Correlations between family characteristics and childcare in optimizing the growth of children under six years
Laili Rahayuwati, Desy Indra Yani, Sri Hendrawati, Arlette Suzy Setiawan, Damar Irza, Sherllina Rizqi Fauziah

TL;DR
This study explores how family traits like education and media exposure affect childcare quality for children under six in Indonesia.
Contribution
The study identifies specific family characteristics linked to better childcare practices in Indonesia.
Findings
Parents' education and health media exposure correlate with better childcare.
Families without health insurance and those with more than two young children show improved childcare patterns.
Parental age between 20–34 years is associated with better childcare outcomes.
Abstract
Families have a the primary influence on children. In particular, excellent childcare in the family is assumed to correlate with children’s health status, growth, and development. Hence, some family factors contribute to the optimization of childcare. This study aims to analyze family characteristics that correlate with childcare for children under six in Indonesia. The data collection instrument used was a Performance and Accountability Survey Program (SKAP) questionnaire of the National Population and Family Planning Board for Indonesia to assess family function in children’s health development in a sample of 7,651 parents, mothers, and/or fathers of children under six years of age. Childcare was the outcome variable. In addition, the chi-square test and logistic regression were used for statistical analysis. The results showed a significant correlation between parents’ education,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
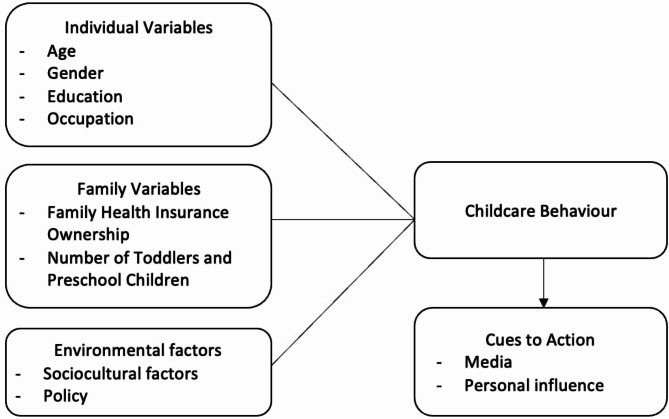 Figure 1
Figure 1- —University of Padjadjaran
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Nutrition and Water Access · Public Health and Nutrition · Breastfeeding Practices and Influences
Background
Family is an element that can directly correlate with the status of individual health, especially that of children [1]. The family is a provider of economic, social, and psychological resources and serves to protect it from health threats. Family is the primary influence on children, included in many preschool children. According to Duvall’s 1962 theory, there are eight stages in the family life cycle, with the third stage being families with preschool children, where the oldest child is between 2 ½ and 6 years old [2]. Family factors, such as resources and parenting patterns that shaped healthy lifestyles in the past, influenced lifestyles later in life [3]. In addition, environmental and family factors can influence the behavior of parents and children. Specifically, family characteristics, including access to socioeconomic resources, such as education level and income, are associated with differences in parenting styles for childcare. As such, parents with educational backgrounds below high school, lack of support, and lack of resources are more likely to have authoritarian and permissive parenting styles [4]. Higher income, scholarly performance, and financial improvement determine the shape of childhood development [5]. Work-life balance, time spent caring for children, and the presence of chronic illness are independent predictors of parent-child relationships [6]. Therefore, family care is also a crucial factor in health, especially in meeting nutritional needs, to improve children’s health status and growth [7].
