CT‐Imaging Manifestations and Diagnostic Insights in Pulmonary Intravascular Large B‐Cell Lymphoma: A Case Series and Literature Review
Xinyi Gou, Yinli Zhang, Yuan Li, Libao Hu, Jin Cheng, Nan Hong

TL;DR
This study examines chest CT and PET/CT imaging features of a rare lung lymphoma, revealing common patterns and diagnostic insights.
Contribution
The study provides new clinical imaging insights for diagnosing pulmonary intravascular large B-cell lymphoma through a case series and literature review.
Findings
Chest CT scans of IVLBCL patients commonly show bilateral ground-glass opacities.
FDG PET/CT demonstrates high sensitivity for detecting pulmonary IVLBCL lesions.
FDG PET/CT can detect metabolic activity in lesions even when CT scans appear normal.
Abstract
Intravascular large B‐cell lymphoma (IVLBCL) is a rare and aggressive subtype of non‐Hodgkin lymphoma. Although autopsy findings have revealed that IVLBCL often involves the lungs, its clinical features and imaging manifestations have rarely been reported. This study aimed to explore the pulmonary imaging manifestations of three patients with pulmonary IVLBCL. We retrospectively reviewed the clinical data and chest computed tomography (CT) images of three patients diagnosed with pulmonary IVLBCL between January 2010 and July 2023 in our hospital. In this case series, three patients (2 males and 1 female, aged 51–65 years) presented with a variety of symptoms. Laboratory tests revealed elevated lactate dehydrogenase levels in all three individuals. Chest CT scans revealed bilateral ground‐glass opacities (GGOs) in the lungs in all cases. Although previous case reports have often…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
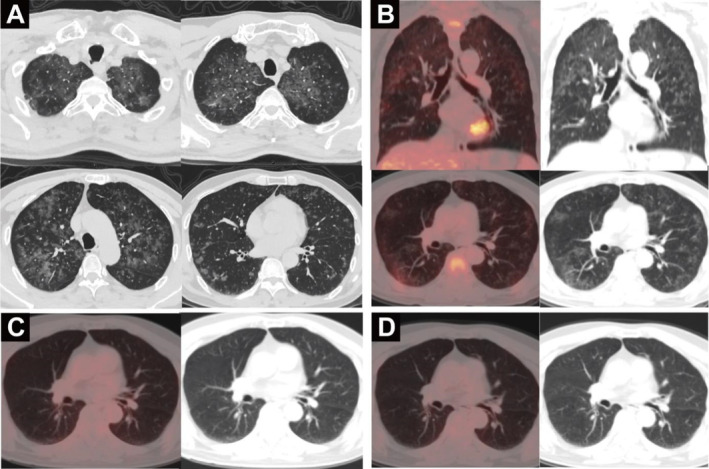 FIGURE 1
FIGURE 1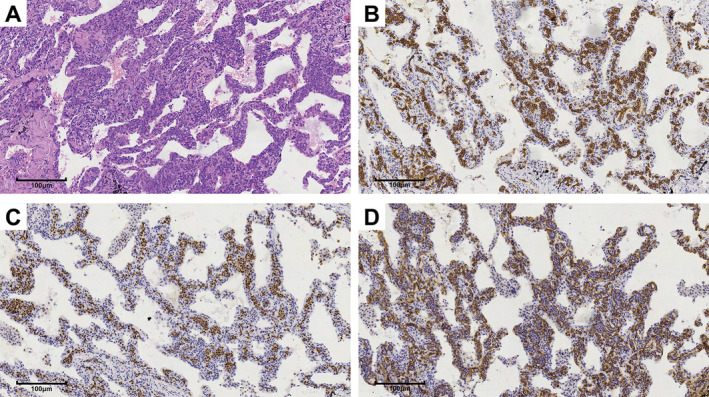 FIGURE 2
FIGURE 2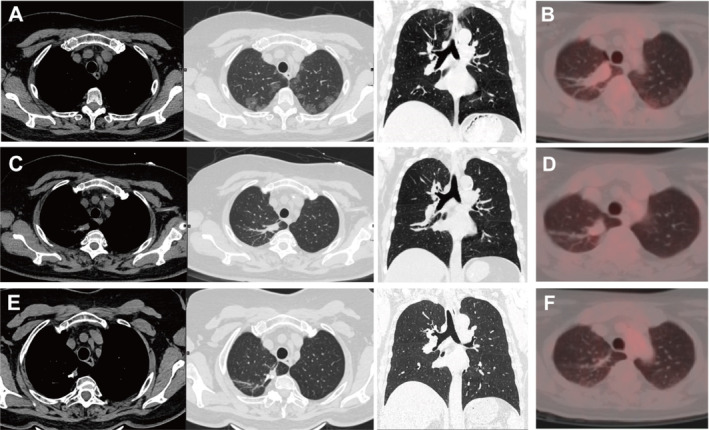 FIGURE 3
FIGURE 3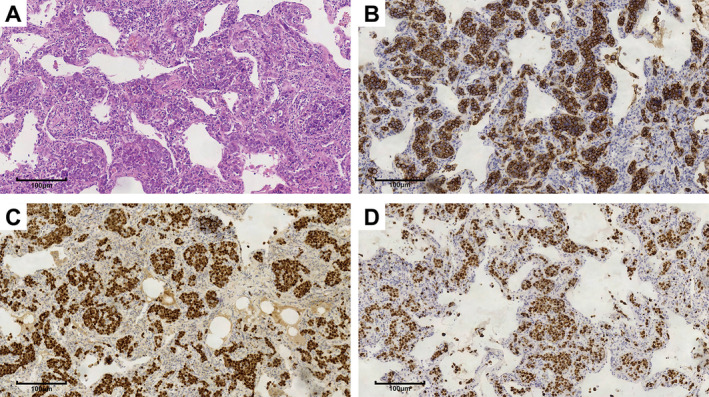 FIGURE 4
FIGURE 4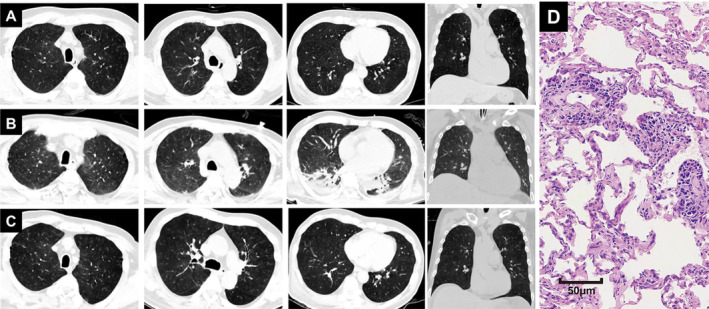 FIGURE 5
FIGURE 5| Case 1 | Case 2 | Case 3 | |
|---|---|---|---|
| Age | 65 | 63 | 51 |
| Sex | Male | Female | Male |
| Involving site | |||
| Pulmonary | + | + | + |
| Brain | − | − | + |
| Other | − | − | + |
| Clinical features | |||
| Fever | − | − | + |
| General fatigue | + | − | + |
| Laboratory examination | |||
| LDH (U/L) | \ | 338 | 1250 |
| RBC (1012/L) | 4.22 | 3.99 | 4.6 |
| WBC (109/L) | 4.5 | 5.7 | 6.7 |
| Plt (109/L) | 155 | 254 | 76 |
| Hemoglobin (g/L) | 128 | 123 | 157 |
| Ki‐67 (%) | 90 | 90 | 10 |
| Ground‐glass opacities | + | + | + |
| With consolidation | + | − | − |
| Ill‐Defined GGOs | − | − | + |
