in the final multivariable model will be identified as those with p < 0.2 in the univariable model, as well as those covariates with clinical relevance and no statistical associations with other relevant variables.
Minimal missing values for exploratory outcomes are anticipated, as the study procedures include the thorough training of site research staff and independent remote and onsite data monitoring conducted by the study coordinator. Multiple imputation will be performed if the percentage of missing data regarding the core variables exceeds 10%, following standard procedures for multiple imputation using chained equations. For a percentage of missing data ≤ 10%, complete case analyses will be conducted.
Exploratory analysis will be conducted to assess the risk factors that are associated with postoperative complications and mortality. This exploratory analysis will be performed using the paired t test (or Wilcoxon signed rank test for nonnormally distributed data) if a time effect is detected, as well as by using Cox regression; moreover, visualization will be performed using the Kaplan-Meier curve.
After data collection from the last enrolled patient is completed, the database will be cleaned and locked, and the analysis plan will be submitted for publication. The hypothesis tests will be two-sided with a significance level of 5%, and no adjustments of p values will be made for multiple comparisons. All of the analyses will be performed using R software version 4.2.0 or using the most updated version (R Foundation for Statistical Computing, Vienna, Austria).
Subgroups of patients undergoing open surgery or percutaneous surgery will be separately analyzed. Prespecified secondary outcomes and subgroup analyses will not be adjusted for multiple comparisons; therefore, they should be interpreted as exploratory factors. We have prespecified the following risk factor analyses to assess their impacts on mortality and postoperative complications: patients with a previous use of a circulatory assistance device compared to those without prior use, patients with prior uses of vasoactive drugs compared to those without preoperative uses, comparison of the types of utilized cardioplegic solutions, comparison of the types of utilized circulatory assistance devices, influence of cumulative fluid balance, influence of hyperglycemia requiring intravenous insulin, influence of laboratory tests collected during the perioperative period, myocardial revascularization with extracorporeal circulation versus without extracorporeal circulation, impact of cardiopulmonary bypass time, impact of intraoperative use of etomidate, impact of preoperative anemia, impact of the development of anemia during the perioperative period, and impact of the type of infused solution (crystalloid or colloid). Additionally, we will describe the risk factors that are associated with the development of the following postoperative complications: renal complications, pulmonary complications, cardiovascular complications, neurological complications, gastrointestinal complications, hematological complications, new surgical approaches conducted in an unscheduled event of urgency or emergency, sepsis and septic shock, and severe hemodynamic instability.
Collected variables
Demographic data and preoperative, intraoperative and postoperative variables will be collected. During the postoperative follow-up period, variables will be collected in the first three postoperative days or until discharge from the ICU (whichever event occurs first). Data will be recorded using printed clinical forms and/or an electronic form that is specifically designed for the study by utilizing the electronic form REDCap®. Access to the system will be individually provided to each study participant, and this access will be secured via login and password procedures. The authors will be responsible for monitoring the data. The variables that are collected from each patient will be described below.
Randomization
Not applicable.
Ethical considerations
This study will be performed according to national and international guidelines, adhering to the principles of the Declaration of Helsinki and the Act for Medical Research Involving Humans. This study will be approved by the local Research Ethics Committee (Institutional Review Board, or IRB) of the coordinating study center (Hospital Israelita Albert Einstein) (CAAE: 69330823.1.0000.0071), as well as by the local IRB from each center, in compliance with Brazilian legislation. Sites will be required to obtain documentation of proof that the IRB evaluated and approved the study. Any modifications to the protocol that may affect the development, potential benefits, or safety of the study (including changes in the objectives, design, study population, sample size, interventions or relevant management aspects) require protocol amendments. These amendments should be submitted for approval to the IRB of the coordinating center and to all of the IRBs at the participating centers. The need for informed consent is determined by the Institutional Review Board of each participating center.
Safety
Adverse events and interim analyses
Due to the fact that this study is observational and that we do not anticipate inherent risks in its performance, interim analyses are not planned. Adverse events are defined as unwanted events experienced by a patient during the study, regardless of whether they are related to the proposed interventions or not. Although adverse events related to the study are not expected, local researchers, data assistants, and attending physicians are responsible for reporting any such events to the research ethics committee that approved the study.
Patient information and informed consent
The researchers will request written consent from the patient or their legal representative if the patient’s clinical conditions do not allow them to directly provide consent. The proposed informed consent form will be evaluated by each research center, and any necessary changes must be approved by the coordinating center of the study before submission to the IRB. If informed consent is not required by the local IRB, a waiver must be obtained.