Parental childcare is a factor associated with the nutritional status of families [8]. Since Indonesia has a 21.6% prevalence of stunting, the country’s government has directly focused on childcare and nutritional status and has produced several instructions to optimize child growth [9]. Excellent childcare must follow an overview of the nutritional status of toddlers and be an instrument for monitoring and evaluating the achievement of specific indicators and interventions issued by the Health Research and Development Agency of the Ministry of Health. The Indonesian Nutritional Status Survey [Survey Status Gizi Indonesia (SSGI)], which applies to provincial and city/district levels, was started in 2019 and will continue until 2024. These specific nutritional indicators include prenatal checks, routine and complete basic immunizations, monitoring of toddler growth, administration of iron supplement tablets for pregnant and young women, access to medicines by toddlers, and provision of additional food to toddlers and pregnant women. Optimal nutritional status will be obtained by children when they have easy access to nutrient-rich food, adequate healthcare services, and a healthy environment [10], especially at 1000 days of fetal life [11, 12]. Complementary breastfeeding supports healthy growth and development [13]. Poor complementary feeding has been identified as a risk factor that is directly related to nutritional problems [14]. A systematic review also showed that childcare is related to growth. There is a positive association between childcare attendance and growth, including an association with stunting [15].
There are many risk factors believed to be the causes of nutritional problems, which occur at several levels, namely, community, family, household, and individual levels [16]. At the community level, the causes are inadequate health services, environmental cleanliness, and little clean water. Causes at the family level include economic factors, nutrition, and parenting style. Causes of individual elements included history of infectious diseases, history of weight, low birth weight, and maternal nutritional status during pregnancy [17]. Therefore, child development outcomes are related to parental knowledge, attitudes, and practices in managing family health and nutrition [18]. Another study on similar issues revealed that family income, ethnicity, or age differences may contribute to differences in childcare [19]. In particular, healthy parenting measures the extent to which parents play a role and function in carrying out their duties and responsibilities to provide good health status for their children. The description of the concept used in this study is based on the Health Belief Model, as shown in Fig. 1.
Fig. 1. Conceptual framework
Multidisciplinary professionals conducted the SKAP survey. However, the large amount of data acquired was only used for social sciences research. Hence, specific explanations of childcare, psychology, and public health aspects have not been explored much. However, issues of stunting and malnutrition require extensive support from national-level data, such as the SKAP data survey. These data can be used to describe how childcare is influenced by various family characteristics, such as parents’ educational background, employment, insurance ownership, gender, age, number of children, and media exposure to child health. Therefore, this study aimed to analyze the relationship between family characteristics and childcare in children under six years of age based on secondary data.
Methods
Study design and setting
This research was conducted by the National Population and Family Planning Board for Indonesia in a cross-sectional manner, using secondary data from the Performance and Accountability Survey Program (SKAP) in 2019. The second paragraph explains the procedure for collecting primary data, and the third paragraph explains the secondary data used in this study.
SKAP is a survey and national research conducted by the National Population and Family Planning Board for Indonesia through the Center for Research and Development for Family Planning, Prosperous Families, and Population to measure the success of the family and population development programs that have been carried out. While collecting primary data, the sampling methods used were probability-proportional to size (PPS) and systematic random sampling. First, PPS sampling was used with the number of households, which resulted in household listings. PPS is a method for selecting cluster samples proportionally, considering differences in the number or size of each target. Here, “size” refers to the number of households to be included as samples. The PPS method is also used to determine both the selected cluster and its location. A cluster, in this context, is a group of adjacents adjacent census blocks, located in one area and consisting of an average of 200 households. This cluster forms part of a village or ward area with identifiable administrative boundaries. The household listings were then selected by systematic random sampling to be chosen as respondents. Households identified during data collection that meet the minimum requirement of consisting of at least one family are considered eligible. In each cluster, 35 eligible households will be interviewed. Single-person households or those that do not meet the family requirement are excluded from eligibility.
Data were collected through door-to-door interviews with the selected respondents using the SKAP questionnaire, which included questions about child growth and development. The survey was conducted in 34 provinces of Indonesia. In addition, no respondent received any intervention. Therefore, the results of the survey represent data at the Indonesian national level [20]. The data were approved by the National Population and Family Planning Board for Indonesia Ethical Review Institutions (number 454/LB.02/H4/2019).
