Advancing pre-clinical surgical education by using intuitive short videos
Marie Perrin, Markus Schäfer, Pierre-Alexandre Bart, Dieter Hahnloser

TL;DR
Short educational videos significantly improve medical students' understanding and retention of abdominal surgery topics, showing high demand and effectiveness in pre-clinical education.
Contribution
Demonstrates the effectiveness of short educational videos in enhancing pre-clinical surgical education and student engagement.
Findings
90-96% of students found videos helpful for understanding and recalling lecture content.
A median 12.5% improvement in examination results was observed when videos were used.
High demand for videos was consistent across all student cohorts.
Abstract
The ever-expanding field of surgery requires novel tools to teach surgical pathologies and their management. Basic knowledge must already be acquired on a pre-graduate level at medical school. The SARS-CoV-19 pandemic has pushed students to explore digital online platforms to complement their medical education. This study aimed to assess the utility of short educational videos and the importance of digital learning methods to teach abdominal surgery. A literature review was performed for a thorough understanding of educational videos. Short videos were then created covering different topics of abdominal surgery. To evaluate the utility of such videos, three consecutive cohorts of medical students were compared. The first cohort comprised students studying without the videos (V0), whereas the second and third cohorts had access to the videos (V1, V2). Between the three groups, the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
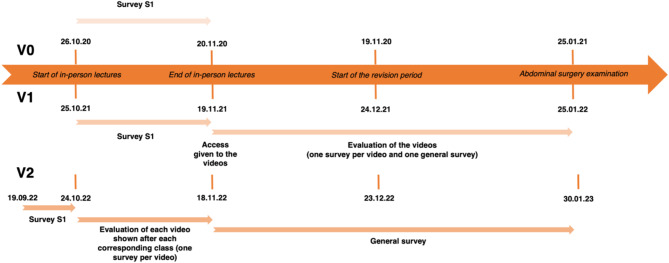 Figure 1
Figure 1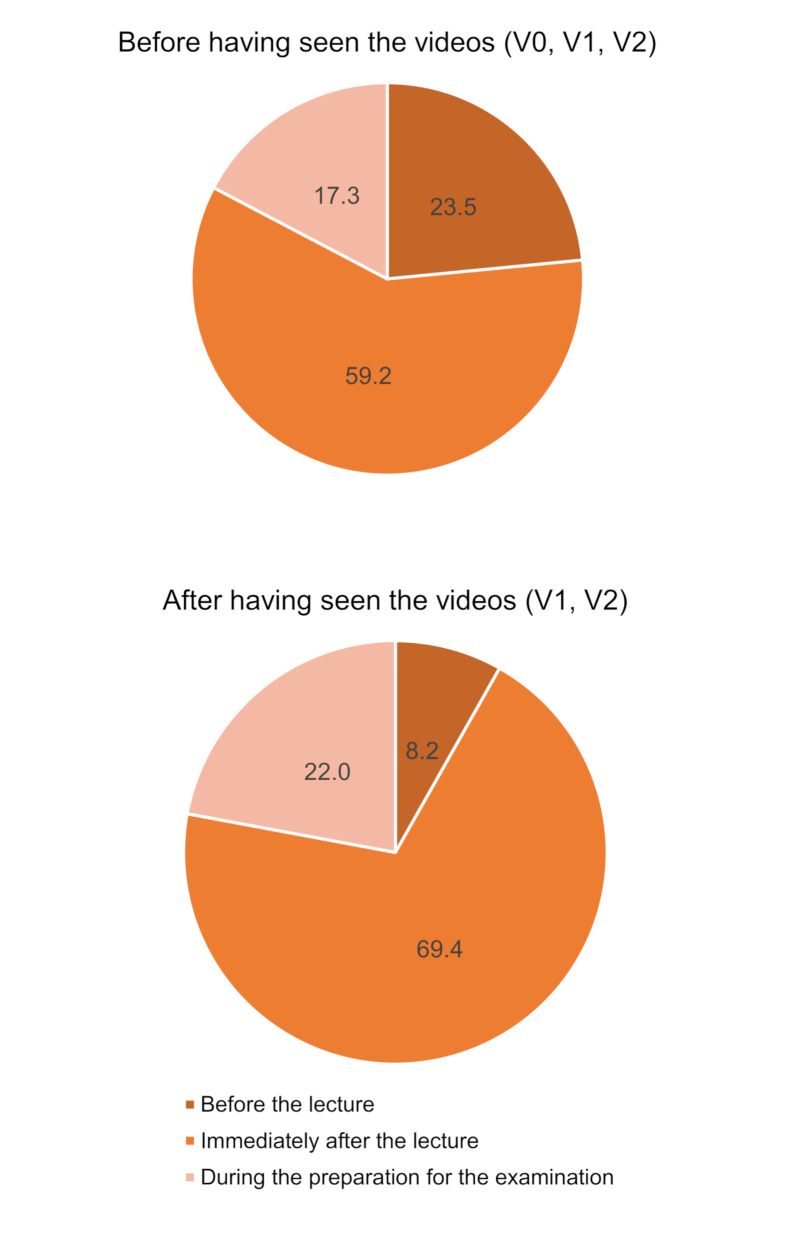 Figure 2
Figure 2 Figure 3
Figure 3- —University of Lausanne
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovations in Medical Education · Surgical Simulation and Training · Simulation-Based Education in Healthcare
Background
Current medical students, belonging to the generations Y (born 1981–1996) and Z (born 1997 or later), can be described as digital natives [1–3]. They use videos daily for various purposes and learn differently than previous generations [4–8]. Different types of online contents, e.g. prerecorded lectures, animated videos, podcasts, and interactive cases, allows students to acquire new information at their own speed, without any constraints of time or location [1, 9–13]. This has been shown to improve learning in numerous studies [1, 9, 14–16]. Hence, medical educators who often belong to digital immigrant generations, have to learn using innovative teaching methods to motivate and attract the attention of younger students [10, 11, 13, 17–19]. It is important to note that actually five generations of physicians are now working and learning together, an unique situation which has never happened before [20].
