Role of clinical pharmacist in ensuring safe medication practices for pediatric cardiac care in low- and middle-income countries
Aniqa Batool, Rumana Sangi, Jibran Bin Yousuf, Abdul Sattar Shaikh, Muhammad Mohsin

TL;DR
This study shows that clinical pharmacists help reduce medication errors in pediatric cardiac care in low- and middle-income countries like Pakistan.
Contribution
The study evaluates the impact of clinical pharmacist interventions on medication safety in a pediatric cardiac care setting in Pakistan.
Findings
260 pharmacist interventions were observed among 2754 patients over eight months.
Antibiotics were the most frequent source of prescription errors, accounting for 81% of interventions.
Abstract
Medication safety is critical for pediatric cardiac care, especially in low- and middle-income countries (LMICs), where limited resources contribute to high rates of medication errors. Studies in LMICs have shown that pharmacist interventions can reduce medication errors by up to 57% and proved that clinical pharmacists are essential for ensuring accurate and optimized medication use. This study aims to evaluate the role of clinical pharmacist interventions to rectify prescription errors in a pediatric cardiac care setting in Pakistan. This single-center retrospective study was conducted from January to August 2022 in a pediatric cardiac ward at the National Institute of Cardiovascular Diseases. Pediatric patients of all age groups and genders diagnosed with acquired, inherited, or congenital heart diseases were included. We reviewed patient files for any prescription changes made by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
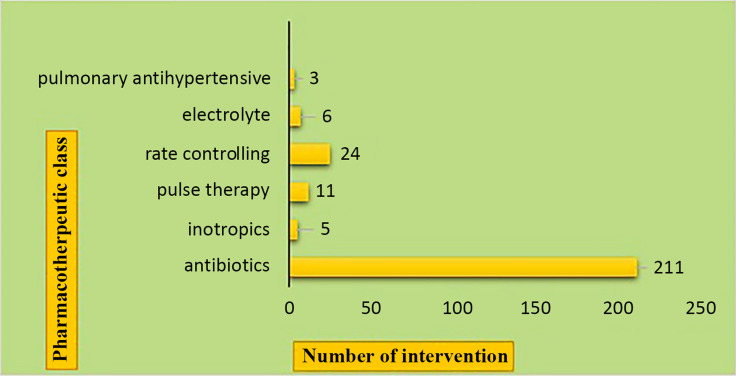 Figure 1
Figure 1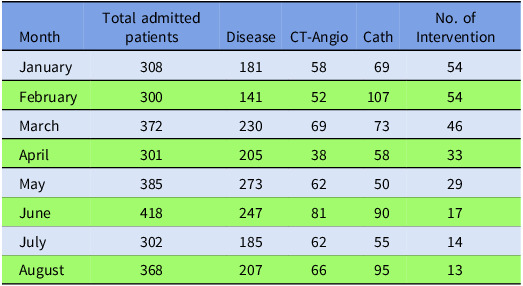 Figure 2
Figure 2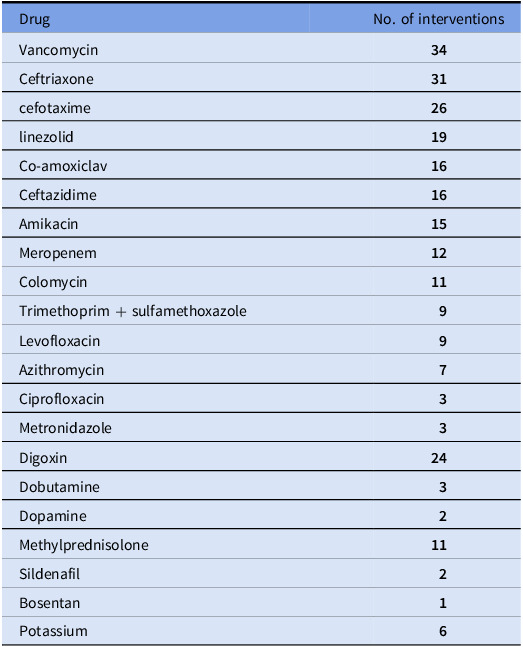 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Failure Treatment and Management · Pneumonia and Respiratory Infections · Pharmaceutical studies and practices
Introduction
Globally, the prevalence of congenital heart disease (CHD) ranges from 4 to 50 per 1,000 live births, while in Pakistan, it is reported to be 3.4 per 1,000 live births. However, specific data on the prevalence of inherited cardiac diseases in Pakistani children remain limited. Furthermore, the prevalence of acquired heart conditions varies based on regional health factors.^1^ Pediatric cardiac disorders include congenital heart disease, arrhythmias, cardiomyopathies, valve disease, aneurysms, and cardiac inflammatory diseases (eg, pericarditis and myocarditis).^2–4^ Effective treatment includes a comprehensive, multidisciplinary approach, medical therapy, nutritional, developmental, and psychosocial support.^3,5^
Clinical pharmacist is important in optimizing pharmacotherapy in pediatric cardiac care, in developing countries.^6^ A systematic review of pharmacist-led interventions in LMICs revealed a 57% reduction in medication errors.^7^ Another study conducted in pediatric settings showed a decline in prescribing mistakes by up to 35%, particularly with antibiotics, antiepileptics, and cardiovascular drugs.^8^ These findings underscore the need for pharmacists to ensure the optimal use of medications. However, in Pakistan, this service remains limited due to a shortage of trained clinical pharmacists with expertise in managing medications for the pediatric cardiac population,^9^ especially in public-sector hospitals. In contrast, such services are predominantly available in private-sector hospitals.^10,11^
In this context, our study aims to address this gap by evaluating the role of clinical pharmacists in identifying and rectifying medication prescription errors in a pediatric cardiac care setting at a public hospital in Pakistan. The findings of this study will underscore the critical role of pharmacists in optimizing medication therapy in pediatric cardiac patients within public-sector settings in LMICs, particularly for this vulnerable population.