This study uses secondary data for analysis based on the survey data obtained. The family criteria in this survey refer to Law No. 52 of 2009, concerning population and family development, the smallest unit in a society consisting of husband and wife, husband and wife with their children, fathers with their children, and mothers with their children (Undang-Undang Republik Indonesia, 2009). The family respondent sample comprised all families on the list of selected household members. Based on SKAP survey data, this research focuses on the two most populous provinces in Indonesia, namely West Java and Banten, with a total of 10.731 respondents’ data collected. Missing data occurred when respondents did not fill the answer column; therefore, only complete data were used for analysis. Thus, 102 respondents were excluded from the study. After being selected with research criteria, a total of 7.651 respondents in the secondary data were analyzed in this study.
Participants
The respondents in this study were families in all provinces of Indonesia. In detail, the inclusion criteria of the respondents were couples of childbearing age families, reproductive age, or Pasangan Usia Subur (PUS) who were or had ever engaged in caring for children under six, with a minimum age of 14 years. There were no exclusion criteria for this study.
Variables
Two types of variable were used in the analysis. Childcare was the dependent variable. In this study, childcare was defined as the care provided by parents. The seven indicators of SKAP were adapted from the practice of caring for the growth and development of children and toddlers, knowledge, and information related to family functioning. These indicators formed the instrument in the form of a questionnaire. The answer choices for these questions were yes and no. Indicator values of 0 to 2 yes answers indicated fairly childcare, while 3 to 7 indicated good childcare provision. Those indicators were asked to be answered based on the parents’ experience of providing caregiving to children, without considering the number of children or the child.
The independent variables in this study were family characteristics, such as age, gender, education, occupation, and media exposure to children’s health, as well as family aspects such as health insurance ownership and the number of toddlers and preschool children. Respondents of this study were only one of the parents or a respondent who represented the family parenting pattern in the household and who were available for the survey interview. In addition, media exposure is defined as the history of knowing about the national family program through health officer visits, television, posters, or other media exposures. The family health insurance ownership question asked was the BPJS National Health Insurance. Additionally, the number of toddlers under six entails the history of all respondents having children under six. Those with children more than six years old were categorized as no toddlers or children of preschool age, and they were asked a retro question to review their experience of having children under six.
Statistical analysis
Univariate and bivariate data analyses were performed using data-processing software. Because this study has a large volume of data produced, the researcher used STATA software. This is intended so that the analysis process can be carried out optimally. Univariate analysis was carried out using the frequency distribution method, describing family characteristics and caring for children under six years in frequency (n) and proportion (%). In this analysis, the 75th percentile was used to justify the conditions of the studied variables. Bivariate analysis was performed using the chi-square test (X^2^) to assess the relationship between childcare upbringing and distinct family components. Other analyses were performed using the multivariate logistic regression method to estimate the magnitude of the probability of a particular event as an explanatory function. A multivariate regression model is a regression model with more than one correlated response variable and one or more predictor variables (OR [95% C.I]). We conducted the analysis using statistical software and then looked for a connection between variables. In this case, the possible childcare factors were determined based on family characteristics. In addition, we analyzed the data guided by the National Population and Family Planning Board’s framework of children’s growth and development, which explains the importance of monitoring children’s growth and development from the perspective of physical growth, development, and mental-emotional aspects [21].
Results
Based on the participants’ baseline data, Table 1 shows the results of the distribution of family characteristics from a total of 7.651 households with couples of childbearing age families (PUS) samples. The highest age category, namely 2,504 samples (32.7%), was 35–49 years. This range is considered an adult and productive age category. Most of the data showed the last education category attended was primary school, comprising 3,158 samples (41.3%), and 4,208 (55%) of the sample were employed. Conditions also show that 7,415 samples (96.9%) have less than two children under six, while only 4,735 (61.9%) samples have insurance. The exposure of the sample to media that provides information about stunting is dominated by the range of 1–5 types of media, or approximately 7,138 (93.3%) of the total sample. It can be seen in Table 1.