Videos may transmit information in a very expressive way, resulting in vastly improved learner experiences, knowledge retention, and understanding of the lecture’s content [6, 13, 16]. Furthermore, students consider video materials very engaging [6, 9, 12, 14, 15]. The challenge for medical educators is to use these new technologies effectively to transform learning into a more collaborative and personalized experience [10].
This study aimed to assess the demand and utility of educational videos among third-year medical students at the University of Lausanne. Indeed, courses have typically been delivered in a very traditional manner, with ex-cathedra lectures in large auditoriums. However, there has been a strong initiative to modernize teaching methods to improve learning in visceral/abdominal surgery.
Methods
This prospective study was conducted at the Medical school, University of Lausanne, in association with the Lausanne University Hospital, between October 2020 and January 2023. The study was approved by the dean of the Medical school. Three consecutive third-year medical student classes (V0 = year 2020/2021, V1 = year 2021/2022 and V2 = year 2022/2023) were compared. The third-year’s first semester is composed of three sequential modules, whereby the second module contains abdominal surgery lectures. Following this class-intensive period, four weeks devoid of lectures are dedicated for the preparation of three semestrial examinations, one for each module.
The V0 cohort only received in-person lectures (only available as a live stream due to the SARS-CoV-19 pandemic). The V1 and V2 cohort studied in a blended learning approach using in-person lectures (available face to face as well as a live stream) and the animated educational videos. The V1 group received the videos all at once after having finished all in-person lectures. In comparison, the V2 group received the videos over a 4-week period. Indeed, each video was first shown to the V2 students during the corresponding lecture and was then directly available on the university’s online platform. Figure 1 outlines the timeline for all three cohorts.
Fig. 1. Project timeline
Survey assessing the demand for educational videos (S1)
The same questionnaire was given to all three cohorts prior to having access to the videos. The survey assessed study habits, utility of the educational videos and the students’ preference when the videos should be accessed during the learning process (Appendix 1).
Literature review and creation of the videos
To create appropriate and efficient videos, a vast literature research was done using PubMed with the following search words: “educational videos”, **“**surgical education”, “pedagogical techniques”, “medical students”, “digital learning platform” and cross reference. After analyzing the literature, short, animated videos for all abdominal surgery lectures were created using Microsoft PowerPoint^®^ (version 16.60) and Adobe Illustrator^®^ (version 2021). Respective lecturers were consulted to guarantee the accuracy of the video’s content.