Figure 1.Prescription errors in the pharmacological categorical class identified and rectified by clinical pharmacist.
Methods
Study overview: This is a retrospective clinical pharmacist experience on intervention over eight months (January to August 2022) on 2754 Pediatric cardiac patients admitted at the National Institute of Cardiovascular Disease (NICVD), Karachi, Pakistan. Probability consecutive sampling was employed to select the study participants from Pediatric cardiac patients admitted to the pediatric cardiac ward.
Ethics approval and consent to participate: This study was approved by the ethical review committee of the NICVD, Karachi, Pakistan with IRB-No. 39/2024. Due to the retrospective clinical experience nature of the study, ERC waived the patient’s consent.
Procedure: As a routine practice, clinical pharmacists were assigned to the pediatric cardiac ward. Their activities included reviewing patient profiles, confirming diagnoses, recording weight and height, evaluating treatment regimens, and interpreting laboratory results. Prescriptions were checked by calculating doses according to weight, frequency, and duration of therapy, and identifying the same pharmacotherapy medication regimen.^12^ When medication prescription errors were identified, the clinical pharmacist coordinated with the attending medical doctor to modify or change the prescription.^13^ The interventions were on the wrong dose, wrong frequency, incorrect duration of treatment, and unnecessary medication coverage.
Data Collection: We reviewed the patient file for any alteration or re-evaluation of prescriptions by the clinical pharmacist to the physician’s prescriptions based on a comprehensive review of the patient profile, assessment of treatment regimens, and interpretation of laboratory results to ensure safe and effective pharmacotherapy.
Statistical Analysis: Data were analyzed using the Statistical Package for Social Science Version 19. Data were summarized with the help of appropriate statistical measures such as mean ± standard deviation were reported for continuous variables and frequency (percentages %) was computed for the categorical variables.
Results
Overview
A clinical pharmacist observed 260 interventions in this study, with the number of interventions gradually declining over time, as shown in Table 1. Table 2 demonstrates the total number of interventions observed by the clinical pharmacist in rationalizing the medication therapy within eight months.
Table 1.Number of interventions per monthMonthTotal admitted patientsDiseaseCT-AngioCathNo. of InterventionJanuary308181586954February3001415210754March372230697346April301205385833May385273625029June418247819017July302185625514August368207669513
Table 2.Medication error prevention by pharmacist intervention in the pediatric cardiac wardDrugNo. of interventionsVancomycin34Ceftriaxone31cefotaxime26linezolid19Co-amoxiclav16Ceftazidime16Amikacin15Meropenem12Colomycin11Trimethoprim + sulfamethoxazole9Levofloxacin9Azithromycin7Ciprofloxacin3Metronidazole3Digoxin24Dobutamine3Dopamine2Methylprednisolone11Sildenafil2Bosentan1Potassium6
Types of interventions
The nature of clinical interventions included wrong dose: 126 interventions, wrong frequency: 101 interventions, same coverage: 23 interventions, days of therapy: 8 interventions, and both wrong dose and frequency: 2. The most frequent prescription errors were associated with the use of antibiotics (vancomycin, ceftriaxone, cefotaxime, ceftazidime, co-amoxiclav, linezolid, and amikacin), involving incorrect dose, frequency, or duration of therapy.
Discussions
Globally, congenital heart disease (CHD) is the most common congenital anomaly associated with child mortality. The risk of medication errors heightens treatment complexity in CHD, necessitating stringent evaluation and management strategies.^14^ This study highlights the pivotal role of clinical pharmacists in ensuring safe medication use among pediatric cardiac patients in LMICs. The observed reduction in medication errors following pharmacist interventions highlights the need to integrate clinical pharmacy services into multidisciplinary teams to enhance medication safety and patient outcomes in pediatric cardiac care.
Our study corroborates with the findings, particularly in reducing antibiotic-related errors, which account for the highest proportion of prescribing errors in pediatric care globally. Given that antibiotics are often overprescribed or misused in LMICs, pharmacist-led interventions represent a critical step toward antimicrobial stewardship. For instance, research in Nigeria showed that pharmacist participation in multidisciplinary teams reduced inappropriate antibiotic use by 27% over one year^15^ whereas, in our study 10% reduction in inappropriate use of antibiotics.