Table 1. Baseline Data of participants (n = 7.651)Family CharacteristicsFrequencyPercentage Parents Age < 1980510.5%20–342.30930.2%35–492.50432.7%> 502.03326.6% Parent’s Gender Male3.91051.1%Female3.74148.9% Parent’s Education Never and not yet in school1361.7%Primary School3.15841.3%Junior High School1.44218.9%Senior High School2.25129.5%D1/D2/D3/Academy1932.5%College/University4716.1% Parent’s Occupation Employed4.20855%Unemployed3.44345% Family Health Insurance Ownership Don’t have insurance2.91638.1%Have insurance4.73561.9% Parent’s Media Exposure Related to Children’s Health Not exposed to media1241.6%Exposure to 1–5 types of media7.13893.3%Exposure to 6–10 types of media3434.5%Exposure to 11–15 types of media460.6% Number of Toddlers and Preschool Age Children (< 6 years) < 2 children7.41596.9%> 2 children2363.1%
Table 2 shows the results of the Pearson Chi-square analysis, which states a significant relationship between the variable components of family characteristics: age (ρ = 0.000), education (ρ = 0.000), health family insurance (ρ = 0.010), number of toddlers and pre-school age (ρ = 0.000) and media exposure to health information (ρ = 0.001), with childcare. With the highest category percentage that has an impact on good childcare, there were found that parents aged 20–34 years were 807 (34.9%) respondents, do not have family health insurance were 626 (21.5%) respondents, exposure to 11–15 types of media related to children’s health were 12 (26.1%) respondents and had > 2 children were 159 (67.4) respondents. However, in contrast to other family characteristic components, gender (ρ = 0.497) and occupation (p = 0.370) have no relationship with childcare in children. It can be seen in Table 2.
Table 2. The correlation between family characteristics and childcare (n = 7.651)Family CharacteristicVariableChildcare Chi-Square GoodFairlyFrequency (n)Percentage (%)Frequency (n)Percentage (%) Parent’s Age (years) < 199812.2%70787.8%0.00020–3480734.9%1.50265.1%35–4959023.5%1.91476.5%> 50331.6%2.00098.4% Parent’s Gender Male76919.7%3.14180.3%0.497Female75920.3%2.98279.7% Parent’s Education Not yet in school85.9%12894.1%0.000Primary School47515.05%2.68384.95%Junior High School38026.4%1.06273.6%Senior High School50122.3%1.75077.7%D1/D2/D3/Academy5126.4%14273.6%College/University11324%35876% Parent’s Occupation Employed85620.3%3.35279.7%0.370Unemployed67219.5%2.77180.5% Family Health Insurance Ownership Don’t have insurance62621.5%2.29078.5%0.010Have insurance90219%3.83381% Parent’s Media Exposure Related to Children’s Health Not exposed to media86.4%11693.6%0.001Exposure to 1–5 types of media1.42920%5.70980%Exposure to 6–10 types of media7923%26477%Exposure to 11–15 types of media1226.1%3473.9% Number of Toddlers and Preschool Age Children (< 6 years) < 2 children1.3697.9%6.04692.1%0.000> 2 children15967.4%7732.6%^*^ Condition of child caring for the growth and development of children is based on the 75th percentile justification
The results of the multivariate analysis showed that variables had a significant effect on childcare at a significance level of 10% (α = 0.10), except parental education. The analysis indicated that as age increased, childcare improved, with the odds of the good childcare are 3.515 times greater at the age of 20–34 years compared to the odds for those who were in the age of 14–19 years old (95% CI: 2.78–4.44, p-value = 0.000). Regarding parental educational background, the analysis showed that while parental education was not significantly associated with childcare, it still had exhibited a positive correlation. Our research finds that families without insurance have a better chance of doing good childcare compared to families who have insurance (OR: 0.853, 95% CL: 0.75–l0.96). Media exposure also plays a role, as parents who are more exposed to media tend to provide better childcare about children’s health than those with limited or no exposure to media. The optimal condition was observed among those exposed to 11–15 types of media, with an odds ratio (OR) of 2.919 (95% CI: 1.01–8.38, p-values = 0.047). Furthermore, parents with more than two toddlers and pre-school age (< 6 years old) exhibited better childcare than those with fewer than two toddlers and preschool-age, including none at all, with an odds ratio (OR) of 5.612 (95% CI: 4.20–7.48, p-value: 0.000) times the odds for those who were have less than 2 children. The results are presented in Table 3.