According to the literature, to maximize the benefits of educational videos, three aspects are vital: motivating students to watch the videos, managing the cognitive load of each video and promoting active learning (Table 1) [14].
Table 1. Criteria used to create effective videosCriteriaExamples used in this studyMotivation• Short video lengths• Examination-relevant information• Modern and enjoyable design• Representational illustrations• High-yield video topicsCognitive load management• Videos structured using a similar model• Few rapidly moving visual elements• Highlighting of important information• Uniform introductionActive learning• Open-ended questions in each video with time to answer them
Motivation
The main reason for keeping the videos short, is that student’s engagement is strongly associated with video length [6, 14, 21–23]. Moreover, efforts were made to increase students’ motivation to watch the videos. For example, each video was designed for one respective lecture and contained examination-relevant material [14, 24]. A modern and enjoyable design was also used [14]. It has been shown that the use of visual aids helps students to organize complex contents into meaningful images in their mind, facilitating learning compared to purely text-based methods [25]. Therefore, time was spent on creating representational illustrations in order to serve as the backbone from which students could build their own mental representation of a subject. The chosen topics were frequent and well established in order to minimize the risk yearly modifications [16].
Cognitive load
To make educational videos effective, particular attention was given to managing their cognitive load [6, 14, 26]. For instance, each video followed the same structure and avoided the excessive use of rapidly moving visual elements [21]. Moreover, signals were used to highlight important information [14, 25, 26]. A uniform introduction was created so that students could easily know which video they were viewing [21, 26].
Active learning
In order to promote active learning, each video contained several open-ended questions stimulating self-reflexion [14]. If the time was insufficient to answer these questions, students had the option to pause the video.
Once the videos were available, V1 and V2 students were regularly reminded by email and through the student classes’ WhatsApp^®^ group to watch and evaluate them, as well as during the lectures for the V2 group using a QR-code leading directly to the corresponding survey. All videos were available to students via the university Moodle^®^ platform.
Video evaluation
Three educational parameters were inquired: (A) satisfaction (surveys, see Appendices 2, 3 and 4), (B) examination performance (multiple choice questions results), and (C) students’ engagement in using the videos (indicators extracted from Moodle^®^ statistics). Videos were evaluated individually as well as after the students had viewed all of them. The global pertinence, appreciation, and utility of this new learning format was assessed by the students and the teachers.
Statistical analysis
Descriptive statistics included median and range for continuous variables as well as frequencies and percentages for binary and categorical variables. Categorical data were compared by Chi-2 test and continuous variables by T-test. P-values < 0.05 were considered statistically significant.
Results
Students
In total, 746 students over three years participated in the study (V0 n = 236, V1 n = 255, V2 n = 255). Students’ demographics were comparable in the three groups, with 68% female in V0, 64% in V1 and 63% in V2.
Creation of educational videos
By applying the indications found in the literature research, 23 videos were created according to the in-person lectures given on abdominal surgery (See one of the videos in Appendix 5). Video lengths ranged from 1 min 24 s to 5 min 39 s. The average length was 2 min 35 s, and the total duration of all videos was 59 min 13 s (Table 2).