| Associated findings | |||
| Pleural effusion | − | − | + |
| Pericardial effusion | − | − | − |
| Interlobular septal thickening | − | − | − |
| Distribution | |||
| Axial plane | Random | Peripheral | Random |
| Coronal plane | Middle and upper lung field predominant | Upper lung field predominant | Diffuse |
| References | Case | Age | Sex | Clinical findings | Laboratory findings | CT findings | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Fever | Cough | Dyspnea | LDH | CRP | sIL2‐R | |||||
| [ | No. 1 | 35 | F | 37°C–39°C | Yes | Yes | 1554 IU/L | 175 U/L | NA | Bilateral interstitial shadows with small granules and nodules |
| [ | No. 1 | 54 | F | 37.6°C | Yes | Yes | 749 IU/L | NA | NA | Bilateral diffuse, hazy ground‐glass infiltrates throughout the lungs |
| [ | No. 1 | 69 | F | 37.3°C–39.8°C | Yes | Yes | 2250 IU/L | 88 mg/L | NA | Increased attenuation in bilateral lung parenchyma with multiple GGOs and part progression to consolidation, especially on the superior lobes |
| [ | No. 2 | 68 | M | Low‐grade fever | Yes | Yes | 1449 IU/L | 12 mg/L | NA | A ground pattern in a mosaic distribution and small centrilobular nodules |
| [ | No. 4 | 60 | F | Intermittent high fevers to 39°C | NA | Yes | 1542 IU/L | 80 mg/L | NA | Pulmonary nodules with part‐solid diffused GGOs in the lungs without pleural involvement |
| [ | No. 1 | 70 | F | Intermittent high fevers to 39°C | Yes | Yes | 1977 U/L | NA | NA | Patchy GGO throughout both lungs with lower‐lobe predominance |
| [ | No. 1 | 56 | M | Yes | NA | Yes | 1416 U/L | NA | 1744 U/mL | Bilateral diffuse faint GGOs |
| [ | No. 1 | 73 | M | Yes | Yes | Yes | 562 U/L | 17.9 mg/dL | 8313 U/mL | Diffusely spreading GGOs in both lungs |
| [ | No. 1 | 76 | F | NA | NA | Yes | NA | NA | NA | Diffuse interstitial thickening and GGOs with a basilar predominance within the lungs |
| [ | No. 1 | 44 | M | Yes | Yes | Yes | 1000 U/L | NA | NA | Diffuse hazy ground glass infiltrates throughout both lung fields |
| [ | No. 1 | 75 | M | NA | NA | NA | 1491 | 39.8 | NA | Bilateral GGOs predominantly in the upper lobes with increased nodularity |
| [ | No. 1 | 59 | M | No | Yes | No | 712 U/L | NA | NA | Bilateral patchy GGOs and reversed halo sign |
| [ | No. 1 | 74 | M | NA | NA | Yes | 238 U/L | 0.6 mg/dL | 1277 U/mL | Multiple bilateral pulmonary GGNs |
| [ | No. 1 | 39 | F | No | Yes | Yes | 1532 U/L | 35.39 mg/L | NA | Increased attenuation in bilateral lung parenchyma with multiple GGOs |
| [ | No. 1 | 61 | M | Yes | Yes | No | 971 U/L | 40.76 mg/L | NA | Bilateral multiple GGOs with diffuse interlobular septal thickening |