Table 3. Logistic regression of good childcare by potential Associated factors (n = 7.651)Family characteristicOR[95% C.I] p LowerUpper Parents Age *<1920–34 3.515 2.7814.4420.00035–492.1681.7052.7570.000> 500.1290.0850.1950.000 Parent’s Education *Never went to schoolPrimary School1.3600.6312.9290.432Junior High School1.6110.7443.4860.225Senior High School1.4240.6603.0750.367D1/D2/D3/Academy1.8830.8174.3380.137College/University1.5070.6803.3380.311 Family Health Insurance Ownership *Don’t have insuranceHave insurance0.8530.7530.9660.013 Parent’s Media Exposure Related to Children’s Health *Not exposed to mediaExposure to 1–5 types of media2.4681.1495.2980.020Exposure to 6–10 types of media2.3761.0595.3320.036Exposure to 11–15 types of media2.9191.0168.3830.047 Number of Toddlers and Preschool Age Children (< 6 years) <2 children> 2 children5.6124.2097.4810.000Base categories
Discussion
Factors significantly related to childcare in the present study were parents’ age, education, family health insurance ownership, media exposure related to children’s health, and the number of toddlers and preschool children. Most studies report each component of childcare separately, such as nutrition and immunization, rather than childcare as a single variable. However, parents are an important part of the adult population because they are in charge of their health of their children. Child care consists of providing children with balanced nutrition, immunizing children, providing breast milk and vitamins, treating children when sick, and teaching children healthy behaviors.
Parent education correlates with children’s nutrition by imparting literacy and skills and exposing prospective parents to health information and knowledge [22]. In this research, parental education showed a positive correlation with childcare, and media exposure to health (11–15 types of media) showed a better childcare in children. In addition, parents’ high level of health literacy was linked to healthy habits in their children, such as eating better, brushing their teeth more often, and being more active. Children under age 11, whose parents had high health literacy, consumed more vegetables, salads, and fruits than other children [23]. Dietary and physical activity patterns typically develop during childhood and persist throughout adulthood. Thus, it is crucial to develop health-promoting lifestyle patterns at an early age to promote lifelong health and to reduce the risk of lifestyle-related chronic diseases.
Health-conscious parents were more likely than non-health-conscious parents to view their child’s diet as an essential contributor to future health. Childhood diet influences the risk of developing a preference for unhealthy foods, being overweight, having poor growth and development, and developing diabetes. Parents’ health consciousness influences their perspectives and behaviors regarding their child’s nutrition and health [24].
Immunization safeguards children from infectious diseases that can be fatal. However, parental vaccination non-adherence remains high. Significant correlations were found between infant immunization practices and parental education, primary school, secondary school, and higher education, and parents who had adequate knowledge of infant immunization [25]. The factors associated with immunization adherence include vaccination-related knowledge, employment status, educational level, economic status, and family size [26]. In addition, male parents, parents who did not know anyone who had personally experienced severe side effects from any vaccine, and parents who did not believe vaccines were effective methods to protect communities from disease were significantly less likely to have vaccinated their offspring than female parents, those who knew someone who had, and those who believed that vaccines were an effective means of protecting communities from disease [27]. Incomplete immunization mothers were young, single, had secondary education, poor, and primiparous [28]. There was a significant correlation between immunization non-compliance and parental age, source of information, education, and occupation [29]. Mothers’ compliance with child immunization was correlated with their marital status, knowledge, and attitude toward immunization. Knowledge of the mother was the most accurate predictor of immunization compliance [30]. Vital to a successful child immunization program is the knowledge gained through appropriate health education from health workers regarding immunization, which will correct misconceptions and provide accurate facts and a thorough understanding of child immunization.