Table 2. Length, visualizations, and topic of each video (listed by order of appearance on Moodle)Video topicDurationTotal number of viewsNumber of different viewers (percent)Number of views per viewerV1V2**V1V2V1*V2Anal abscess and fistula1 min 25 s353545192 (75.5)204 (80)1.82.7Appendicitis1 min 24 s300632186 (72.9)206 (80.8)1.63.1 Bariatric surgery 1 min 53 s265439172 (67.5)198 (77.7)1.52.2Post-operative complications3 min 17 s253490160 (62.8)201 (78.8)1.62.4Diverticulosis and diverticulitis2 min 59 s260544161 (63.1)201 (78.8)1.62.7Abdominal examination3 min 23 s176262130 (50.9)146 (57.3)1.41.8Hemorrhoids and anal fissures2 min 45 s210418147 (57.7)192 (75.3)1.42.2Inguinal hernia2 min 56 s207413145 (56.9)190 (74.5)1.42.2Hernias2 min 30 s196421140 (54.9)192 (75.3)1.42.2Ileus2 min 50 s235507146 (57.3)199 (78)1.62.6Mesenteric ischemia2 min 10 s211443134 (52.6)193 (75.7)1.62.3Benign lesions of the liver4 min 02 s198452127 (49.4)192 (75.3)1.62.4Crohn’s disease1 min 25 s188401127 (49.4)179 (70.2)1.52.2Acute pancreatitis2 min 25 s209494131 (51.4)191 (74.9)1.62.6Chronic pancreatitis1 min 51 s188419123 (48.2)184 (72.2)1.52.3Biliary tract diseases5 min 39 s215558130 (51)195 (76.5)1.72.9Ulcerative colitis1 min 29 s184350127 (49.4)174 (68.2)1.52.0Lower gastrointestinal bleeding2 min 34 s192383127 (49.4)175 (68.6)1.52.2Splenomegaly and spleen trauma2 min 52 s182453122 (47.8)177 (69.4)1.52.6 Solid organ transplantation 2 min 42 s172201123 (48.2)114 (44.7)1.41.8Abdominal trauma2 min 28 s163342125 (49)170 (66.7)1.32.0Pancreatic tumors2 min 54 s194435127 (49.4)182 (71.4)1.52.4Peptic ulcer and perforation1 min 20 s196445131 (51.4)188 (73.7)1.52.4 Mean 2 min 35 s215,1436,8140,6 (55.1)184,5 (72.4)1,52,4 Median 2 min 34 s198439131 (51.4)191 (74.9)1,52,3Note that the videos in italic were not shown during the class for the V2 group*Numbers collected during a 67-day viewing period, from initial access to examination date** Numbers collected during a 98-day viewing period, from initial access (following each respective class on a 4-week period) to examination date
Students request video-based learning
Response rate to the survey S1 between the three cohorts significantly differed though the absolute differences were small (V0 = 90.3%, V1 = 87.8%, V2 = 78.4%, p < 0.001). In the three cohorts, only 7 to 14% (V0 = 14/213, V1 = 16/224, V2 = 27/203) of students reported studying topics before attending the respective lectures. However, if a short educational video would be available, the majority would have watched it to prepare for the lecture, to review the lecture and to prepare for the examination (Appendix 6). In all cohorts, the overall demand for educational videos was high.
Most students reported using the lecture’s PowerPoint slides (V0 = 94%, V1 = 94%, V2 = 91%) and their personal notes taken during the lecture (V0 = 84%, V1 = 87% and V2 = 75%) to review the lectures and prepare for the examination. Only 20 to 33% used internet videos, including resources such as YouTube^®^, Osmosis^®^ or Khan Academy^®^. In the three cohorts, less frequently used resources included text or table summaries, internet platforms such as Wikipedia^®^ and Amboss^®^, and published scientific books (details can be found in Appendices 7a, b and c).
Prior to introducing the videos to any group, students in all cohorts said they would prefer access to videos immediately after the lecture (60% in V0, 62% in V1 and 56% in V2, p = 0.016) compared to before the lecture or during the examination preparation. This remained the case in V1 and V2 after having viewed the videos (59% and 80%, respectively, p = 0.002, Fig. 2), with V2 responding significantly higher to viewing the videos immediately after the lectures.
Fig. 2. Time points at which the students would prefer to watch the videos. 3a: before having access to the videos (V0, V1, V2); 3b: after having actually watched the videos
Videos are an incredibly effective tool to improve learning
Satisfaction
The videos helped 86% and 95% (V1 and V2, respectively, p = 0.017) of students in their learning of abdominal surgery and 89% and 96% (V1 and V2, respectively, p = 0.026) to remember the lectures more easily. In the V1 and V2 group, 98.9% and 100% (p = 0.835) of students would recommend viewing these videos as part of the abdominal surgery teaching module, respectively.
The response rate to each individual video was low (V1 = 24%, range: 19–40%; V2 = 18%, range: 3–62%, Appendix 8). However, though the following results were not statistically significant, a mean of 94% and 97% (V1 and V2, respectively, p = 0.108) of students found that the videos were successful in summarizing the key points of the lecture. Similarly, a mean of 95% and 98% (V1 and V2, respectively, p = 0.099) of students found that the amount of information presented in the videos was appropriate and that the videos helped to better recall the content presented during the corresponding in-person lecture (V1 = 96% and V2 = 97%, p = 0.085).