| [ | No. 2 | 69 | F | Yes | Yes | Yes | NA | NA | NA | Bilateral diffuse GGO |
| [ | No. 1 | 70 | F | Subfever | NA | Yes | 947 U/L | 3.28 mg/dL | 5280 U/mL | A diffuse, minimal, nonspecific ground‐glass appearance in both lungs |
| [ | No. 1 | 73 | M | Intermittent fever | Yes | Yes | 480 IU/L | NA | NA | Diffuse ground‐glass opacities, bilateral hilar calcified lymph nodes |
| [ | No. 1 | 73 | M | NA | NA | Yes | NA | NA | 2098 U/mL | Multiple patchy GGO in the bilateral lungs and a solid lesion in the right lower lobe of the lung (approximately 2 cm) |
| [ | No. 1 | 66 | M | Yes | Yes | Yes | 2726.3 U/L | 56.6 mg/L | NA | GGOs in bilateral lung fields and mild pericardial effusion |
| [ | No. 1 | 65 | F | Intermittent fever | NA | 281.25 U/L | 44.93 mg/L | 236 U/mL | Scattered subpleural GGO in both lungs | |
| [ | No. 1 | 68 | M | Intermittent high fevers | Yes | Yes | 2340 IU/L | 13.4 mg/L | NA | Thickened interlobular septa, multiple micronodules and ground‐glass opacity patched in bilateral lungs |
| No. 2 | 60 | F | Intermittent high fevers | NA | Yes | 1434 IU/L | 79.9 mg/L | NA | Diffuse centrilobular nodules and ground‐glass opacity in the bilateral lungs, with local thinckened interlobular septa | |
| No. 3 | 69 | F | Yes | Yes | Yes | 1095 IU/L | 88.5 mg/L | NA | Multiple patches, and GGO in bilateral lungs, with local interlobular septal thickening | |
| References | Case | Age | Sex | Clinical feature | Laboratory findings | FDG PET/CT findings | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Fever | Cough | Dyspnea | LDH | CRP | sIL2‐R | |||||
| [ | No. 1 | 58 | Female | 40°C | Yes | Yes | 570 IU/L | 10.3 mg/dL | 3699 U/mL | NA |
| [ | No. 1 | 43 | Male | Yes | Yes | Yes | Increased | NA | NA | Diffuse and dense FDG uptake of the lungs (SUVmax: 5.44) |
| [ | No. 1 | 60 | Male | 39.8°C | NA | Yes | Increased | Increased | NA | Diffuse hypermetabolic bilateral pulmonary FDG uptake, greater than physiologic hepatic uptake |
| [ | No. 1 | 41 | Male | Yes | Yes | NA | Increased | NA | NA | Diffuse FDG uptake in and the bilateral lungs before treatment; PET showed disappearance of FDG uptake in the bilateral lungs after treatment |
| [ | No. 1 | 58 | Female | Yes | NA | NA | NA | NA | 6774 pg/mL | A subsequent examination using FDG PET/CT showed a high uptake in the bilateral lung |
| [ | No. 3 | 65 | Male | No | Yes | Yes | 886 IU/L | 27 mg/L | NA | NA |
| [ | No. 1 | 84 | Male | NA | NA | NA | 641 IU/L | NA | 2238 U/mL | There was no abnormal accumulation of FDG in bilateral lung fields |
| [ | No. 1 | 63 | Male | Yes | NA | NA | 520 U/L | NA | NA | Mild FDG activity in both lungs (SUVmax = 2.2) |