Exclusive breastfeeding is provided for infants for the first six months and then continuing breastfeeding for up to two years while gradually introducing other meals suitable for their age. In Indonesia, exclusive lactation is positively influenced by mothers’ level of education [31]. Indicators of exclusive breastfeeding included the household affluence index and the mother’s occupation [32]. A total of 52.3% of infants were exclusively breastfed, and the likelihood of exclusive breastfeeding significantly increased with parity, antenatal care visits, early initiation of lactation, low-income households, and living in rural areas [33]. In contrast, exclusive breastfeeding was linked to a mother’s lack of formal education, monthly income under $100, female children, absence of antenatal guidance on exclusive nursing, and lack of husband support [34]. In addition, working status, cesarean delivery, and cesarean section were associated with a decreased likelihood of exclusive lactation [33]. Interventions to promote breastfeeding in Indonesia should pay particular attention to women who are vulnerable to breastfeeding and should also be encouraged by nutrition-sensitive programs such as postpartum care and smoking cessation. Given the individual and social context, breastfeeding promotion strategies should emphasize increasing breastfeeding mothers’ knowledge and problem-solving skills, especially in urban areas where barriers to exclusive breastfeeding are more complex [35].
Children are at risk for vitamin A deficiency, along with subpopulations at risk for deficiencies in folate, thiamine, vitamin B12, niacin, riboflavin, other B vitamins, and vitamin D [36]. To combat micronutrient deficiencies, it is essential to identify those at risk and prevent and manage these risks. In addition to improved and varied diets, fortification, and other public health support measures, the public health approach includes dietary supplementation.
High parental health literacy is associated with positive health behaviors in children, such as increased consumption of fruits and vegetables, decreased consumption of sugary beverages, regular dental brushing, and increased physical activity [23]. Parents, as the most influential factors on their child’s adult health, viewed diet and physical activity in adulthood, and physical activity in infancy and adolescence as important.
The factor that did not contribute to childcare was parents’ sex. However, parental gender considerably moderated the positive parenting influence (maternal vs. paternal) [37]. Nurses and healthcare professionals play a vital role in forming partnerships with parents, addressing patient education, and assisting parents in the growth and development of children. Through the dissemination of educational materials for parents of children, the degree of knowledge could be increased to accurately identify children’s health symptoms, make healthy dietary and health behavior choices, and manage sick children. It is essential to continue to provide those involved (parents and children) with support, knowledge, and skills. There is a need for culturally and contextually pertinent educational interventions, such as traditional (herbal and religious) knowledge and evidence-based knowledge. Households must be thoroughly equipped with awareness, knowledge, and abilities. Future research must continue to elucidate the educational requirements and supportive elements for children and their parents, who are primarily responsible for their growth and development care in the home. This can guide research and clinical efforts to identify effective interventions for parents and children.
Study limitation
This study did not evaluate the impact of a program but only captured the results (output) achieved in 2019. The availability of data obtained only from primary data collection makes secondary research limited. Some of the limitations is that not all the information related to the variables studied is available and secondary data users cannot intervene in the primary data collection process. Researchers can only analyze the data obtained based on secondary data, and the data analyzed were obtained in accordance with the research objectives. Therefore, some information, such as aspects of housing and economic status, including family income and expenditure, are not discussed in their entirety. These factors may be weaknesses of this study. However, the comprehensive and relevant nature of the SKAP survey instrument did not affect the quality of the secondary research conducted.