Our findings are consistent with previous research by Elhabil et al., which identified 309 drug-related problems (DRPs) in 87 patients.^16^ In the present study, clinical pharmacists identified and resolved 260 DRPs among 2,754 pediatric cardiology patients over eight months. Similarly, a study conducted in Ethiopia reported that dosing errors were the most frequent issue, accounting for 37% of identified problems.^17^ In our study, dosing errors constituted the majority of interventions, with 48.5% of errors resolved by clinical pharmacists, highlighting their critical role in addressing medication safety concerns.
Studies have shown that pharmacist interventions in adult populations reduce medication errors, improve adherence, and enhance therapeutic outcomes,^18^ suggesting that similar benefits can extend to pediatric care. This study underscores the critical role of clinical pharmacists in optimizing medication use for vulnerable pediatric populations and highlights the need to integrate clinical pharmacy services into multidisciplinary teams to enhance medication safety and patient outcomes in pediatric cardiac care.
Despite these promising results, our study has several limitations. It is a single-center study, and the absence of a comparator group limits the generalizability of the findings. Additionally, the lack of full-time pharmacist involvement restricted comprehensive monitoring of adverse events, evaluation of hospitalization costs, food-drug and drug-drug interactions, review of discharge medication prescriptions, and assessment of emergency room visits. These constraints highlight the need for further research with robust study designs and expanded pharmacist involvement to fully elucidate the impact of clinical pharmacist interventions on patient outcomes.
Conclusion
Clinical pharmacist intervention in pediatric cardiac care within LMICs, particularly in Pakistan, is an emerging field that holds significant promise for improving medication management and patient outcomes. While this study provides preliminary evidence of its potential benefits, it also underscores the critical shortage of trained clinical pharmacists in the region. This shortage may lead to suboptimal medication therapy and an increased risk of adverse events for pediatric cardiac patients. Although the results are promising, further research and a broader implementation of clinical pharmacy services are essential to confirm and expand upon these findings.
Call to action for stakeholders to support and invest in pharmacist intervention programs
-
Analyzing the barriers to access to trained clinical pharmacists in pediatric cardiac care in LMICs and potential solutions to address this shortage.
-
Awareness regarding the importance of collaboration between healthcare providers, pharmacists, and other stakeholders to enhance patient safety and quality of care.
-
Examining successful pharmacist intervention programs implemented in other healthcare systems and how they could be adapted to benefit patients in LMICs.
-
Investigating the role of technology and telemedicine in bridging the gap between patients, healthcare providers, and pharmacists in resource-limited settings for improved medication therapy management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van Der Linde D , Konings EE , Slager MA , Witsenburg M , Helbing WA , Takkenberg JJ , et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 2011;58:2241–2247.22078432 10.1016/j.jacc.2011.08.025 · doi ↗ · pubmed ↗
- 2Jaarsma T , Haaijer-Ruskamp FM , Sturm H , Van Veldhuisen DJ . Management of heart failure in The Netherlands. Eur J Heart Fail 2005;7:371–375.15718177 10.1016/j.ejheart.2005.01.007 · doi ↗ · pubmed ↗
- 3Rao PS . Management of congenital heart disease: state of the art—part II—cyanotic heart defects. Children 2019;6:54.30987364 10.3390/children 6040054 PMC 6518252 · doi ↗ · pubmed ↗
- 4Arshad MS , Anwar-ul-Haq HM , Adnan M , Zulqarnain A . Frequency and pattern of paediatric heart diseases: five years experience at the children’s hospital, Multan. Pak J Med Sci 2020;36:1308.32968399 10.12669/pjms.36.6.2312 PMC 7501000 · doi ↗ · pubmed ↗
- 5Dunn SP , Birtcher KK , Beavers CJ , Baker WL , Brouse SD , Page RL , et al. The role of the clinical pharmacist in the care of patients with cardiovascular disease. J Am Coll Cardiol 2015;66:2129–2139.26541925 10.1016/j.jacc.2015.09.025 · doi ↗ · pubmed ↗
- 6Hailu BY , Berhe DF , Gudina EK , Gidey K , Getachew M . Drug-related problems in admitted geriatric patients: the impact of clinical pharmacist interventions. BMC Geriatr 2020;20:1–8.10.1186/s 12877-020-1413-7PMC 695857931931723 · doi ↗ · pubmed ↗
- 7Babar Z-U-D . Ten recommendations to improve pharmacy practice in low and middle-income countries (LMI Cs). J Pharm Policy Pract 2021;14:6.33407945 10.1186/s 40545-020-00288-2PMC 7788796 · doi ↗ · pubmed ↗
- 8Brennan-Bourdon LM , Vázquez-Alvarez AO , Gallegos-Llamas J , Koninckx-Cañada M , Marco-Garbayo JL , Huerta-Olvera SG . A study of medication errors during the prescription stage in the pediatric critical care services of a secondary-tertiary level public hospital. BMC Pediatr 2020;20:1–8.33278900 10.1186/s 12887-020-02442-w PMC 7718655 · doi ↗ · pubmed ↗