- —Peking University People’s Hospital Scientific Research and Development Funds
- —Natural Science Foundation of Beijing Municipality 10.13039/501100005089
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCNS Lymphoma Diagnosis and Treatment · Lymphoma Diagnosis and Treatment · Moyamoya disease diagnosis and treatment
Background
1
Intravascular large B‐cell lymphoma (IVLBCL) is a rare subtype of non‐Hodgkin lymphoma, characterized by the filling of lymphoma cells in the vascular lumen [1]. IVLBCL occurs infrequently, with an estimated prevalence of about 0.095 per million people in the United States and roughly 0.5 cases per million worldwide [2, 3].
It has a heterogeneous presentation with no lymphadenopathy or detectable lymphoma cells in the peripheral blood. IVLBCL has a slight male predominance of 1.1:1 and predominantly affects the elderly, with a median age at diagnosis of 67 years (range, 41–85 years) [4]. It is highly invasive and can involve various organs throughout the body, and pulmonary involvement is frequently observed in autopsy studies [5, 6]. Its prognosis is extremely poor, with a median survival time of approximately 1 year [7].
Early diagnosis is crucial for IVLBCL patients, as previous studies have shown that patients who receive timely and appropriate treatment have a better prognosis [8]. Due to its rare occurrence and ambiguous clinical presentation (such as fever of unknown origin and dyspnea), IVLBCL is frequently misdiagnosed or only identified during post mortem examination [9, 10, 11]. Laboratory findings in patients with IVLBCL with lung involvement typically include anemia, a low platelet count, and high serum lactate dehydrogenase (LDH) levels [12, 13]. Confirming the diagnosis requires histological examination, typically through a random skin biopsy or bone marrow biopsy and transbronchial lung biopsy (TBLB) [10, 14, 15, 16, 17]. While the path from non‐specific symptoms to histopathological confirmation can be challenging, medical imaging techniques serve a vital role in providing supplementary diagnostic information.
Most patients with pulmonary IVLBCL undergo chest computed tomography (CT) scans because of fever and respiratory symptoms. This may provide an opportunity to suspect IVLBCL. Fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT), which has demonstrated a high sensitivity in detecting non‐Hodgkin's lymphoma, was prominent [18, 19]. Therefore, further understanding of the imaging findings of IVLBCL with pulmonary involvement is crucial for early diagnosis and prognosis improvement [12].