Either the investigators at each site or the study coordinator will be responsible for obtaining consent and providing all of the relevant information regarding the study to the patient or their legal representative. The patient (or the patient’s legal representative) and the researcher assigned to obtain consent must date and sign two copies of the informed consent form, with one copy being provided to the patient (or their legal representative) and the other copy being filed with the study documents. Researchers must ensure that patients or their legal representatives understand that participating in the study is voluntary and that they may withdraw from the study at any time without affecting the quality and conduct of the subsequent medical treatment.
Confidentiality of data
The patient and the investigating center will be identified by corresponding numbers on the electronic data collection form to ensure anonymity. The data obtained from medical records must be handled in a confidential manner and stored in cabinets with restricted access by the researchers. Anonymity of all of the data in both provisional and definitive reports will be guaranteed, thereby ensuring that no identifiable information is disclosed. Sites that are involved in the research must securely store all of the data for the duration specified by the study and according to local regulations. After the designated study period has elapsed, data must be securely destroyed to prevent unauthorized access to patient data. However, the team will enact every precaution to ensure data confidentiality throughout the study and beyond.
Publication and administrative aspects
Coordinating center
The coordinating center of the study is the Hospital Israelita Albert Einstein, São Paulo, Brazil. The responsibilities of the coordinating center include planning and conducting the study, preparing the protocol and clinical forms for data collection, developing the operations manual, managing and controlling the quality of the data, performing the statistical analysis, and preparing the final manuscript.
Public disclosure and publication policy
The BraSIS 2 group will publish the study findings regardless of the results. The main manuscript will be submitted on behalf of the research group (BraSIS 2).
Organization
The coordinators will be responsible for recruiting sites and ensuring the proper performance of the study. Local coordinators at each participating center will provide scientific and structural leadership. They will ensure that all of the necessary local ethical and regulatory approvals are obtained before patient enrollment begins. Local coordinators will also train and monitor their respective research teams, thus ensuring the integrity of data collection and the inclusion of data in the electronic medical records.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Serruys PW Morice MC Kappetein AP Colombo A Holmes DR Mack MJ Ståhle E Feldman TE van den Brand M Bass EJ Van Dyck N Leadley K Dawkins KD Mohr FW SYNTAX Investigators Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease N Engl J Med 2009360109619721922861210.1056/NEJ Moa 0804626 · doi ↗ · pubmed ↗
- 2Tsao CW Aday AW Almarzooq ZI Anderson CA Arora P Avery CL Baker-Smith CM Beaton AZ Boehme AK Buxton AE Commodore-Mensah Y Elkind MSV Evenson KR Eze-Nliam C Fugar S Generoso G Heard DG Hiremath S Ho JE Kalani R Kazi DS Ko D Levine DA Liu J Ma J Magnani JW Michos ED Mussolino ME Navaneethan SD Parikh NI Poudel R Rezk-Hanna M Roth GA Shah NS St-Onge MP Thacker EL Virani SS Voeks JH Wang NY Wong ND Wong SS Yaffe K Martin SS American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommitt · doi ↗ · pubmed ↗
- 3Flynn M Reddy S Shepherd W Holmes C Armstrong D Lunn C et al Fast-tracking revisited: routine cardiac surgical patients need minimal intensive care Eur J Cardiothorac Surg 20042511161221469074210.1016/s 1010-7940(03)00608-0 · doi ↗ · pubmed ↗
- 4Dieberg G Smart NA King N Minimally invasive cardiac surgery: a systematic review and meta-analysis Int J Cardiol 20162235545602755748610.1016/j.ijcard.2016.08.227 · doi ↗ · pubmed ↗
- 5Yusuf S Zucker D Peduzzi P Fisher LD Takaro T Kennedy JW et al Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration Lancet 19943448922563570791495810.1016/s 0140-6736(94)91963-1 · doi ↗ · pubmed ↗
- 6Landoni G Augoustides JG Guarracino F Santini F Ponschab M Pasero D et al Mortality reduction in cardiac anesthesia and intensive care: results of the first International Consensus Conference Acta Anaesthesiol Scand 20115532592662128820710.1111/j.1399-6576.2010.02381.x · doi ↗ · pubmed ↗
- 7Nashef SA Roques F Sharples LD Nilsson J Smith C Goldstone AR et al Euro SCORE II Eur J Cardiothorac Surg 20124147347442237885510.1093/ejcts/ezs 043 · doi ↗ · pubmed ↗
- 8Edwards FH Clark RE Schwartz M Coronary artery bypass grafting: the Society of Thoracic Surgeons National Database experience Ann Thorac Surg 19945711219827987710.1016/0003-4975(94)90358-1 · doi ↗ · pubmed ↗