The five lecturers were satisfied with the content, the amount of information and the design of the videos corresponding to their classes. Moreover, in 96% of the cases, they found that the corresponding video complemented the lecture well. According to them, the best moment to give the students access to their videos is during or after the lecture (80%), in comparison to during the examination preparation (20%) or before the lecture (0%).
Examination performance
The MCQ examination, presented every year to the students, contained 18 (2021, V0 group), 22 (2022, V1 group) and 19 (2023, V2 group) questions on abdominal surgery topics. Between V0 and V1, 10 questions remained identical, whereas V2 had different questions. Regarding the 10 identical questions, V1 increased the median overall score by 12.5% (p = 0.225, Table 3). Overall, the median percentage of correct answers for all abdominal surgery questions was V0 = 67%, V1 = 87% and V2 = 60%.
Table 3. Examination question subjects and percentages of correct answers in V0 and V1 groupsQuestion number and subjectPercentage of correct answers in V0 (n = 232)Percentage of correct answers in V1 (n = 251)1 – Acute abdomen31.932.32 – Abdominal pain79.769.33 – Anal bleeding70.786.54 – Diverticulitis68.1925 – Acute abdomen84.9986 – Abdominal trauma99.199.67 – Proctology65.953.88 – Abdominal pain77.287.39 – Hepatobiliary surgery91.493.210 – Hepatobiliary surgery71.682.5 Median of correct answers 74.486.9
Students’ engagement in using the videos
Audience retention
Over a 67-day period, the videos accumulating the highest number of views and number of different viewers in the V1 group were “Anal abscess and fistula” (353 views, 192 viewers), followed by “Appendicitis” (300 views, 186 viewers) and “Bariatric surgery” (265 views, 172 viewers). The V2 students accessed each video after the respective lecture, increasing the viewing period up to 98 days. The videos “Appendicitis” (632 views), “Biliary tract diseases” (558 views) and “Anal abscess and fistula” (545 views) accumulated the highest number of views. In both groups, topics focusing on less specific subjects such as “Abdominal trauma”, “Solid organ transplantation” and “Abdominal examination” were among the less consulted videos (Table 2).
Key moments of the audience
In both groups, videos were most often consulted at two key moments during the study period: the start of the examination preparation phase and just before the abdominal surgery examination (Fig. 3). Furthermore, viewing the videos immediately after each corresponding lecture (V2 group) increased the audience (4371 to 7808 Moodle platform consultations per week) and the number of times a video was watched (1.5 to 2.4 times per video). The length of the videos did not impact the number of views.
Fig. 3. Number of Moodle consultations per week while videos were available
Discussion
Educational videos that accompany surgery lectures were considered to be very helpful by third-year medical students, especially if they were immediately available after the lectures. These videos were well-received tools for summarizing lecture content, improving knowledge retention, and supporting preparation for examination. This highlights the potential of integrating video-based learning into traditional teaching methods to meet the student needs.
The traditional concept of surgical lecture is now being challenged and questioned by emerging novel teaching methods [9, 27, 28]. and demands of a new generation of students [17, 18, 27, 29, 30]. One of the major differences between generations Y and Z compared to previous generations is their relationship with technology [2, 10, 31]. This offers an opportunity for medical educators to assess the application, sustainability and relevance of new learning techniques in their classrooms [31–34], as we did in this study. Indeed, the use of digital tools in combination with in-person lectures, known as the “blended learning” technique, can improve the quality of medical education [1, 6, 9, 19, 30, 35]. Educational videos will have a prominent role in modern medical education, starring in many blended and online lectures [13–16, 18, 21]. Well-designed videos may be used by educators, ultimately reducing the time needed to create high-quality educational content [11, 14, 16, 36]. The novelty of our study is that we applied this new teaching format to abdominal surgery.
The paradigm of 21st -century learning is shifting from an educator-centric to a learner-centric model [13]. From the point of view of the medical students, traditional learning needs the implementation of novel tools, e.g. educational videos, and teachers are increasingly forced to become familiar with such novel technologies to provide high quality lectures. However, for many academic educators, teaching is just one task among many others. An increased administrative load, more involvement in research and pressure to be clinically productive has led to a higher demand on academic faculty members. This has resulted in less time being spent on teaching [1, 9, 37]. The SARS-CoV-2 pandemic has further forced medical schools to quickly shift from in-person to E-learning teaching methods.