The results of this study suggest that the government should focus on improving education and family productivity, including family financial and social aspects, as well as massive health promotion for parents to be prepared to provide optimal childcare in the future. Therefore, these results can be used to evaluate the implementation of the National Population and Family Planning Board. In addition, it can be an input for policymakers in formulating Family Planning and Development Program policies and preparing future program implementation strategies.
Conclusions
Child health problems occur at several levels, such as individual, family household, and community levels. As a result, the variables of parents’ education, occupation, health insurance ownership, number of toddlers, and health media exposure contribute to the quality of childcare. Meanwhile, the variables of parental gender and parents occupation did not significantly contribute to the quality of childcare. The results of the multivariate analysis showed that variables in this research had a significant effect on childcare at a significance level of 10% (α = 0.10), except parents education. Older parental age (20–34), exposure to health media (11–15 types of media), having more than two toddlers and pre-school age, and without health insurance showed better childcare. These results can be used as evaluation and input for implementing family planning and development programs in the future. Based on this study, it is recommended that the government and public health officers specifically provide more health promotion of childcare to populations with the same conditions as the related factors. It is hoped that future research will specifically look at children’s factors regarding their psychological and physical growth and development, so that they do not only focus on parental factors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Joronen K, Rantanen A. Family Life Cycle Stages. Encyclopedia of Quality of Life and Well-Being Research [Internet]. 2014 [cited 2024 Sep 25];2186–8. Available from: https://link.springer.com/referenceworkentry/10.1007/978-94-007-0753-5_1004
- 2Lanjekar PD, Joshi SH, Lanjekar PD, Wagh V. The Effect of Parenting and the Parent-Child Relationship on a Child’s Cognitive Development: A Literature Review. Cureus [Internet]. 2022 Oct 22 [cited 2024 Aug 9];14(10). Available from: /pmc/articles/PMC 9678477/10.7759/cureus.30574 PMC 967847736420245 · doi ↗ · pubmed ↗
- 3Türk O, Dergisi SB, Özkan E, Pekçetin S, Temel RG. The Parental Occupational Balance and Child-Parent Relationship. Online Turkish Journal of Health Sciences [Internet]. 2023 Sep 6 [cited 2024 Aug 9];8(3):326–31. Available from: https://dergipark.org.tr/en/pub/otjhs/issue/79625/1238445
- 4Kemkes. Kementerian Kesehatan Rilis Hasil Survei Status Gizi Indonesia (SSGI) tahun 2022 [Internet]. Kemkes RI. 2023. Available from: https://upk.kemkes.go.id/new/kementerian-kesehatan-rilis-hasil-survei-status-gizi-indonesia-ssgi-tahun-2022
- 5Kang Y, Aguayo VM, Campbell RK, Dzed L, Joshi V, Waid JL et al. Nutritional status and risk factors for stunting in preschool children in Bhutan. Matern Child Nutr. 2018;14(4).10.1111/mcn.12653 PMC 658744430412341 · doi ↗ · pubmed ↗
- 6Mäkelä I, Koivuniemi E, Vahlberg T, Raats MM, Laitinen K. Self-reported parental healthy Dietary Behavior relates to views on child feeding and health and Diet Quality. Nutrients. 2023;15(4).10.3390/nu 15041024 PMC 995900836839382 · doi ↗ · pubmed ↗
- 7Makoae M, Mokhele T, Naidoo I, Sifunda S, Sewpaul R. Determinants of parents taking their children for scheduled vaccinations during COVID-19 pandemic in South Africa. Vaccines (Basel). 2023;11(2).10.3390/vaccines 11020389 PMC 996381536851266 · doi ↗ · pubmed ↗
- 8Paramashanti BA, Dibley MJ, Huda TM, Alam A. Breastfeeding perceptions and exclusive breastfeeding practices: A qualitative comparative study in rural and urban Central Java, Indonesia. Appetite. 2022 Mar 1;170. 10.1016/j.appet.2021.10590734979175 · doi ↗ · pubmed ↗