Although previous studies have reported that ground‐glass opacities (GGO) and diffuse FDG uptake can be seen on imaging of lung involvement, the radiological features are still not well described. The present study aimed to provide a detailed descriptive evaluation of radiological findings associated with pulmonary IVLBCL. Through an analysis of three case studies and a review of published reports, we sought to characterize the imaging patterns that can aid in recognizing this rare disease, thereby enhancing the diagnostic accuracy and guiding clinical management.
Case Presentation
2
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Helsinki Declaration (as revised in 2013), and the study was approved by the Ethics Review Committee of our hospital. We retrospectively reviewed the clinical data and chest images of three patients diagnosed with pulmonary IVLBCL at Peking University People's Hospital between January 2010 and July 2023. The inclusion criteria were as follows: (1) diagnosis of IVLBCL based on pulmonary pathology samples, and (2) availability of corresponding chest CT images. The clinical information and chest CT imaging manifestations of these patients are summarized in Table 1.
Case 1
2.1
A 65‐year‐old male was admitted to our hospital in April 2019 because of a month history of paroxysmal dry cough, dyspnea, and fatigue. Diffuse patchy and nodular GGOs were found in both lungs, mostly in the middle and upper lung fields, with clear subpleural areas (Figure 1A). An FDG PET/CT scan (April 23, 2019) showed that these lesions were accompanied by increased FDG uptake with an SUVmax of 1.9 (Figure 1B). After thoracoscopic lung wedge resection, multiple nodular lesions were observed in the lung tissue of the right middle lobe specimen; the alveolar septa were widened in the lesion area, the capillaries were dilated, and medium to large lymphoid cells were observed in the lumen, with fine chromatin and small nucleoli (Figure 2). Immunohistochemical staining showed CD20(+), CD34(−), CD3(−), CD43(−), PAX‐5(+), CD30(−), bcl‐6(−), mum‐1(+), CD10(−), and a Ki‐67 proliferation index of > 90%. Therefore, the diagnosis of pulmonary IVLBCL was confirmed.
(A) Chest CT images before chemotherapy showing bilateral diffuse patchy and nodular GGOs of the lungs; (B) FDG PET/CT images before chemotherapy showing increased FDG uptake; FDG PET/CT after four (C) and eight (D) rounds of chemotherapy showing that previous lesions disappeared and no FDG uptake was observed.
Lung wedge resection specimen (right middle lobe), (A) hematoxylin and eosin staining, ×20 magnification; (B) immunohistochemical staining for CD20, ×20 magnification; (C) PAX5 staining, ×20 magnification; (D) immunohistochemical staining for CD34, ×20 magnification.
The patient underwent four cycles of R‐CHOP chemotherapy (rituximab, cyclophosphamide, epirubicin, vinesine, and dexamethasone). FDG PET/CT re‐examination (August 19, 2019) showed that the bilateral diffuse GGOs had disappeared and no obvious FDG uptake was observed, indicating a complete metabolic response (Figure 1C). After four additional cycles of R‐CHOP chemotherapy and rituximab monotherapy consolidation treatment, a follow‐up FDG PET/CT revealed continued complete metabolic response on January 2, 2020 (Figure 1D). No recurrence was observed during the approximately three‐year follow‐up period ending on January 20, 2022.
Case 2
2.2
A 64‐year‐old woman with multiple ground‐glass nodules (GGNs) detected during a medical checkup was referred to our hospital on August 12, 2020. She had no respiratory symptoms, and after a 12‐day course of antibiotics, no significant changes were observed in her lung condition. During outpatient follow‐up on October 28, 2020, chest CT images revealed multiple well‐defined round GGNs (the largest one was approximately 6 mm) beneath the pleura in the bilateral upper lobes of the lung (Figure 3A). TBLB and bronchoalveolar lavage fluid (BALF) analysis were performed (November 2, 2020), but no significant abnormalities were found. The patient underwent FDG PET/CT (November 10, 2020) after TBLB, which revealed multiple GGNs and increased FDG uptake in some areas (SUVmax: 1.7) (Figure 3B). After wedge resection by thoracoscopy on November 11, 2020, pathological examination showed that the lung tissue had interstitial vascular dilation and was filled with lymphoid cells of moderate size with nuclear atypia, visible nucleoli, and mitotic figures (Figure 4). Immunohistochemically, these atypical cells were positive for CD20, CD5, PAX‐5, BCL2, BCL6, and MUM1; negative for CD3, CD5, and CD10; and had a Ki‐67 proliferation index of > 90%. The patient was diagnosed with pulmonary IVLBCL.