Nowadays, medical students wish to have customized learning materials, accessible from anywhere, at any time. The students in this study mainly used the PowerPoint slides and their own notes for revision of the lectures, while scientific books and internet videos were rarely used. This showed that students prioritize using resources directly linked to the lecture they attended that is related to several reasons. First, the examination questions at Lausanne’s medical school are created by the teacher who gives the respective lecture. Second, students only have four weeks to prepare for their examinations, and they may not have time using resources not directly linked to the lecture. Even if internet videos and other resources may be much better adapted to their learning styles, the risk of spending time studying something not likely to be tested is too high, as shown in other studies [1, 5].
Medical school teaching is often influenced by external factors such as the curriculum and examination organization. The use of E-learning platforms could help avoid superficial learning and allow students to deepen their knowledge [38, 39]. In this study, the long-term effects of this intervention on learning were not examined. It would be interesting if students who studied with the videos took a second examination several months after their participation in the study, to examine the long-term effect of studying with the videos compared to without. According to the literature, lower performing students benefit the most from blended learning approaches including educational videos and reported higher satisfaction in their learning process [6, 40].
In addition, to the bias brought on by the MCQ examination format, this study has some other limitations. There might be a potential selection bias and results may not be generalizable to other settings. Also, response rate to the final satisfaction survey were low for both groups, most likely because answering these surveys was optional and had no influence on the final grade. However, views of the videos increased from 215 times (V1) to 436 times (V2). Another potential bias why there was no significant increase in correct answers to the MCQ could by the fact that the examination for the V0 cohort took place online, due to the COVID-19 pandemic, while V1 and V2’s examinations were in person. Students taking the examination online at home may have had lower stress levels, consequently resulting in a higher number of correct answers.
Further studies are warranted in which blended-learning lectures are directly compared in parallel to classical in-person lectures, measuring outcome using an objective examination system. This would help advance our understanding of the modern student’s needs and learning styles, as well as their connection with new technologies. Furthermore, a more accurate way to objectively measure the utility of videos is needed. This could be done using an examination specifically created for the study, not only containing MCQs, but also open-ended questions.
Conclusions
In conclusion, this study supports the evidence that medical students demand novel methods including short, animated videos. Videos should be customized to the individual lecture and should be best shown immediately after the corresponding lecture and made available online thereafter. Students used such videos most frequently within four weeks before the multiple-choice examination. In the future, such videos could also be used to preparing lectures and increasing digital learning experiences. Future research should track long-term retention of knowledge and experimental designs to compare the effectiveness of various types of video content.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Engels PT, de Gara C. Learning styles of medical students, general surgery residents, and general surgeons: implications for surgical education. 2010;6.10.1186/1472-6920-10-51PMC 290997420591159 · doi ↗ · pubmed ↗
- 2Dufour J-C, Emeric A, Giorgi R, Université A-M. Interactive Videos within an e-Learning Context.:1.27071891 · pubmed ↗
- 3Vogelsang M, Rockenbauch K, Wrigge H, Heinke W, Hempel G. Medical Education for Generation Z: Everything online?! – An analysis of Internet-based media use by teachers in medicine. GMS Journal for Medical Education; 35(2):Doc 21 [Internet] 2018 [cited 2022 Apr 17];Available from: http://www.egms.de/en/journals/zma/2018-35/zma 001168.shtml 10.3205/zma 001168 PMC 602258129963611 · doi ↗ · pubmed ↗
- 4Guze PA. Using technology to meet the challenges of medical education.:11.PMC 453072126330687 · pubmed ↗
- 5Luke K. How to create effective instructional videos. 2020 [cited 2022 Apr 15]; Available from: http://rgdoi.net/10.13140/RG.2.2.20274.94404
- 6Marshall AL, Wolanskyj-Spinner A. COVID-19: Challenges and Opportunities for Educators and Generation Z Learners. Mayo Clinic Proceedings. 2020;95(6):1135–7.10.1016/j.mayocp.2020.04.015PMC 716757032376100 · doi ↗ · pubmed ↗