(A) Chest CT images before chemotherapy showing multiple GGOs beneath the pleura in the bilateral upper lobes of the lungs; (B) FDG PET/CT images before chemotherapy; (C, D) chest CT images and FDG PET/CT images after the first round of chemotherapy showing disappearance of lesions and no FDG uptake; (E, F) chest CT images and FDG PET/CT images after the second round of chemotherapy showing disappearance of the lesions and no FDG uptake.
Lung wedge resection specimen (right upper lobe), (A) hematoxylin and eosin staining, ×20 magnification; (B) Immunohistochemical staining for CD20, ×20 magnification; (C) PAX5 staining, ×20 magnification; (D) Ki‐67 staining, ×20 magnification.
After one round of chemotherapy with the R‐CHOP regimen, chest CT images (January 15, 2021) revealed that the GGNs had disappeared (Figure 3C,E), and there was no metabolic activity on FDG PET/CT (February 9, 2021) (Figure 3D,F). Subsequently, complete metabolic response was considered. The patient received R‐CHOP regimen chemotherapy and rituximab monotherapy in the following 1 month. Continuous follow‐up monitoring was then conducted. The latest chest CT scan on February 5, 2025, did not reveal any significant abnormalities, and no recurrence has been observed.
Case 3
2.3
A 51‐year‐old man presented with dyspnea for 2 months on May 19, 2022. Laboratory results showed elevated LDH, decreased platelet count, and decreased albumin levels. And C‐reactive protein was 18.5 mg/L. Chest CT images (May 20, 2022) showed bilateral diffuse ground‐glass infiltration with unclear boundary (Figure 5A). Empiric treatment with anti‐infection and symptomatic treatments was ineffective. Chest CT images (May 30, 2022) showed diffuse and hazy ground‐glass infiltrates in both lungs and pleural effusion (Figure 5B). Hormone and immunoglobulin therapies were administered, and the symptoms improved. Moreover, chest CT (June 17, 2022) showed diffuse GGOs in both lungs, which had improved compared with before, and a small amount of pleural effusion on both sides was absorbed compared with before (Figure 5C). The lung biopsy sample from the outer basal segment of the right lower lobe showed that the alveolar septum was widened and the inner vascular wall was filled with moderately large lymphoid cells, revealing intravascular large B‐cell lymphoma in the lungs. Pulmonary IVLBCL was confirmed. Unfortunately, the patient was discharged from the hospital against medical advice, and death was confirmed 3 months later via telephone follow‐up.
(A) Baseline chest CT images revealed bilateral diffuse ground‐glass infiltrates; (B) following empirical treatment, chest CT images demonstrated persistent diffuse and hazy ground‐glass opacities in both lungs, accompanied by pleural effusion; (C) after immunoglobulin and hormone therapy, chest CT images showed diffuse GGOs in both lungs, which had improved, and a small amount of pleural effusion on both sides had been absorbed. (D) Hematoxylin and Eosin staining of the lung biopsy specimens (×20 magnification).
Discussion
3
IVLBCL is characterized by the preferential growth of malignant lymphocytes within the lumina of small vessels. In cases with isolated pulmonary involvement, tumor cells infiltrate the pulmonary vasculature, resulting in local ischemia and inflammation. This can manifest as symptoms such as dyspnea and cough, accompanied by specific radiological abnormalities. It typically has a poor prognosis and is often fatal. Although early and standardized chemotherapy can greatly improve the prognosis of patients with IVLBCL, early diagnosis remains a major challenge due to the nonspecific clinical presentation and low incidence of this disease. This study reported three cases of pulmonary IVLBCL (Table 1) and reviewed chest CT images and clinical information of 32 patients with pulmonary IVLBCL in previous case reports (Tables 2 and 3).
Clinical Features and Laboratory Findings
3.1
IVLBCL can manifest with fever, fatigue, weight loss, and other symptoms. Lung involvement may cause cough, dyspnea, and hypoxemia. However, clinical manifestations may be absent in some cases, such as in Case 2 and a previous case [45]. Laboratory findings frequently revealed elevated LDH and soluble interleukin‐2 receptor (sIL‐2R) levels, thrombocytopenia, and other abnormalities (Table 2). Moreover, a previous study found that sIL2R levels were significantly higher in patients with Asian‐variant IVLBCL than in those with non‐Asian‐variant IVLBCL [47].
Diagnostic Clues in Medical Imaging
3.2
GGO is typically defined as an area exhibiting hazy obscuration or increased attenuation in chest imaging. It results from the replacement of air by various factors, including fluid, collapsed airways, fibrotic tissue, or neoplastic growth. According to previous case reports and our case series of IVLBCL with pulmonary involvement, bilateral GGOs were the most common chest CT manifestations in these patients [29, 48]. A total of 35 patients (20 males and 15 females, aged 35–84 years) with pulmonary IVLBCL were reviewed based on previous case reports and three cases from our hospital. Among them, 21 cases (including Case 3) showed multiple or diffuse GGO infiltrations in both lungs (60.0%), 6 cases (including Cases 1 and 2) showed multiple GGOs with clear borders (17.1%), and no obvious abnormal chest CT findings were observed in eight cases (22.9%). This finding may be related to the pathological presentation of IVLBCL in the lungs, which typically involves widening of the interstitial space between the alveoli, expansion of capillaries and lymphoid tissue, and filling of the lumen of the bronchioles with lymphoid cells.
Although bilateral GGOs are frequently observed in IVLBCL patients, these findings lack specificity. FDG PET/CT scans can reveal high diffuse uptake of FDG in lesions of IVLBCL patients earlier, providing crucial diagnostic information such as lesion location and extent of IVLBCL involvement [49, 50]. It is important to note that other conditions, including acute respiratory distress syndrome, pulmonary contusion, and inflammatory or infectious pneumonitis, may also manifest as GGOs on CT scans, particularly in areas with increased FDG uptake. These conditions can be differentiated based on the patient's medical history and disease course [42]. Therefore, FDG PET/CT plays an important role in the diagnosis of IVLBCL.
In addition, some case reports demonstrated that some pulmonary IVLBCL patients could have no abnormality on chest CT, although some of them had fever and dyspnea (Table 3). However, diffuse FDG uptake is usually observed in the lungs. Diffuse FDG uptake without evident chest CT findings is called hot lung, which is quasi‐pathognomonic for pulmonary IVLBCL [41]. When pulmonary IVLBCL is highly suspected clinically but chest CT is normal, FDG PET/CT can provide valuable information. Additionally, hot lung may also indicate chemotherapy‐induced pneumonia or acute respiratory distress syndrome, which requires differentiation based on the patient's history [41, 42].
As a noninvasive imaging technique, FDG PET/CT has significant value in IVLBCL patients [47, 51]. FDG PET/CT also plays an important role in guiding biopsy sites and evaluating the extent of systemic involvement or response to chemotherapy after relapse [51]. Therefore, even if there are no obvious abnormalities in chest CT scans, FDG PET/CT can be considered to obtain more comprehensive diagnostic information non‐invasively for patients with fever of unknown origin, fatigue, elevated LDH levels, ineffective conventional anti‐inflammatory treatment, or those who are highly suspected of pulmonary IVLBCL.
In addition, it is crucial to recognize that diagnostic tests like FDG PET/CT and TBLB cannot detect all lesions with 100% accuracy. Therefore, the doctor's assessment and judgment play a vital role in the diagnostic process. One patient was diagnosed with pulmonary IVLBCL by TBLB without obvious abnormal chest CT and FDG PET/CT findings in a previous literature report [45]; there was focal FDG high uptake and no abnormal TBLB findings in Case 2.
Conclusions
4
IVLBCL should be considered in patients with symptoms such as fever of unknown origin, fatigue, elevated LDH levels, or hemophagocytic syndrome. In the diagnosis and monitoring of pulmonary IVLBCL, chest CT scans are indispensable. Bilateral GGOs are frequently observed and may show improvement following therapeutic intervention. Furthermore, GGOs may sometimes manifest as multiple, distinct GGNs with clear boundaries. Although chest CT scans may occasionally appear unremarkable, elevated FDG uptake in PET/CT imaging can suggest lung involvement. When FDG PET/CT yields positive results, prompt biopsy should be considered. Accurate diagnosis depends on the combination of H&E staining for morphological examination and IHC to verify B‐cell lineage and distinguish IVLBCL from other lymphoma types, thereby informing appropriate treatment approaches.
Author Contributions
Conceptualization: Xinyi Gou, Libao Hu, and Jin Cheng. Methodology: Yuan Li and Jin Cheng. Software: Xinyi Gou. Data curation: Yinli Zhang and Yuan Li. Investigation: Xinyi Gou, Yinli Zhang, and Yuan Li. Validation: Xinyi Gou and Yinli Zhang. Formal analysis: Xinyi Gou. Supervision: Libao Hu and Jin Cheng. Funding acquisition: Libao Hu. Visualization: Xinyi Gou. Project administration: Jin Cheng and Nan Hong. Resources: Jin Cheng and Nan Hong. Writing – original draft: Xinyi Gou. Writing – review and editing: Xinyi Gou, Yinli Zhang, Libao Hu, Jin Cheng, and Nan Hong.
Ethics Statement
This retrospective study was approved by the Ethics Review Committee of the Peking University People's Hospital (no. 2022PHB276‐001). The authors are accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013). Written informed consent was obtained from all participants, or if participants were under 16 years of age, from a parent and/or legal guardian.
Consent
All procedures were discussed with the patients, and they gave their full consent in writing to the present publication and accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Ponzoni , E. Campo , and S. Nakamura , “Intravascular Large B‐Cell Lymphoma: A Chameleon With Multiple Faces and Many Masks,” Blood 132, no. 15 (2018): 1561–1567.30111607 10.1182/blood-2017-04-737445 · doi ↗ · pubmed ↗
- 2K. Shimada and H. Kiyoi , “Current Progress and Future Perspectives of Research on Intravascular Large B‐Cell Lymphoma,” Cancer Science 112, no. 10 (2021): 3953–3961.34327781 10.1111/cas.15091 PMC 8486207 · doi ↗ · pubmed ↗
- 3D. J. Rajyaguru , C. Bhaskar , A. J. Borgert , A. Smith , and B. Parsons , “Intravascular Large B‐Cell Lymphoma in the United States (US): A Population‐Based Study Using Surveillance, Epidemiology, and End Results Program and National Cancer Database,” Leukemia & Lymphoma 58, no. 9 (2017): 1–9.10.1080/10428194.2017.128736328278725 · doi ↗ · pubmed ↗
- 4T. Murase , M. Yamaguchi , R. Suzuki , et al., “Intravascular Large B‐Cell Lymphoma (IVLBCL): A Clinicopathologic Study of 96 Cases With Special Reference to the Immunophenotypic Heterogeneity of CD 5,” Blood 109, no. 2 (2007): 478–485.16985183 10.1182/blood-2006-01-021253 · doi ↗ · pubmed ↗
- 5X. Bai , X. Li , L. Wan , G. Wang , N. Jia , and J. Geng , “Intravascular Large B‐Cell Lymphoma of the Kidney: A Case Report,” Diagnostic Pathology 23, no. 6 (2011): 86.10.1186/1746-1596-6-86PMC 318910521943175 · doi ↗ · pubmed ↗
- 6T. Takeshige , N. Harada , Y. Sekimoto , et al., “Pulmonary Intravascular Large B‐Cell Lymphoma (IVLBCL) Disguised as an Asthma Exacerbation in a Patient With Asthma,” Internal Medicine 56, no. 14 (2017): 1885–1891.28717087 10.2169/internalmedicine.56.7613 PMC 5548684 · doi ↗ · pubmed ↗
- 7Z. Liu , Y. Zhang , Y. Zhu , and W. Zhang , “Prognosis of Intravascular Large B Cell Lymphoma (IVLBCL): Analysis of 182 Patients From Global Case Series,” CMAR 12 (2020): 10531–10540.10.2147/CMAR.S 267825 PMC 759106733122951 · doi ↗ · pubmed ↗
- 8K. Sakaguchi and T. Watari , “Early Diagnosis of Intravascular Large B‐Cell Lymphoma by Random Skin Biopsy,” Eur J Case Rep Intern Med 9, no. 7 (2022): 003497.36051170 10.12890/2022_003497 PMC 9426967 · doi ↗ · pubmed ↗